

Abstract
Objective. Biologic treatments including the humanized anti-interleukin 6 (anti-IL-6) receptor antibody tocilizumab (TCZ) provide therapeutic options for patients with rheumatoid arthritis (RA). We investigated useful biomarkers to predict the responsiveness to TCZ by measurement of serum proinflammatory cytokine concentrations.
Methods. Serum samples were collected from 61 patients with RA before biologic treatment and at 4 weeks after initial administration of either TCZ (n = 32) or infliximab (IFX; n = 29) and from 13 healthy serum donor controls. Disease Activity Score of 28 joints (DAS28) was determined at baseline and after treatment.
Results. Although IL-1β, IL-2, IL-6, IL-17A, IL-17F, interferon-α, and tumor necrosis factor-α (TNF-α) were all increased in sera from patients with RA compared with controls, only the IL-6 level was significantly correlated with DAS28 before treatment. The IL-6 level before treatment was positively correlated with DAS28 after TCZ treatment, and was significantly lower in TCZ-responsive patients (as judged by a post-treatment DAS28 < 3.2) than in TCZ-resistant patients (post-treatment DAS28 ≥ 3.2). DAS28 after TCZ was significantly lower than after administration of IFX in patients with low pretreatment IL-6 (< 51.5 pg/ml, the mean baseline value of IL-6 in all RA patients), but not in those with high pretreatment IL-6. These results indicate that low serum IL-6 is associated with a favorable response to TCZ.
Conclusion. Although both TNF-α and IL-6 are major targets of therapeutic intervention in RA, baseline serum IL-6 but not baseline TNF-α level is a potential biomarker reflecting disease activity. Measurement of serum IL-6 in RA before treatment may be useful to estimate residual disease activity after TCZ treatment and to predict responsiveness to TCZ treatment.
- RHEUMATOID ARTHRITIS
- TOCILIZUMAB
- INFLIXIMAB
- TUMOR NECROSIS FACTOR-α
- INTERLEUKIN 6
- INFLAMMATORY CYTOKINES
- DISEASE ACTIVITY SCORE 28
Rheumatoid arthritis (RA) is a chronic autoimmune disorder characterized by inflammation of synovial membranes and destruction of cartilage and bone. Biologic treatments, including several types of tumor necrosis factor-α (TNF-α) inhibitor, interleukin 6 (IL-6) receptor inhibitor, and a synthetic analog of cytotoxic T lymphocyte antigen-4 (CTLA4), have provided therapeutic options for patients with RA. However, responsiveness to biologics is variable among individuals, and there are poor responders to certain biologic treatments. Therefore, it is essential to identify useful biomarkers that predict responsiveness to biologics. Recent reports have indicated that plasma type I interferon (IFN) activity, serum levels of IL-1 receptor antagonist, and IL-1β levels in lipopolysaccharide-stimulated blood culture are useful factors that predict the response to anti-TNF-α therapies1,2. However, there is scant evidence for predictive factors in anti-IL-6 therapy.
The clinical influence of anti-TNF-α and anti-IL-6 therapies on progression of RA helps us comprehend the critical role of these cytokines and engenders a novel concept of TNF-α- and IL-6-dependent immunity. Both cytokines, which can be secreted from a wide variety of cells including macrophages, T cells, B cells, and synovial fibroblasts, are regarded as upper-rank cytokines in the hierarchical cytokine network involved in the pathogenesis of RA3. For example, differentiation of Th17 cells, which has been implicated in the inflammatory response of RA4, is regulated by both IL-6 and TNF-α5. Studies have revealed that anti-TNF-α therapy reduces serum levels of proinflammatory cytokines including IL-1β, IL-6, and TNF-α6,7 as well as the inflammatory chemokines IL-8, monocyte chemoattractant protein-1, macrophage inflammatory protein-3α, RANTES (regulated on activation, normal T cell expressed and secreted), and IFN-γ-inducible protein-108,9,10. Although there is abundant evidence for the immunomodulatory action of anti-TNF-α therapy from a series of clinical studies measuring serum cytokine concentrations, there is little evidence concerning the immunomodulatory effects of the anti-IL-6 therapy tocilizumab (TCZ), which acts as an IL-6 receptor (IL-6R) antagonist and a competitive inhibitor of IL-6 signaling. However, the profoundly efficacious outcomes of TCZ treatment suggest a pivotal role for the IL-6–dependent immune response in influencing the cytokine network in RA. Indeed, IL-6 has a broad range of biological activities against a variety of immune cells and regulates immune responses such as B cell proliferation and antibody production, hematopoiesis, and T cell differentiation. Further, IL-6 directly triggers the release of acute-phase proteins such as C-reactive protein (CRP) from liver tissues11, promotes differentiation of Th17 cells12, and activates synovial fibroblasts to express matrix metalloproteinases (MMP)13 and receptor activator of nuclear factor-κB (RANK) ligand14 that in turn induce the differentiation of osteoclasts with bone-resorbing activity15, leading to bone erosions. However, it remains largely unclear how in vivo IL-6 hierarchically intervenes in the cell–cytokine network linked to the pathogenic events of RA, or how an IL-6-blocking agent influences serum proinflammatory cytokine concentrations.
