

Abstract
Objective. Previous studies indicated that pyridinoline, a collagen crosslink in cartilage and bone, might be a good marker to predict joint destruction in patients with rheumatoid arthritis (RA), although large prospective studies are lacking. We evaluated the predictive value of serum pyridinoline levels for joint destruction, both at baseline for longterm prediction and during the disease course for near-term prediction.
Methods. Patients with early RA from the Leiden Early Arthritis Clinic were studied. Radiographs at baseline and yearly during 7 years of followup were scored according to the Sharp-van der Heijde Scoring (SHS) method. Pyridinoline serum levels at baseline and during followup were measured by ELISA. The association between baseline pyridinoline levels and difference in SHS over 7 years was tested, with a multivariate normal regression model. Second, the association between pyridinoline levels determined during the disease course and progression of SHS over the next year was tested with a multivariable linear regression analysis.
Results. Studying baseline pyridinoline serum levels in 437 patients revealed that the mean SHS over 7 years was 6% higher for every higher pyridinoline level (nmol/l) at baseline (p = 0.001). Subsequently, during followup (n = 184 patients) the progression in SHS in the upcoming year was 17% higher for every higher nmol/l pyridinoline level (p = 0.001). The area under the receiver-operation characteristic curve for rapid radiological progression was 0.59.
Conclusion. Increased pyridinoline serum levels, both at baseline and during the disease course, are associated with more severe joint destruction during the coming year(s), although the predictive accuracy as a sole predictor was moderate.
Predicting an individual patient’s future disease severity is required for decisions for individualized treatment. At disease onset it can guide the initial treatment strategy and during the disease course it may guide treatment adaptations. The severity of rheumatoid arthritis (RA) is often measured using the extent of joint destruction. At present, only part of the variance in joint destruction is explained by currently known risk factors, which consist mainly of autoantibodies and markers of inflammation1. Markers of cartilage or bone metabolism have been studied to a lesser extent. Studies have found evidence that C-terminal crosslinking telopeptide of type I collagen (CTX-I) and C-terminal crosslinking telopeptide of type II collagen (CTX-II)2 were associated with radiologic progression. Pyridinoline is a major crosslink of collagen in cartilage and is also present in collagen of bone and other tissue as synovium. Based on initial studies it can be presumed that pyridinoline might be a good marker for RA as well. Pyridinoline levels are increased in patients with RA compared to healthy persons or to patients with other rheumatologic diagnoses3,4,5,6. In addition, some studies indicate that pyridinoline levels are higher in cases of active or severe RA3,4,7,8,9. Most previous studies were performed on urine levels of pyridinoline.
To date no large longitudinal studies on serum pyridinoline levels and severity of joint destruction in RA have been performed. We evaluated the predictive value of serum pyridinoline levels for future joint destruction, both at baseline for longterm prediction and during the course of RA for more near-term prediction of disease severity.
MATERIALS AND METHODS
Patients
Patients included in the Leiden Early Arthritis Clinic (EAC) cohort that fulfilled the 1987 American College of Rheumatology criteria for RA at baseline or during the first year of disease were studied. The Leiden EAC is a large, prospective cohort1. Briefly, patients were referred by general practitioners when arthritis was suspected and were included in the EAC cohort if arthritis was confirmed on physical examination and symptom duration was < 2 years. At inclusion, patients were queried about their joint symptoms and underwent examination. At baseline and at the yearly followup visits, blood samples were taken for routine diagnostic laboratory screening and serum was stored at −70°C. Radiographs of hands and feet, taken at baseline and yearly thereafter during 7 years of followup, were scored according to the Sharp-van der Heijde Scoring (SHS) method with known time order by an experienced reader, blinded to any clinical information. The within-reader ICC was 0.91. Written informed consent was obtained from all participants. The study was approved by the local medical ethics committee.
Pyridinoline levels
Pyridinoline serum levels were measured by ELISA (QuickVue; Quidel Corp.), according to the manufacturer’s instructions, using stored baseline and followup serum samples. All baseline and all followup ELISA were done at the same point in time. The intraassay coefficient of variation (CV) was 6.8% and the interassay CV was 11.1%. The limit of detection was 0.5 nmol/l (lower limit of quantification 0.5 nmol/l and upper limit of quantification 12 nmol/l).
