

Abstract
Objective. To evaluate the outcome of tumor necrosis factor-α inhibition (anti-TNF) for pediatric uveitis.
Methods. We retrospectively assessed children (age ≤ 18 yrs) with noninfectious uveitis receiving anti-TNF at 5 uveitis centers and 1 pediatric rheumatology center. Incident treatment success was defined as minimal or no uveitis activity at ≥ 2 consecutive ophthalmological examinations ≥ 28 days apart while taking no oral and ≤ 2 eyedrops/day of corticosteroids. Eligible children had active uveitis and/or were taking higher corticosteroid doses.
Results. Among 56 eligible children followed over 33.73 person-years, 52% had juvenile idiopathic arthritis (JIA) and 75% had anterior uveitis (AU). The Kaplan-Meier estimated proportion achieving treatment success within 12 months was 75% (95% CI 62%–87%). Complete absence of inflammatory signs with discontinuation of all corticosteroids was observed in an estimated 64% by 12 months (95% CI 51%–76%). Diagnoses of JIA or AU were associated with greater likelihood of success, as was the oligoarticular subtype among JIA cases. In a multivariable model, compared to those with JIA-associated AU, those with neither or with JIA or AU alone had a 75%–80% lower rate of achieving quiescence under anti-TNF, independent of the number of immunomodulators previously or concomitantly prescribed. Uveitis reactivated within 12 months of achieving quiescence in 14% of those continuing anti-TNF (95% CI 6%–31%). The incidence of discontinuation for adverse effects was 8%/year (95% CI 1%–43%).
Conclusion. Treatment with anti-TNF was successful and sustained in a majority of children with noninfectious uveitis, and treatment-limiting toxicity was infrequent. JIA-associated AU may be especially responsive to anti-TNF.
Uveitis is an important contributor to visual morbidity in children. In Northern California, the annual incidence of uveitis was 7/100,000 among children ≤ 14 years of age and 27/100,000 among adolescents1. In the developed world, most pediatric uveitis cases are undifferentiated or are associated with juvenile idiopathic arthritis (JIA; 13%–47%)2,3,4,5,6. Across JIA subtypes, 12%–13% of children develop uveitis, although this percentage is much higher among certain subgroups, particularly those who are antinuclear antibody (ANA)-positive7. The uveitis leads to complications in over half of children, including iris synechiae (iris scarring), corneal calcium deposition, glaucoma, cataracts, macular edema, and/or visual loss8,9,10,11. Many complications necessitate surgery. Early and aggressive treatment is needed to prevent the most devastating longterm outcomes12. Even with the broad array of treatments available, the incidence of vision loss (≤ 20/50) is 0.17/person-year13.
Topical corticosteroids are the first line of treatment, but are poorly tolerated in children, leading to early use of second-line immunomodulatory therapies such as methotrexate MTX12. More recently, biologic immunomodulatory agents also have been used, especially tumor necrosis factor-α inhibitors (anti-TNF). Particularly for JIA-associated uveitis, anti-TNF have shown impressive effects regarding control of inflammation and improvement of visual acuity in small, single-center observational studies14,15,16,17,18,19,20,21,22,23,24. Definitions of success varied by study, making comparisons across these small studies impractical.
Whether certain patients are better suited to treatment with anti-TNF is unknown. Because anti-TNF treatment is costly, it would be important to identify whether particular factors are associated with response to these agents, yet this has not been investigated. Because some studies have suggested that children with JIA-associated uveitis have worse visual outcomes than those with non-JIA–associated uveitis25, we hypothesized that children with JIA might respond less well to anti-TNF. Further, in JIA-associated uveitis, certain factors have been associated with an increased likelihood of developing severe uveitis or poor visual outcomes. These included male sex4, nonwhite race13, younger age at onset4,7, oligoarticular JIA11, ANA positivity7,13, complications at presentation4,9,13,26, and intermediate, or posterior, rather than anterior, uveitis (AU)3,4,6. We hypothesized that these factors also might be associated with worse response to anti-TNF. To address these questions, we assembled a relatively large multicenter cohort of children with uveitis receiving anti-TNF treatment begun while the uveitis was active or else required an unsustainable dose of corticosteroids to maintain quiescence. We wished to examine the outcomes of anti-TNF therapy and to identify variables positively or negatively associated with achieving control of uveitis with minimal or no use of corticosteroids.
MATERIALS AND METHODS
Study setting and study population
This was a retrospective cohort study of patients from 5 uveitis subspecialty centers participating in the retrospective Systemic Immunosuppressive Therapy for Eye Disease (SITE) Cohort Study combined with patients managed in the rheumatology and ophthalmology practices of The Children’s Hospital of Philadelphia (CHOP) during the anti-TNF era (1999–2010; SITE: 1999–2007; CHOP: 2004–2010). At SITE centers, data had been collected from all available medical records of every patient with noninfectious uveitis27,28. Additional subjects were identified by searching the CHOP electronic medical record system for International Classification of Diseases, 9th ed. (ICD-9) codes possibly indicating noninfectious uveitis (ICD-9 363.x, 364.x)1. The charts of patients thus identified, who presented for care between 2000 and 2010, were reviewed to determine whether they had uveitis and whether ophthalmologic records were available.