The aim of our study was to identify useful biomarkers for RA in order to select TCZ treatment for patients who will have a better therapeutic response to this agent; thus, we undertook measurement of serum proinflammatory cytokine concentrations as a systemic response in patients with RA undergoing TCZ treatment, and assessed the in vivo immunomodulatory action of TCZ on the cytokine network. Our results showed that serum IL-6 is a critical biomarker for evaluating disease activity and that measurement of IL-6 before and after TCZ treatment is a useful means to predict the response to this biologic agent. Our data provide new insight into the in vivo active mechanisms underlying the blockade of IL-6 activity in RA.
MATERIALS AND METHODS
Patients, clinical assessment, and therapy
Peripheral blood samples were collected from 13 healthy serum donor controls and 61 biologic-naive patients with RA diagnosed according to the revised American College of Rheumatology criteria16 at the First Department of Internal Medicine and the Department of Rheumatology and Clinical Immunology, Kansai Medical University, Osaka, Japan. Written informed consent was obtained from all patients with RA. This study was approved by the Institutional Review Board of Kansai Medical University and the research was in compliance with The Declaration of Helsinki. The 13 controls, who had no evidence of infection (no physical symptoms, increased CRP, or abnormal leukocyte count), were selected from among hospital workers.
Data were collected at baseline (before treatment) and after treatment (at 4 weeks after initial administration) with either TCZ (32 patients) or infliximab (IFX; 29 patients) as a first biologics therapy. TCZ was infused at 8 mg/kg every 4 weeks, and IFX was infused at 3 mg/kg at 0, 2, and 6 weeks and then every 8 weeks. At infusion and each followup visit, the following clinical data were recorded: physician’s global assessment of disease activity, patient’s global assessment of disease activity, patient’s assessment of pain, patient’s assessment of fatigue, CRP, erythrocyte sedimentation rate (ESR), rheumatoid factor (RF), and MMP3. The patients’ 28-joint Disease Activity Score (DAS28)/CRP4 and DAS28/ESR4 were calculated after data collection. The mean age of patients and baseline data are shown in Table 1. No significant differences were noted at study entry between groups treated with TCZ and IFX. All patients had been taking a stable dose of MTX 2.5 to 10.0 mg/week.
Characteristics of patients with rheumatoid arthritis (RA) prior to treatment with tocilizumab (TCZ) or infliximab (IFX). Values are mean ± SD. Statistical significance of differences in measurements between patients treated with TCZ and those treated with IFX was determined using the Wilcoxon signed-rank test.
Analysis
After centrifugation of blood samples, sera were stored at −80°C until analysis. IL-1β, IL-2, TNF-α, IFN-α, and IL-6 were quantified by a cytometric bead array method (BD Biosciences) and IL-17A (R&D Systems) and IL-17F (Abcam) were measured with quantitative ELISA kits. Minimal detectable concentration of each cytokine as stated in the manufacturers’ instructions was 2.3 pg/ml (IL-1β), 11.2 pg/ml (IL-2), 1.6 pg/ml (IL-6), 15.6 pg/ml (IL-17A), 20 pg/ml (IL-17F), 0.7 pg/ml (TNF-α), and 1.5 pg/ml (IFN-α).
Statistical analysis
The data from 2 independent groups (patients with RA and controls) were compared using Mann-Whitney U tests. Associations between clinical/laboratory measures and serum cytokine levels were assessed using Pearson’s correlation test or Spearman’s rank correlation test. The statistical significance of differences between pre- and post-treatment measurements was analyzed using Wilcoxon signed-rank tests. A value of p < 0.05 was considered statistically significant.