Statistical analyses
To approximate a normal distribution, all radiological data were log-transformed before analyses. First, associations between baseline pyridinoline levels and log-transformed radiographic joint destruction over 7 years were analyzed using a multivariate normal regression model with radiological score as response variable, testing for a constant difference in SHS. This method analyzes all repeated measurements at once and takes advantage of the correlation between these measurements. The effect of time was entered as a factor in the model, to properly capture the mean response profile over time10. All analyses were adjusted for age, sex, and treatment strategy. The treatment strategies differed according to the inclusion period, which was used as a proxy for treatment strategy in the analyses. Patients included in 1993–95 were initially treated with nonsteroidal antiinflammatory drugs, patients included in 1996–98 were initially treated with chloroquine or salazopyrine, and patients included after 1999 were promptly treated with methotrexate or salazopyrine. Since the baseline SHS is included in the repeated measurement analyses as the response variable, baseline SHS was not also included as an adjustment factor. Next, additional adjustments were made including other known risk factors for progression of joint destruction: anticyclic citrullinated peptide (CCP) antibody status, C-reactive protein (CRP) levels, body mass index (BMI), and smoking. The analyses were repeated for the total erosion score and the total joint space narrowing score as outcomes, adjusted for age, sex, and treatment.
The association between pyridinoline levels determined during the disease course and progression of joint damage during the next year was studied with a multivariable linear regression analysis with log-transformed delta SHS over the upcoming year as response variable, adjusting for age, sex, treatment, and disease duration. Thereafter, additional adjustments were made for CCP-positivity and CRP level. The first analysis with pyridinoline levels during disease course were also repeated with total joint space narrowing score and erosion score as outcomes.
To evaluate the prognostic accuracy for clinical practice, the positive and negative likelihood ratios (LR) and area under the receiver-operator characteristic (ROC) curve (AUC) were determined. Therefore pyridinoline levels and radiographic progression were recoded as binary variables. Radiologic data were categorized using a definition of rapid radiographic progression (increase of SHS ≥ 5 after 1 year) as reported11. This was done at baseline and during the disease course. The cutoff point to categorize pyridinoline levels was determined based on the optimal maximum from the ROC curve, with rapid radiological progression (RRP) as outcome. Finally, the prognostic accuracy was determined for pyridinoline levels on RRP and any progression in joint destruction during the next year (an increase of ≥ 1 SHS in 1 year). Correlations between CRP and pyridinoline levels were determined with Spearman’s correlation coefficients. Analyses were performed using SPSS version 20.0. P values < 0.05 were considered significant.
RESULTS
Baseline serum pyridinoline levels
Serum pyridinoline levels were determined in 437 patients with early RA, who had median symptom duration of 19 weeks. Patient characteristics are provided in Table 1. The median serum level was 4.7 nmol/l (range 3.8–6.0). These baseline levels were significantly associated with the severity of joint damage over 7 years. For every nmol/l increase in pyridinoline level at baseline, patients had 6% higher total SHS (β = 1.06, p = 0.001; Figure 1A). After adjustment for age, sex, and treatment and also for known risk factors such as anti-CCP positivity, CRP levels, BMI, and smoking, the association between serum pyridinoline level and joint destruction remained significant (β = 1.06, p = 0.044).