Inclusion criteria
Subjects selected for this analysis were ≤ 18 years old at the time of initiation of anti-TNF treatment and either had active uveitis or slightly active/inactive uveitis controlled by systemic and/or topical corticosteroids, > 2 drops/day. Anti-TNF therapies included infliximab, etanercept, and adalimumab. Concomitant treatment with corticosteroids and/or MTX, azathioprine, mycophenolate mofetil, or cyclosporine was recorded. A subject was included only if uveitis activity status was available within 30 days prior to anti-TNF initiation and for ≥ 2 visits after treatment initiation (the minimum followup required to meet the success definition). If a subject had more than 1 treatment course with anti-TNF that met inclusion criteria (drug episode) and success never was achieved with the first anti-TNF treatment course, that subject could be included in the cohort more than once. As per survival analysis, which measures time-to-event, person-time after an event could not be included. Drug episodes discontinued during the first infusion were not included.
Data collection
Protocol-driven retrospective paper chart reviews had been performed at the 5 SITE centers, and data were entered into an electronic database created for the SITE Cohort Study. At CHOP, data were obtained from electronic medical or paper records through the divisions of rheumatology and/or ophthalmology and were entered into a simplified version of the SITE database addressing the outcomes of interest for this study. Paper charts included clinic notes from both CHOP-affiliated and community ophthalmologists. The CHOP subcohort of patients with JIA were characterized further into subtypes according to the International League of Associations for Rheumatology (ILAR) criteria29. Age at uveitis was dichotomized (≤ 6 vs > 6 yrs), following the American Academy of Pediatrics ophthalmologic screening guidelines for children with JIA30. ANA status and whether uveitis involved pain/redness/photosensitivity at the onset were data available only from the CHOP subcohort.
Definition of disease activity/location
Disease activity at each visit was characterized as an ordered categorical outcome, using the approach the SITE Cohort Study has used previously: inactive, slightly active, or active, incorporating information from sites of inflammation other than the anterior chamber (AC) into a single activity variable31,32,33,34,35. Categories closely parallel the uveitis definitions of the Standardization of Uveitis Nomenclature Working Group36,37. Chart reviewers ascertained disease status from the physician’s overall assessment at the visit through the use of descriptors such as quiet or quiescent, as well as quantitative descriptors of cell grade and vitreous haze. “Inactive” indicated designations such as no cells, rare cells, no vitreous haze, and no corticosteroids; “slightly active” indicated gradings such as trace or fewer AC cells (≤ 0.5+) and minimal vitreous haze or cells; and “active” indicated higher levels of inflammation. Disease state was recorded by eye; a patient’s disease state was considered as the worse level of the 2 eyes if both had uveitis or else the level of the eye with uveitis for unilateral cases. Uveitis location was categorized as anterior, intermediate (± anterior), posterior, or panuveitis36.
Outcome definitions
The primary outcome (success) was defined as achieving either “slightly active” or “inactive” uveitis status as assessed by the evaluating ophthalmologist while on ≤ 2 drops/day topical corticosteroids and no oral corticosteroids. Success was evaluated secondarily in the most restrictive fashion, as the complete absence of inflammatory signs (“inactive”) while taking no topical or oral corticosteroids. Only “successes” documented over ≥ 2 visits spanning ≥ 28 days were counted, to avoid counting transient control of inflammation as a success31,32,33,34,35.
Discontinuation of therapy
The reason for discontinuation of anti-TNF was coded as ineffective, remission, missing, or adverse effects.
Followup time
Followup time began with the first visit at which an anti-TNF was prescribed (subcutaneous etanercept or adalimumab) or from the first day of intravenous administration (infliximab). Only treatment courses initiated under observation during the study period were included. Visit frequency varied, and for survival analyses, data were used from clinical visits while a subject was on therapy until uveitis quiescence. Uveitis information was collected from all available visits to an ophthalmologist. Time to success was measured to the first of the 2 sequential visits necessary for success. Censoring occurred when the anti-TNF was discontinued (in order not to attribute success to a subsequent drug) or the subject was lost to followup without achieving quiescence before the end of observation. In a secondary analysis of time to reactivation while on anti-TNF, analysis time began when a subject achieved quiescence; each subject was followed through uveitis reactivation, drug discontinuation, or loss to followup.
Covariates
Variables evaluated for their association with treatment success (achievement of quiescence) are listed in Table 1.
Characteristics of children with inadequately controlled uveitis starting tumor necrosis factor-α inhibitor therapy.
Data analysis
Data were analyzed using Stata 11.0. Differences in categorical demographic and clinical characteristics between subcohorts were assessed using the chi-square test. Nominal statistical significance was defined as a 2-tailed p value ≤ 0.05. Kaplan-Meier methods evaluated time to success. Because a subject could have more than 1 drug episode, analyses were performed using a robust variance estimator to account for clustering by subject. Cox proportional hazards model-derived HR were used to estimate the association of each independent patient-level or treatment-level variable with each outcome variable. When subjects discontinued treatment because of an adverse event or failure, they were no longer considered “at risk” for succeeding under that drug. Consequently a competing risks analysis was performed using proportional subhazard regression (Stata “stcrreg” command)38. For variable selection in multivariable regression, a variable was included if it was significant at the 0.1 level. Two-way interactions were assessed for variables that were statistically significant in the unadjusted analysis; an interaction was said to exist if it was significant at the 0.05 level. To account for possible differences between CHOP versus SITE, subcohort was included as a covariate.