RESULTS
High levels of serum cytokines in patients with RA
We first analyzed serum IL-1β, IL-2, IL-6, IL-17A, IL-17F, IFN-α, and TNF-α concentrations in 61 patients with RA at baseline prior to the first administration of biologics (32 patients with TCZ, 29 patients with IFX) and 13 healthy controls. Patient characteristics are given in Table 1. All patients had been taking a stable dose of MTX orally before biologics therapy. In controls, serum cytokine concentrations were undetectable except for IL-17F (mean 298.3 ± 677.6 pg/ml); in patients with RA, serum concentrations of all proinflammatory cytokines that we tested were detectable at higher levels: IL-1β, 11.38 ± 17.08 pg/ml; IL-2, 31.33 ± 68.91 pg/ml; IL-6, 51.52 ± 85.50 pg/ml; IL-17A, 18.48 ± 73.52 pg/ml; IL-17F, 9,886 ± 17,664 pg/ml; IFN-α, 12.16 ± 16.96 pg/ml, and TNF-α, 23.37 ± 45.74 pg/ml (Figure 1). Among these cytokines, we found a strong positive correlation between TNF-α and IL-1β levels (r = 0.659), and weaker positive correlations between the levels of other pairs of proinflammatory cytokines, such as IL-1β and IL-2 (r = 0.431), IFN-α and IL-17A (r = 0.435), and IFN-α and IL-17F (r = 0.415; Table 2). However, the serum level of IL-6 did not show a significant correlation with any other cytokines. Despite this, our analyses of DAS28/CRP4 and DAS28/ESR4 as indices of RA disease activity showed that, among these cytokines, only IL-6 was significantly correlated with either DAS28/CRP4 or DAS28/ESR4 (Table 3). These findings suggest that the serum IL-6 level is a good biomarker reflecting disease activity in RA, but that this is not the case with TNF-α, although both cytokines are major targets of therapeutic intervention in RA.
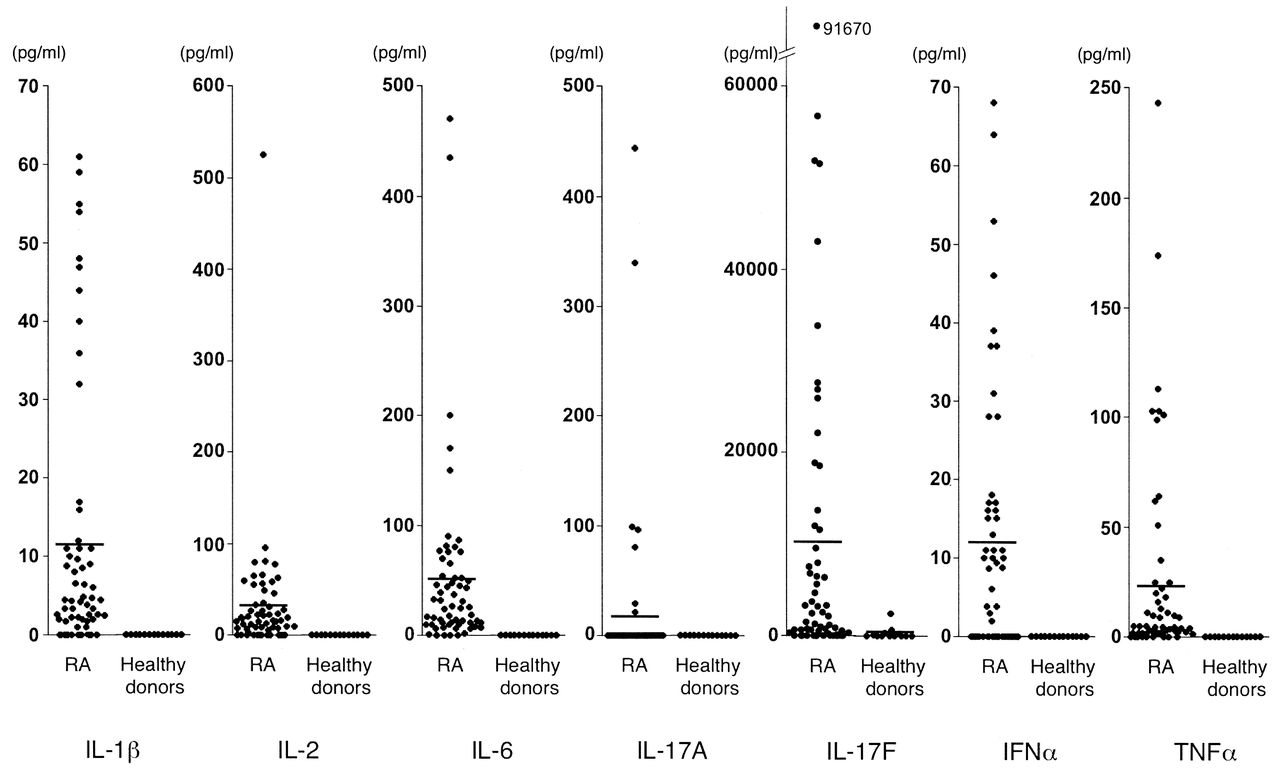
Increased proinflammatory cytokine concentrations in serum samples from 61 patients with rheumatoid arthritis (RA) and 13 controls. Baseline serum concentrations in RA patients prior to the first administration of biologics were detectable at high levels: interleukin 1β (IL-1β), 11.38 ± 17.08 pg/ml; IL-2, 31.33 ± 68.91 pg/ml; IL-6, 51.52 ± 85.50 pg/ml; IL-17A, 18.48 ± 73.52 pg/ml; IL-17F, 9886 ± 17,664 pg/ml; interferon α (IFN-α), 12.16 ± 16.96 pg/ml; tumor necrosis factor-α (TNF-α), 23.37 ± 45.74 pg/ml. Serum cytokine concentrations from controls were undetectable, except for IL-17F (298.3 ± 677.6 pg/ml). Each dot represents an individual donor; bars indicate mean values.