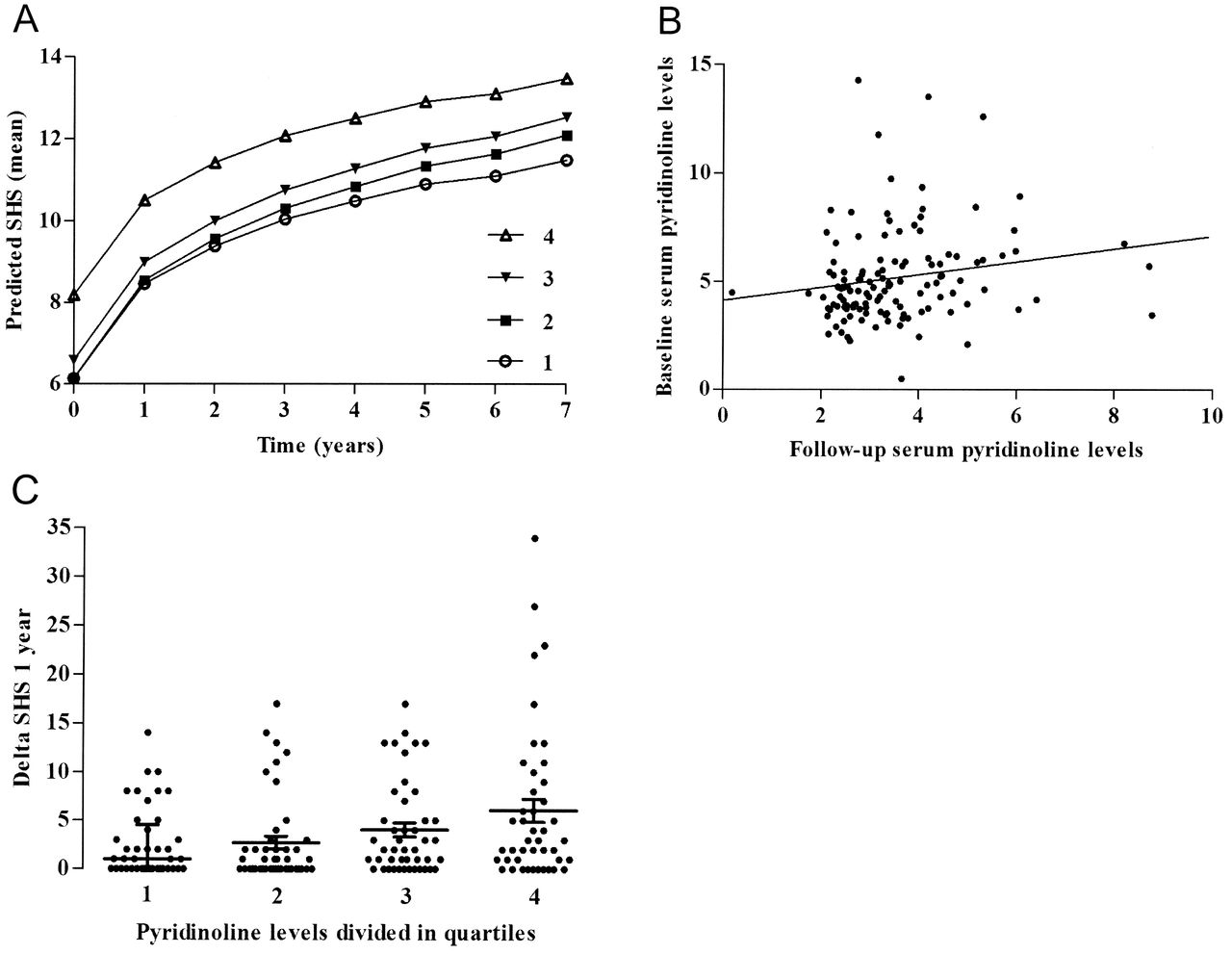
(A) Association between baseline serum pyridinoline levels and the severity of joint destruction over 7 years. Predicted SHS from a multivariable normal regression model is shown, with continuous pyridinoline levels, age, sex, and treatment on the y-axis and time on the x-axis. Serum pyridinoline levels were analyzed at a continuous level, but are divided into quartiles here. First quartile represents lowest 25% of pyridinoline levels, second quartile the highest 25% of the lowest 50%, third quartile the lowest 25% of the highest 50%, and the fourth quartile the highest quartile of pyridinoline levels. (B) Correlation between baseline serum levels and followup serum levels. (C) Association of followup serum pyridinoline levels with progression of joint damage during the next year. Pyridinoline levels were analyzed as a continuous variable but are divided in quartiles here. First quartile represents the lowest 25% of pyridinoline levels, second quartile the highest 25% of the lowest 50%, third quartile the lowest 25% of the highest 50%, and the fourth quartile represents the highest quartile of pyridinoline levels. Horizontal lines indicate the median, with 2-sided interquartile range bars. SHS: Sharp-van der Heijde Score.
Characteristics of 437 patients with early rheumatoid arthritis (RA). Baseline patient characteristics are presented, or at time of serum sampling for followup samples.
The total SHS is a composite of the total erosion score and joint space narrowing score. In order to determine whether serum pyridinoline was associated with bone or cartilage destruction in particular, analyses were repeated on these 2 subscores. Significant associations were observed between serum pyridinoline levels at baseline and both the severity of erosions and joint space narrowing over time (β = 1.06, p = 0.025, and β = 1.05, p = 0.002, respectively).