The institutional review boards of the participating centers approved the SITE Cohort Study. The institutional review boards of CHOP and the University of Pennsylvania approved our study.
RESULTS
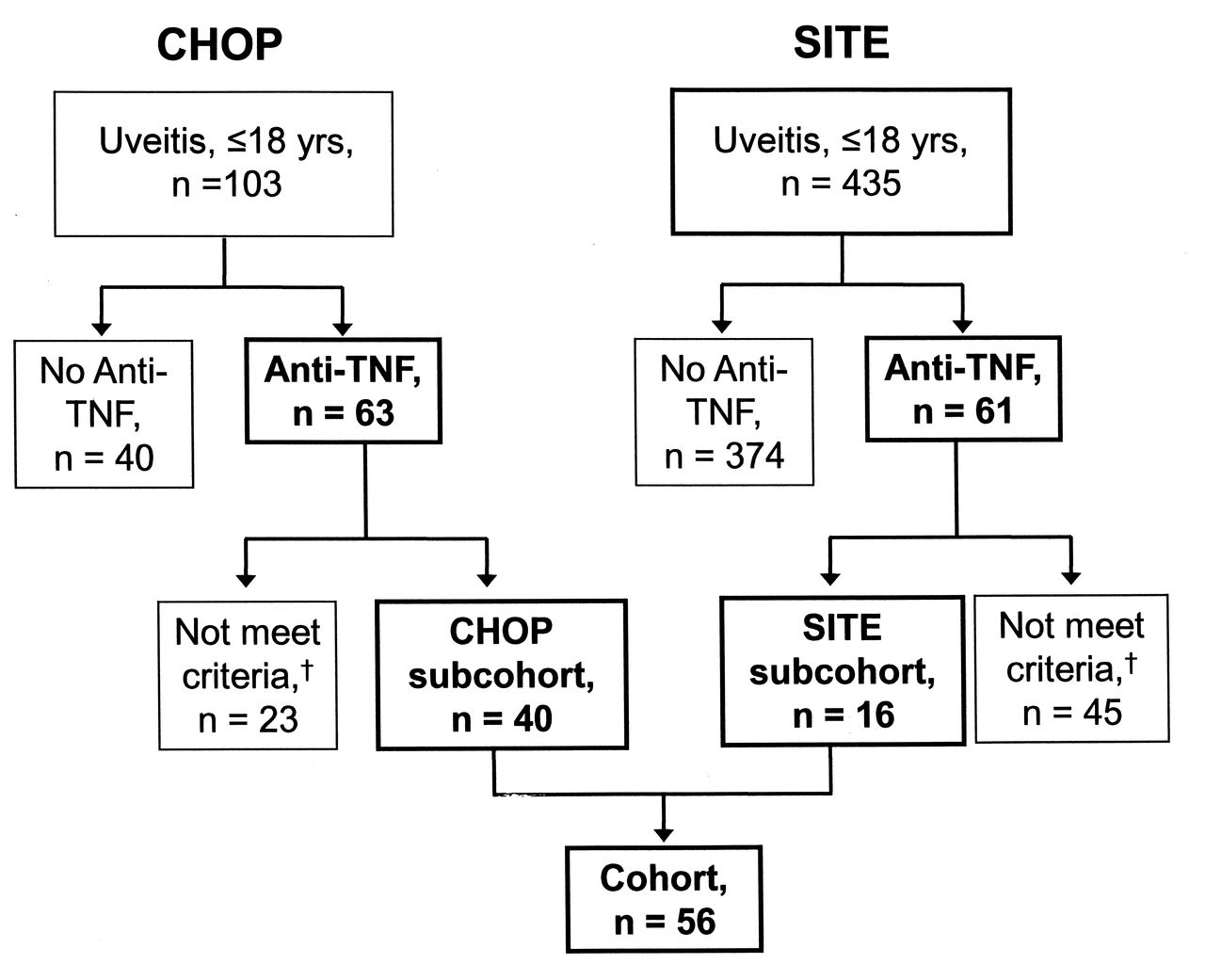
The records of 538 children (ages 18 yrs or younger) with uveitis were evaluated for inclusion in this cohort (Figure 1). Of those, 103 children at CHOP and 435 children in the SITE Cohort were treated for noninfectious uveitis. Overall, 23% of the children diagnosed with uveitis in childhood were treated with anti-TNF. At CHOP, 63 children were treated with anti-TNF; only 40 met inclusion criteria. In the SITE Cohort, 61 children received anti-TNF; only 16 of them met inclusion criteria. The age, race, and sex distributions were similar between those included and those excluded from the cohort because of missing data (data not shown). The 56 children who met inclusion criteria and had adequate followup information to be “at risk” of quiescence were followed over 33.73 person-years (median 0.26, range 0.04–4.12 person-yrs/patient).