Correlations between serum cytokine levels in RA were evaluated at baseline. Statistical significance of the correlation coefficient (r) was determined using Spearman’s rank correlation test (r > 0.3 or p < 0.05; data shown in bold type).
Correlation between disease activity indices and serum proinflammatory cytokine levels. Clinical variables (DAS28/ESR4 and DAS28/CRP4) and serum cytokine levels were evaluated at baseline. Statistical significance of the correlation coefficient (r) was determined using Spearman’s rank correlation test (r > 0.3 or p < 0.05; data shown in bold type).
Immunomodulatory effects of TCZ and IFX on proinflammatory cytokines and disease activity indices
We next investigated the modulatory effects of RA treatment with TCZ or IFX on clinical and laboratory measures of inflammatory RA activity and serum cytokine concentrations by comparing data before and after TCZ or IFX treatment. Our study confirmed the widely known finding that there is notable clinical improvement in RA, as judged by a significant reduction in levels of CRP, ESR, DAS28/CRP4, and DAS28/ESR4, at 4 weeks after the initial administration of either TCZ or IFX compared with baseline (Table 4). Among cytokines we tested, serum IL-2 levels were significantly decreased by both TCZ and IFX treatment (Table 5). While TCZ treatment significantly decreased serum TNF-α levels, there was also a tendency (p = 0.062) for TNF-α to be decreased by IFX treatment. Notably, although IFX treatment significantly decreased serum IL-6 levels, TCZ treatment significantly increased IL-6 levels regardless of the improvements in clinical measures 4 weeks after administration (Table 5). In contrast to IFX, which significantly decreased serum levels of IL-17F, TCZ did not affect IL-17F levels.
Clinical improvement after TCZ or IFX therapy as judged by clinical and laboratory measures evaluated at baseline and at 4 weeks after administration of biologics. Significant reduction was observed in levels of CRP, ESR, DAS28/CRP4, and DAS28/ESR4 after treatment, compared with baseline. Statistical significance of differences in measurements between baseline and post-treatment was determined using the Wilcoxon signed-rank test. Values are mean ± SD.
Immunomodulatory effects of TCZ or IFX therapy on serum cytokine concentrations, which were evaluated at baseline and at 4 weeks after biologics. Statistical significance of the differences in measurements between baseline and post-treatment was determined using the Wilcoxon signed-rank test (p < 0.05; data shown in bold type). Values are mean ± SD pg/ml.