Serum pyridinoline levels during the disease course
Followup serum samples of 184 patients with RA were studied; the mean disease duration at serum sampling was 4 years (± 2 yrs). The median serum level was 3.3 nmol/l (range 2.6–4.2). Pyridinoline levels measured at baseline and during the disease course were correlated (rs = 0.251, p = 0.005; Figure 1B). Subsequently, the association between serum pyridinoline levels and near-term increase in SHS score over the next year was evaluated. After adjustment for age, sex, treatment, and disease duration it was observed that for every nmol/l increase in pyridinoline level, the progression in SHS over the upcoming year was 17% higher (β = 1.17, p = 0.001; Figure 1C). Also including adjustments for anti-CCP positivity and CRP level, the association between pyridinoline level and progression in SHS over the upcoming year remained significant (β = 1.15, p = 0.003).
Subanalyses on the erosion or joint space narrowing scores as outcomes also here yielded significant results for the severity of bone and cartilage destruction (β = 1.10, p = 0.014, and β = 1.10, p = 0.025, respectively).
Prognostic accuracy
The optimal maximum of baseline serum pyridinoline levels on the ROC curve with RRP as outcome was 4.7480 nmol/l. Patients with a baseline pyridinoline level ≥ 4.8 nmol/l had a positive LR of 1.30 for RRP (increase in SHS ≥ 5) during the first year. The negative LR was 0.77 and AUC was 0.59. When taking any progression in joint destruction in the first year as outcome, positive LR was 1.25, negative LR was 0.83, and AUC was 0.56.
The optimal maximum of followup serum pyridinoline levels on the ROC curve with RRP as outcome was 3.3983 nmol/l. Patients with RA who during the disease course had a pyridinoline level ≥ 3.4 nmol/l had a positive LR of 1.49 for RRP (SHS increase ≥ 5) during the next year. The negative LR was 0.67 and AUC was 0.61. Taking SHS ≥ 1 during the next year as the outcome, the positive LR was 2.00, negative LR was 0.61, and AUC was 0.64.
DISCUSSION
We investigated the predictive value of serum pyridinoline levels for future joint destruction and observed that increased pyridinoline levels were significantly associated with more severe joint destruction. This applied to baseline serum levels and joint damage over 7 years as well as to serum levels determined during the disease course and joint destruction during the upcoming year.
The association between pyridinoline and severity of joint damage was observed to be independent of the association of other factors (such as anti-CCP or CRP) with progression of joint damage. Although in the multivariable analyses serum pyridinoline was found to be an independent risk factor, the positive LR and AUC were moderate. This indicates that the serum pyridinoline level alone is insufficient for adequate prediction, but that it will be valuable to include serum pyridinoline in combined predictive models.
Intriguingly, serum levels taken at baseline and during the disease course were correlated. Further, both serum levels were associated with more severe joint destruction over time. Together these data may suggest that patients with more severe radiological progression have increased serum pyridinoline levels at the start of and throughout the disease course. Because treatment effect may have influenced the outcome measures, all analyses were adjusted for differences in treatment.
The strengths of our study are the large group of patients with RA and the availability of high-quality longterm followup data. A limitation could be the lack of measured deoxypyridinoline. Deoxypyridinoline exists only in bone, and pyridinoline in both cartilage and bone. Hence the ratio of these markers can be used to determine whether serum pyridinoline was derived from breakdown of cartilage or bone. To make this distinction we performed subanalyses on pyridinoline levels in relation to joint space narrowing and erosions. These showed that associations were present for both cartilage loss and bone damage.
Another limitation is that our analyses were based on patients from a single cohort. Additional large-scale longitudinal studies on the prognostic value of serum pyridinoline levels are needed to replicate our findings and to establish the predictive value of this biomarker.
Increased serum pyridinoline levels are of additive value to known serological risk factors for future joint damage in patients with RA, both at baseline and during the disease course. A combination of multiple biomarkers with other risk factors most likely will be required to make adequate predictions.
Footnotes
-
A. Krabben was supported by a grant from the Dutch Arthritis Foundation. A.H.M. van der Helm-van Mil was supported by a grant from the Dutch Organization of Health Research and Development. Research was supported by The European Community Seventh Framework Program FP7 Health-F2-2008-223404 (Masterswitch) and by a core grant from the Dutch Arthritis Foundation.
- Accepted for publication March 28, 2013.








{kind=link}