Study cohorts. Of 538 patients treated for noninfectious uveitis, 124 were treated with anti-tumor necrosis factor-α (anti-TNF). Of those, 56 met inclusion criteria for anti-TNF/corticosteroid/immunomodulatory therapy use. †Sixty-eight subjects were excluded (23 potential subjects from CHOP and 45 from SITE) because of inadequate records (did not have a visit within 30 days prior to initiation of anti-TNF, no documentation of uveitis status at onset of anti-TNF therapy, uveitis developed after starting anti-TNF, or initiation of anti-TNF after the cutoff for the study). SITE: Systemic Immunosuppressive Therapy for Eye Disease Cohort Study; CHOP: The Children’s Hospital of Philadelphia.
Baseline characteristics of the cohort
Subject characteristics are described in Table 1. The ILAR subtype of JIA and ANA status was available only from CHOP. Subjects from CHOP and SITE were balanced in most baseline characteristics, except that at CHOP, a lower proportion of children were diagnosed at ≤ 6 years of age (40% vs 89%), more were treated with MTX (98% vs 29%), but fewer were treated with ≥ 2 conventional immunomodulators (7% vs 47%) before anti-TNF, and a lower proportion had an underlying diagnosis of JIA (43% vs 75%). Only 5% of children in the overall cohort began anti-TNF prior to failing ≥ 1 other immunomodulatory agent. In addition to corticosteroids and MTX (n = 44), children had been treated previously with cyclosporine (n = 13), mycophenolate mofetil (n = 12), chlorambucil (n = 2), and cyclophosphamide (n = 1).
Treatment characteristics
Subjects from CHOP had a shorter time between diagnosis of uveitis and anti-TNF treatment relative to subjects from SITE (median 0.32 vs 4.25 years) and fewer of them were treated with the soluble TNF receptor (etanercept) than with monoclonal anti-TNF antibodies (infliximab or adalimumab; 10% vs 47%; Table 1). Children with sarcoidosis-associated uveitis had been treated with infliximab (n = 5) or adalimumab (n = 1).
Of the subjects with known anti-TNF dose information (n = 40, from CHOP), 35 were treated with infliximab; all but 1 began treatment on an every 4-week schedule after drug loading. Subjects had a median starting dose of 9.3 mg/kg (range 4.5 to 13.3 mg/kg); only 5 subjects were treated with doses < 7 mg/kg. All subjects treated with adalimumab received 40 mg every other week. Subjects taking etanercept received 12.5–25 mg twice weekly, except for 1 young child who received 0.8 mg/kg weekly. Three subjects initiated treatment with anti-TNF on 2 occasions that met inclusion criteria for the final analysis. In each case, the initial drug was etanercept, which was discontinued for failure (n = 2, CHOP) or unknown reasons (n = 1, SITE); none were successful while taking their second drug, infliximab.