Increased serum concentration of IL-6 after TCZ correlates with disease activity at baseline
A previous report indicated the possibility that the increased serum IL-6 level measured after initial administration of TCZ reflects the potential disease activity of RA17. Our current study also showed a significant correlation between the increased serum level of IL-6 at 4 weeks after TCZ administration and each of the clinical/laboratory measures of disease activity (DAS28/CRP4 and DAS28/ESR4) at baseline (Table 6), providing support for the hypothesis presented by Nishimoto, et al17. The other cytokines tested after TCZ treatment, IL-1β, IL-2, IL-17A, IL-17F, IFN-α, and TNF-α, showed no significant correlation with disease activity indices at baseline. Therefore the measurement of serum IL-6 after TCZ treatment may provide a useful confirmation of the potential disease activity of RA.
Correlation between disease activity at baseline and serum cytokine levels after TCZ therapy. Correlations between DAS28 scores at baseline and serum cytokine levels at 4 weeks after TCZ administration were analyzed. Statistical significance of the correlation coefficient (r) was determined using Spearman’s rank correlation test (r > 0.3 or p < 0.05; data shown in bold type).
Utility value of serum IL-6 before treatment as a biomarker to estimate responsiveness to TCZ
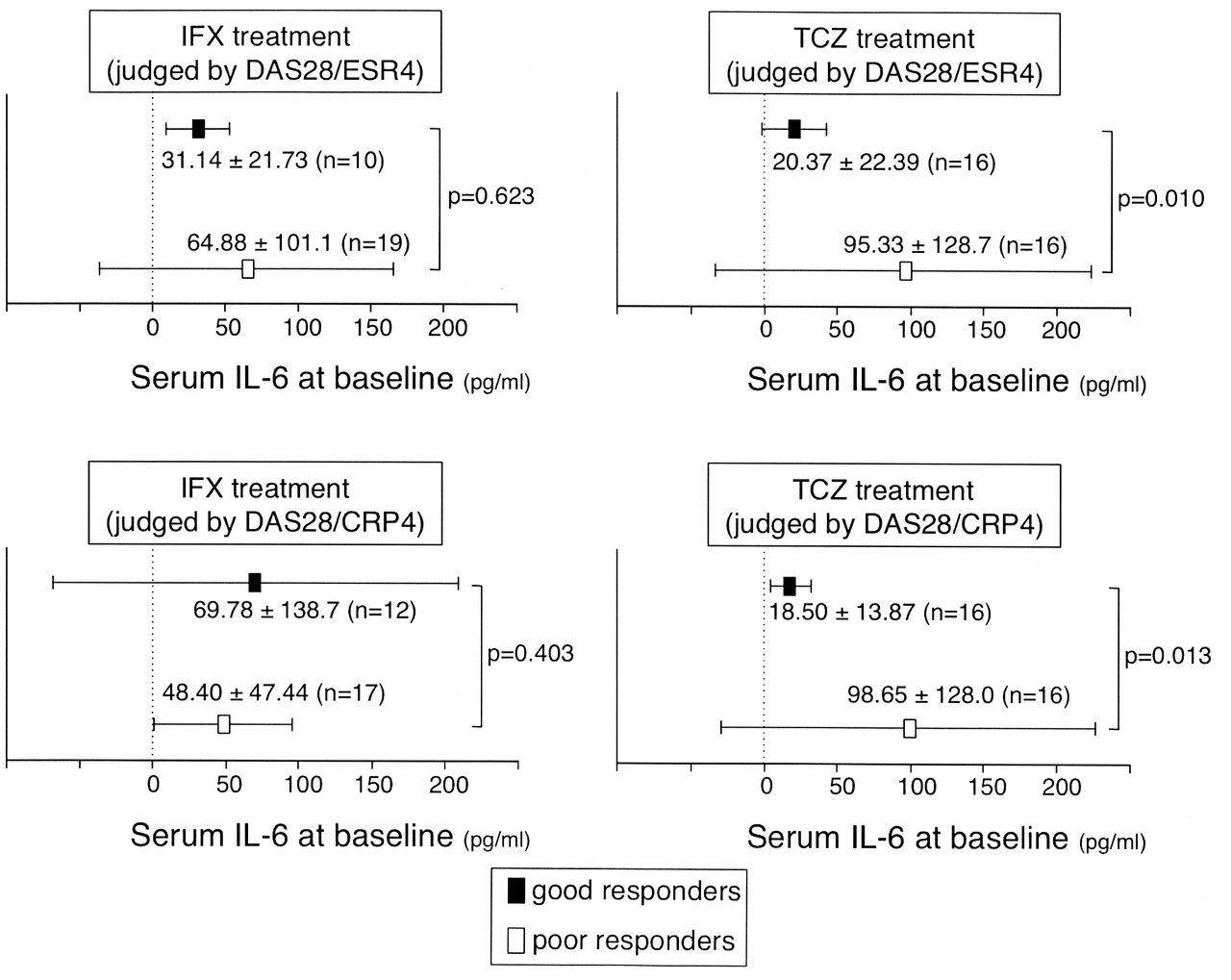
To identify a biomarker that would predict resistance to biologic treatment at baseline, we next analyzed cytokines at baseline for correlation with post-treatment DAS28 measures as indices of residual RA disease activity. Our results showed that only serum IL-6 level at baseline was positively correlated with either DAS28/CRP4 or DAS28/ESR4 after the initial administration of TCZ (Table 7), suggesting that a high serum concentration of IL-6 at baseline is a putative biomarker for TCZ resistance. Other cytokine concentrations at baseline showed no significant correlation with the DAS28 indices after TCZ or IFX treatment. To confirm this point, we sorted all patients into 2 groups: good responders, with DAS28/ESR4 < 3.2 or DAS28/CRP4 < 2.7 at 4 weeks after initial administration of the biologic; and poor responders, with DAS28/ESR4 ≥ 3.2 or DAS28/CRP4 ≥ 2.7 at this timepoint. We then compared mean serum levels of IL-6 at baseline in each group, between good responders and poor responders to TCZ, and between good responders and poor responders to IFX. The mean pretreatment IL-6 level in the good responders to TCZ (whether judged by DAS28/ESR4 or DAS28/CRP4), was significantly lower than that in the poor responders to TCZ (Figure 2). However, there was no significant difference in mean pretreatment serum IL-6 levels between the groups of good responders and poor responders to IFX treatment (Figure 2). These results suggest that effective TCZ treatment can be predicted by a low serum concentration of IL-6 before treatment.
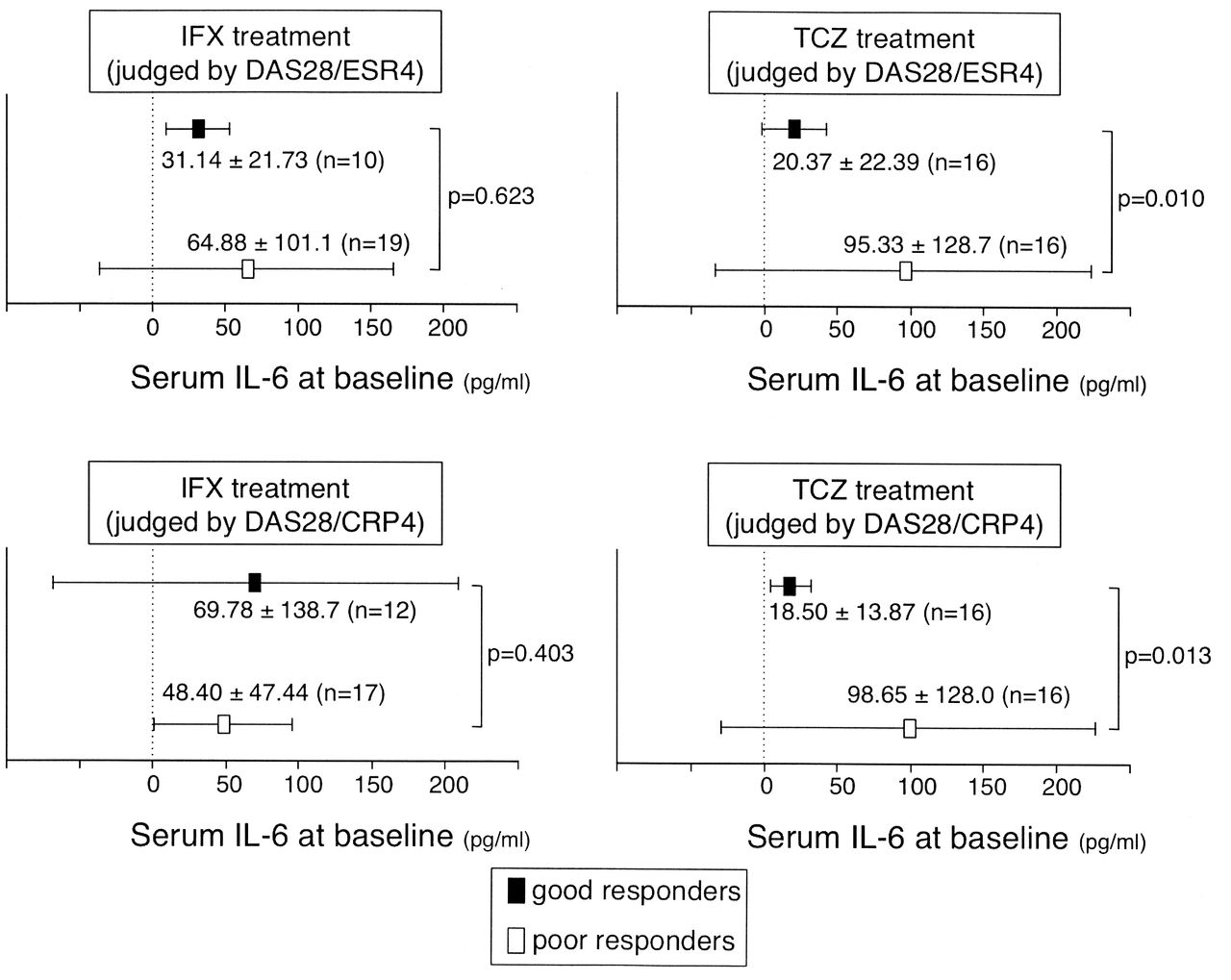
Significant differences in serum interleukin 6 (IL-6) levels at baseline between good responders and poor responders, as judged by DAS28 indices at 4 weeks after treatment with TCZ or IFX. The mean IL-6 level at baseline in the good responders to TCZ was significantly lower than that in the poor responders to TCZ. There was no significant difference in mean IL-6 levels between good responders and poor responders to IFX treatment. Statistical significance of differences in serum IL-6 levels at baseline between the 2 groups was determined by Wilcoxon signed-rank test. Values are mean ± SD. Good responders: DAS28/ESR4 < 3.2 or DAS28/CRP4 < 2.7. Poor responders: DAS28/ESR4 ≥ 3.2 or DAS28/CRP4 ≥ 2.7. DAS28: 28-joint Disease Activity Score; TCZ: tocilizumab; IFX: infliximab; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein.