Response to anti-TNF treatment
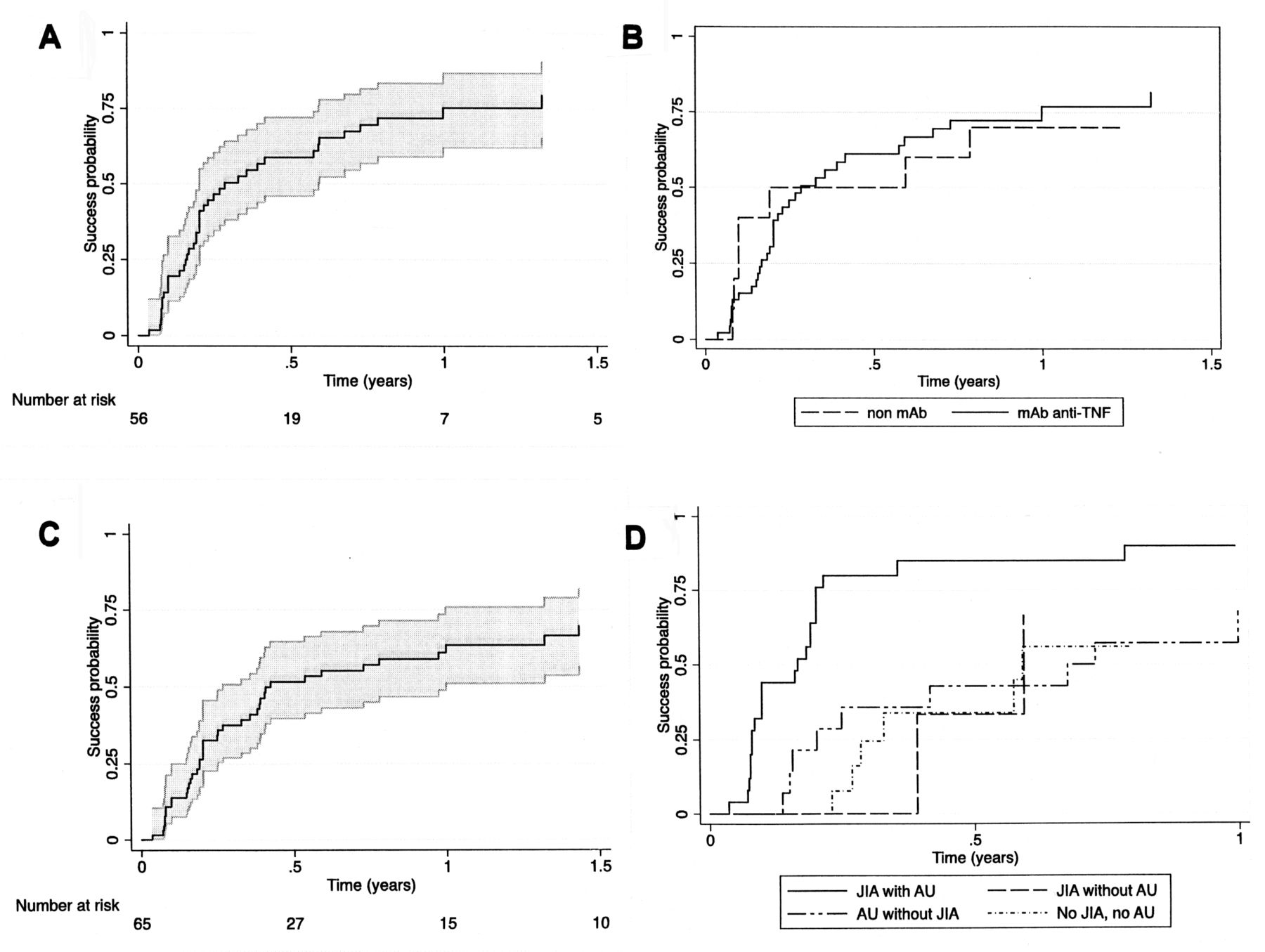
The estimated proportion who achieved treatment success that was then sustained for at least 28 days within 12 months was 75% (95% CI 62%–87%; Figure 2A). The estimated probability of a child achieving quiescence was 47% by 3 months (95% CI 35%–60%) and 59% by 6 months (95% CI 46%–72%); the median time to success was 3.4 months. The cumulative incidence of success did not differ significantly between subcohorts (p = 0.37); treatment success at 12 months was 79% (95% CI 63%–91%) and 68% (95% CI 44%–89%) in the CHOP and SITE subcohorts, respectively. The cumulative incidence of success did not differ significantly between those treated with different classes of anti-TNF agents (monoclonal anti-TNF antibodies vs nonmonoclonal antibody; p = 0.55); treatment success at 12 months was 0.77 (95% CI 0.62, 0.89) vs 0.70 (95% CI 0.32, 0.93; Figure 2B). Most of these also met the higher standard of complete uveitis inactivity without concomitant topical or oral corticosteroids, 34% by 3 months (95% CI 24%–47%), 52% by 6 months (95% CI 40%–65%), and 64% by 12 months (95% CI 51%–76%; Figure 2C). Sensitivity analysis including only 1 drug episode per subject did not alter results qualitatively.
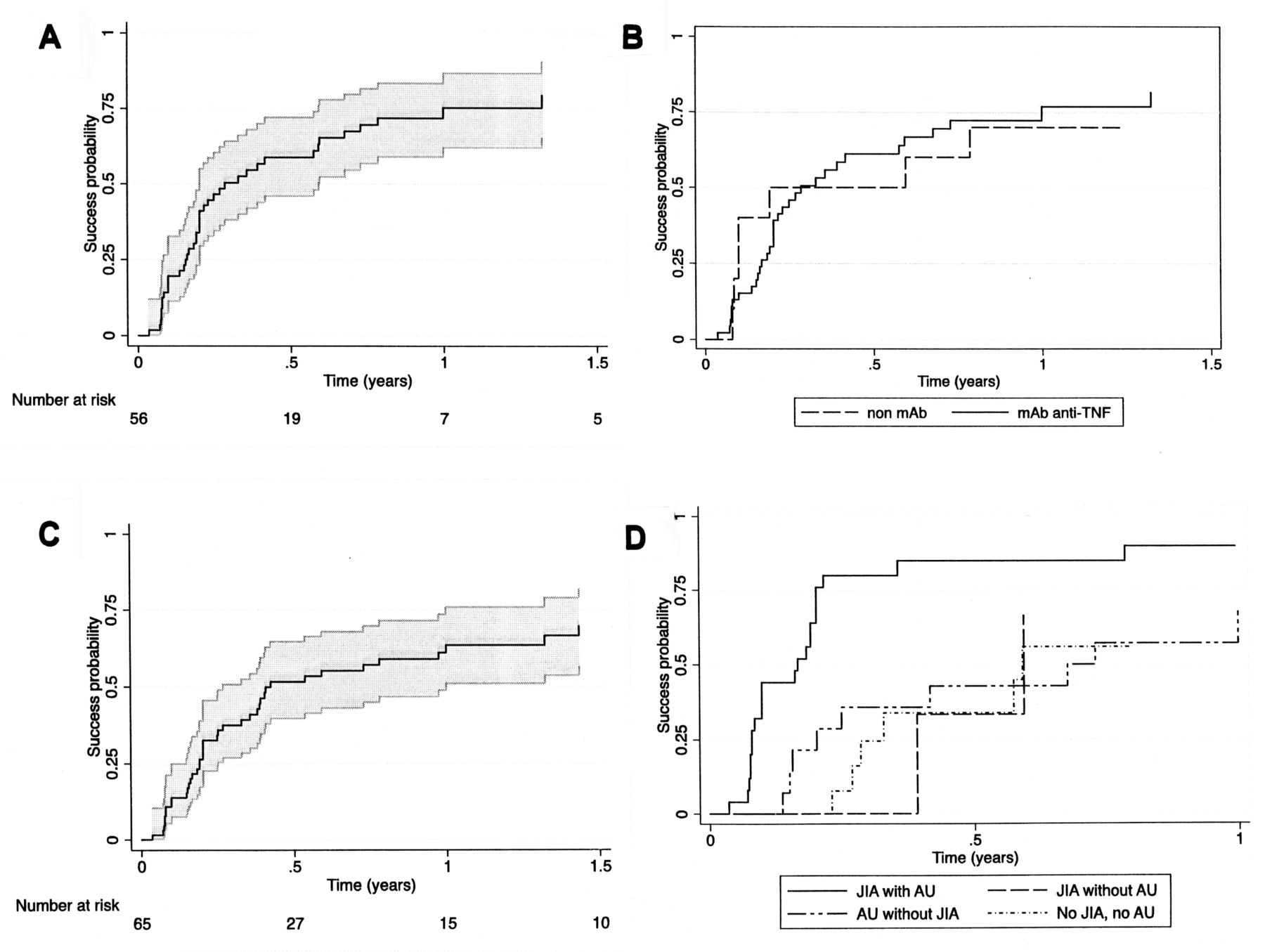
Time-to-treatment success following initiation of anti-TNF in children with uveitis. Areas shaded in gray represent the 95% CI. A. “Slightly active” (trace or fewer anterior chamber cells (≤ 0.5+) or better control of inflammation in all eyes with uveitis absent use of oral corticosteroids and with no more than 2 drops/day of topical corticosteroids. B. “Slightly active” in children treated with monoclonal antibody anti-TNF (infliximab or mAb) versus those treated with etanercept. C. Complete uveitis inactivity without concomitant topical or oral corticosteroids. D. “Slightly active” or better control of inflammation in different subgroups of children with uveitis; treatment success over time is demonstrated in subgroups determined by their juvenile idiopathic arthritis (JIA) and anterior uveitis (AU) statuses.
Factors predictive of treatment success
Diagnoses of JIA (HR 2.41, 95% CI 1.29–4.56) and AU (vs intermediate, posterior or panuveitis, HR 2.52, 95% CI 1.35, 4.69) each were associated with faster development of quiescence (Table 2). Within the CHOP subcohort, children with oligoarticular JIA (vs other forms of JIA) had a higher rate of treatment success (HR 5.93, 95% CI 2.15–16.36). No other variables were significantly associated with treatment success. Results from the competing risks analysis were similar to those from standard proportional hazards analysis.
Factors associated with tumor necrosis factor-α inhibitor treatment success.
Conjoint analysis of the effects of JIA and AU on treatment success, adjusted for subcohort, revealed that compared to patients with JIA-associated AU, the rate of success was 75%–80% lower in patients with neither JIA nor AU, or with either one alone (Table 3). The Kaplan-Meier estimate of the proportion with treatment success by 6 months in those with JIA-associated AU was 0.85 (95% CI 0.68–0.96) versus 0.37 (95% CI 0.23–0.58) for the other 3 groups combined (Figure 2D).
Multivariable hazard ratios for treatment success variables under tumor necrosis factor-α inhibitors. Covariates included in the multiple regression model: diagnoses of juvenile idiopathic arthritis (JIA) and anterior uveitis (with interaction between the 2) and source of data (Children’s Hospital of Philadelphia subcohort vs Systemic Immunosuppressive Therapy for Eye Disease Cohort Study). Referent is different from that in Table 2: it is JIA and AU (rather than no JIA, no AU). Data are hazard ratio (95% CI).
Treatment-limiting adverse effects
Eight percent of anti-TNF treatment episodes were discontinued within 12 months because of adverse effects (n = 1; 95% CI 1%–43%). Only 1 subject stopped infliximab before control was achieved (for allergic reaction). Four subjects discontinued medications because of side effects after they had already achieved success: allergic reaction to infliximab (n = 2); side effects to infliximab (n = 1); and side effects to etanercept (n = 1). None of the subjects treated with adalimumab in the cohort stopped therapy because of adverse effects.
Relapse of uveitis during anti-TNF treatment
Among 45 subjects taking anti-TNF agents who initially achieved treatment success, 36 had sufficient followup while continuing to take anti-TNF to observe a relapse of uveitis. The Kaplan-Meier estimates of the risk of relapse while taking anti-TNF by 3, 6, and 12 months were 8% (95% CI 3%–24%), 11% (95% CI 4%–27%), and 14% (95% CI 6%–31%), respectively (Figure 3).