Correlation between serum cytokine levels at baseline and residual DAS28 scores at 4 weeks after TCZ or IFX administration. Statistical significance of the correlation coefficient (r) was determined using Spearman’s rank correlation test (r > 0.3 or p < 0.05; data shown in bold type).
To further focus on the usefulness of the serum IL-6 level at baseline as a predictive biomarker to estimate the response to TCZ treatment, we sorted all patients into 2 groups, high IL-6 and low IL-6, according to whether the serum IL-6 level at baseline was, respectively, above or below 51.5 pg/ml, the mean baseline value for all patients. We then analyzed the statistical significance of differences in the DAS28 indices after treatment between the 2 groups. As shown in Table 8, in the low IL-6 group, both the DAS28 indices (DAS28/ESR4 and DAS28/CRP4) after TCZ treatment were significantly lower than those after IFX treatment. Meanwhile, there were no significant differences in post-treatment DAS28 indices between TCZ and IFX treatments in the high IL-6 group. This result suggests that, in RA patients with a low serum IL-6 concentration before treatment, TCZ has a more potent effect than IFX. This might not be the case in patients with a high serum concentration of IL-6. On the basis of our results, we propose that the serum IL-6 level before biologic treatment is a predictive biomarker for the effectiveness of TCZ treatment in RA, and that low serum IL-6 concentration could be a useful indicator for preferential selection of TCZ as a biologic treatment.