Time to reactivation of uveitis after achieving treatment success (“slightly active” or better control of inflammation in all eyes with uveitis, absent use of oral corticosteroids, and with no more than 2 drops/day topical corticosteroids), while receiving ongoing TNF inhibitor therapy. Area shaded in gray represents 95% CI.
DISCUSSION
Our results suggest that anti-TNF is a useful treatment for pediatric noninfectious uveitis, particularly for patients with JIA-associated AU. Even though 95% of children in our cohort had failed 1 or more prior immunosuppressive drugs, the substantial majority had a favorable or very favorable response to treatment. Although JIA-associated uveitis has been thought to be more treatment-resistant than other forms of pediatric uveitis39, in our study JIA-associated uveitis responded better under TNF inhibition than did other forms of uveitis, such as sarcoidosis-associated or undifferentiated uveitis. As expected, AU responded better than did other types of uveitis31,33, but the benefit seemed to be primarily among those with JIA-associated AU. Suppression was sustained for 12 months in a large majority of cases. Therapy was well tolerated, with a low rate of discontinuation of anti-TNF agents for complications.
While presumably there is overlap of some SITE cohort patients with those described in previous reports15,22,40,41,42, here we describe the outcomes in 56 patients from 6 tertiary care centers, not previously reported together. This is one of the largest pediatric cohorts of anti-TNF therapy for pediatric uveitis to date. Comparisons of response rates with those from prior smaller studies are complicated in that each used different measures of improvement in inflammation, only some of which took into account the degree of corticosteroid usage. Once uveitis is quiet, many ophthalmologists maintain patients on low-dose topical corticosteroids and vary in their attempts to completely discontinue them. If success required complete corticosteroid discontinuation, time to success would be artificially lengthened by clinicians who did not attempt to completely taper corticosteroids. Given the heterogeneous group of ophthalmologists who saw cases in this cohort, we defined quiescence as uveitis inactivity while taking ≤ 2 corticosteroid drops/day for our primary analysis, in addition to reporting complete quiescence while taking no corticosteroid therapy.
Overall, our results confirm the generally favorable results reported in small series. The 3.4-month median time to response is identical to that observed previously15,21,43. It has been hypothesized that the effectiveness of anti-TNF agents may be affected by their mechanism of action, and that monoclonal anti-TNF antibodies (infliximab and adalimumab) may be more effective than the soluble TNF receptor (etanercept). In fact, there was no benefit of etanercept over placebo for uveitis in a small randomized controlled trial40. Later studies suggested that infliximab was more effective than etanercept15,43 and that adalimumab was more effective than infliximab for uveitis44. Although we did not demonstrate a decreased effectiveness of etanercept relative to the other agents, we had limited power to discriminate between the effects of different anti-TNF agents or between monoclonal antibody and soluble TNF receptor anti-TNF agents. In our combined evaluation of anti-TNF agents, quiescence was achieved in 64%–75% by 1 year, depending on the stringency of the definition of quiescence used, which is similar to 2 other studies describing the 1-year outcome of infliximab treatment14,21. Our observation that the cumulative incidence of complete control of inflammation absent all corticosteroids was only slightly lower than a less stringent definition of success permitting low-dose topical corticosteroids suggests that most patients can be tapered off all corticosteroids while under anti-TNF therapy. Had all ophthalmologists practiced tapering more aggressively, perhaps an even higher incidence of success would have been achieved. The percentage of patients who maintained quiescence through 12 months of continued anti-TNF therapy was higher than that in another study (86%, 95% CI 69%–94%, vs 58%, 95% CI 32%–82%)14, possibly because of higher initial infliximab doses (9 vs 5 mg/kg).
Because physicians may choose anti-TNF over other conventional immunomodulators when uveitis is more severe or recalcitrant, success under different treatment types cannot be contrasted directly. However, review of our results alongside historical controls suggests that anti-TNF may be more effective for inflammatory uveitis. Most pediatric studies did not describe the antiinflammatory and topical corticosteroid-sparing effect of immunomodulators in a single statistic45,46,47. Yet in one study of azathioprine for MTX-resistant uveitis, only 29% of children (95% CI 4%–71%) achieved uveitis control on fewer than 2 drops/day of topical corticosteroids48. In the large SITE cohort studies, including patients of all ages with a variety of sites of inflammation, by 1 year, fewer than 20% of individuals achieved control of inflammation while not taking systemic corticosteroids with mycophenolate mofetil, MTX, cyclosporine A, or azathioprine31,32,33,34,35. Thus the more favorable incidence of success in our study, even in a population that had largely failed conventional immunomodulators and using more stringent success criteria, suggests that anti-TNF treatment may be more effective than alternative immunomodulatory drugs.
Little information has been available previously regarding factors predictive of favorable response to anti-TNF. One study of 20 children with JIA demonstrated a positive correlation between response to adalimumab and a younger age at diagnosis and/or a shorter time between uveitis diagnosis and adalimumab treatment49. Our analysis did not confirm these associations. However, we found that children with JIA-associated AU have a particularly favorable prognosis with anti-TNF therapy. Among patients with JIA in the CHOP subcohort, we observed a particularly favorable prognosis for children with oligoarticular JIA. Many animal models of autoimmune uveitis are primarily driven by antigen-specific Th1 cells, yet innate immune cells are also involved50. JIA-associated AU may be more Th1-driven, or specifically TNF-α–driven, than uveitis of other etiologies. Further work is needed to ascertain whether specific blockade of other cytokines (e.g., interferon-γ) or cellular pathways (e.g., Th17) also might be more effective than conventional immunomodulators in non-JIA-associated uveitis.
In previous SITE Cohort reports, the 1-year incidence of discontinuation for toxicity, defined in the same manner as this study, for cyclosporine, mycophenolate mofetil, MTX, azathioprine, and cyclophosphamide, respectively, were 10.7%, 14.5%, 17.5%, 24.1%, and 33.5%31,32,33,34,35. Thus the tolerability profile of anti-TNF was no worse than and may be favorable compared to alternative conventional immunosuppressive agents.
The greatest limitation of our study is its observational design. Because of the absence of a single prospective study protocol, there was variance in the followup schedule, MTX usage patterns, topical corticosteroid tapering approaches, and anti-TNF doses. A number of potential subjects had to be excluded because of missing information. As in any retrospective cohort study, we were unable to assess whether the outcomes of excluded patients were different from those of observed patients. That their demographic and clinical characteristics were similar suggests that the patients studied were likely to be representative of the larger population. Also, because of the variability in followup, improvement may have been mischaracterized as occurring later or initial treatment success may have been overlooked altogether, thus underestimating the proportion achieving quiescence at each timepoint. Further, uveitis treated at these tertiary care centers, and the uveitis treated there with anti-TNF, may have represented a subset of more severe or treatment-refractory disease. If so, our analysis may underestimate the benefits of anti-TNF therapy. However, that patients who had failed a larger number of prior immunomodulatory therapies did not have a lower rate of success suggests that anti-TNF therapy often succeeds even in that context. Because standard survival analysis may overestimate the incidence of a favorable event in the face of informative censoring, as might occur when a drug was switched because an individual failed to respond to the initial anti-TNF, we used a competing risk analysis. While a competing risk analysis is designed to overcome this problem, it is possible that violations of its assumptions may have led to overestimation or underestimation of the time to treatment success.
Our study’s statistical power also was limited to identify associations with variables that were not collected in the SITE cohort (anti-TNF dose, JIA subtype, ANA status, symptomatic uveitis, or joint activity). Because at CHOP few patients had active musculoskeletal disease at cohort entry, we were unable to evaluate the concordance of joint and eye activity in response to treatment. In our study, concomitant anterior and intermediate uveitis was classified as intermediate. Our analysis may underestimate those with AU, thus underestimating the association between AU and response to anti-TNF. While a difference between subcohorts, CHOP versus SITE, is a potential limitation, outcomes did not differ between subcohorts in a sensitivity analysis. Strengths of the study include a sample size large enough to allow substantially more precise estimates of treatment success, time to success, and risk factor associations than previously were available; and the use of quality control measures in the data collection to maximize retrospective data quality.
Our results suggest that anti-TNF medications are often useful for children with uveitis, even in children who have failed other immunomodulatory therapies, and are generally well tolerated. These agents result in a corticosteroid-sparing benefit, likely limiting the ocular toxicities of longterm topical corticosteroid use. Patients with JIA-related AU or patients with oligoarticular JIA-associated uveitis may be especially likely to respond under such therapy, because the large majority of these patients achieve treatment success relatively quickly. Clinical trials evaluating the relative merits of TNF inhibitor therapy versus conventional immunosuppression would be valuable to more thoroughly characterize the extent of any such advantage, but would be difficult to implement. In the meantime, it seems reasonable to recommend the use of anti-TNF therapy relatively early in the management of pediatric uveitis cases that fail an initial conventional immunomodulatory drug, before uveitis or corticosteroid therapy induce severe eye damage.
Footnotes
-
Supported by a Rheumatology Research Foundation Scientist Development Award (Dr. Lerman); Autoimmunity Centers of Excellence, National Institute of Allergy and Infectious Diseases (Dr. Burnham); R01 EY014943 National Eye Institute (NEI), US National Institutes of Health (NIH; Drs. Daniel, Rosenbaum, Suhler, Thorne, and Kempen); grants AG025152 and AG035751 from the National Institute on Aging (Dr. Hennessy); cooperative agreements from the NEI and the NIH to the Mount Sinai School of Medicine (U10 EY08052), the Johns Hopkins University Bloomberg School of Public Health, (U10 EY08057), and the University of Wisconsin (U10 EY08067; Dr. Jabs); intramural funding from the NEI (Dr. Levy-Clarke, and previously, Dr. Nussenblatt); The US Department of Veterans Affairs (Dr. Suhler); research grants from Abbott, LuxBio Genentech, Bristol Myers Squibb, Novartis, EyeGate, and the RPB Sybil B. Harrington Special Scholars Award (Dr. Thorne); and Research to Prevent Blindness, and the Paul and Evanina Mackall Foundation (Dr. Kempen).
- Accepted for publication May 9, 2013.








{kind=link}
{kind=link}
{kind=link}