DAS28 scores were significantly lower after TCZ treatment than after IFX treatment in “low IL-6” groups. Patients were sorted into “high IL-6” and “low IL-6” groups, according to level of serum IL-6 at baseline, as below. Statistical significance of differences in post-treatment DAS28 indices between TCZ and IFX treatments in each group was determined by Wilcoxon signed-rank test. Values for p < 0.05 indicated by bold type. High IL-6 group: serum IL-6 at baseline > 51.5 pg/ml (mean value of IL-6 for all patients). Low IL-6 group: serum IL-6 at baseline ≤ 51.5 pg/ml.
DISCUSSION
Of the proinflammatory cytokines, TNF-α and IL-6 are regarded as the upper tier in a hierarchical cytokine network that regulates a wide variety of inflammatory processes in the pathogenesis of autoimmune diseases such as RA. Although both TNF-α and IL-6 are the principal targets of therapeutic intervention in RA, our results indicate that serum IL-6 level at baseline is a better predictive biomarker for estimating disease activity than TNF-α. We also demonstrated that increased concentration of IL-6 after TCZ treatment reflects potential disease activity in RA. In addition, our study shows that measurement of serum IL-6 before treatment is useful in predicting the effectiveness of TCZ, and that low baseline IL-6 is a valuable indicator for the preferential choice of TCZ as biologic treatment. We have therefore identified the clinical importance of IL-6 as a biomarker, especially in the response to TCZ therapy.
Given the biological function of TCZ as a competitive inhibitor of the IL-6R, increased serum IL-6 after TCZ administration might be caused by inhibition of IL-6R-mediated clearance, and this free IL-6 cannot induce intracellular signals because IL-6R are occupied by TCZ. In another study, consistent with our results showing that increased IL-6 after administration of TCZ correlates with clinical measures of disease activity (CRP, ESR, DAS28/CRP4, or DAS28/ESR4) at baseline, Nishimoto, et al reported that TCZ treatment increases serum IL-6 concentrations in RA and Castleman disease, and they concluded that the increased level of free IL-6 in sera reflects the endogenous potential for IL-6 production and the true disease activity in the patient17.
Previous studies have not reached a common consensus as to the serum TNF-α and IL-6 concentrations that are predictive biomarkers in progression of RA. It has been reported that, in contrast to our results, serum levels of TNF-α are similar in patients with RA and normal controls18,19; and that, in support of our results, serum levels of IL-6 in RA at baseline correlated with some disease activity indices20. In addition, a recent study has also shown that serum IL-6 level is associated not only with DAS28 but also with radiographic structural progression and increased levels of autoantibody secretion in patients with RA21. Thus, IL-6 may be a possible biomarker of RA activity. In this context, a low baseline serum IL-6 level could indicate low potential disease activity and therefore correlate with better treatment outcome with TCZ therapy. Moreover, increased concentration of serum IL-6 leads to internalization and degradation of the IL-6R in T cells and synovial tissues22. Therefore, it might be inferred that TCZ could not work efficiently as a competitive inhibitor of the IL-6R when blocking this downregulated IL-6R in patients with high serum IL-6 concentration.
Serum concentrations of TNF-α and IL-6 were relatively low or marginal for determination by cytometric bead array or ELISA methods. Therefore, it is possible that the low sensitivity of this detection method to these cytokine levels in sera could be responsible for the conflicting outcomes. In this context, serum levels of IL-17F showed much higher titers than levels of TNF-α and IL-6 as well as IL-17A. Considering the evidence showing a pathogenic role for Th17 cells infiltrating synovial membranes and the importance of Th17 cells in development of RA4,23, we hypothesized that IL-17F could potentially be useful as a biomarker to evaluate disease activity. However, contrary to our expectations, our study revealed no significant correlation between serum IL-17F levels and disease activity indices in RA. We also found that IL-17F concentration was decreased by IFX (a TNF-α inhibitor), but not by TCZ administration, suggesting a link between endogenous Th17 cell activity and TNF-α-mediated inflammation in RA. This finding is supported by a previous report showing that IFX reduces the frequency of Th17 cells in patients with RA24. Because IL-6 plays a key role in inducing the differentiation of Th17 cells, the reduction of IL-17F in our study might be attributed to the concomitant reduction of IL-6 by treatment with IFX. Meanwhile, during TCZ treatment, which results in an increase in serum IL-6 concentration without affecting IL-17F concentration, soluble IL-6 could not induce intracellular signals because of blockade of the IL-6R. Therefore, measurement of IL-17F, in contrast to IL-6, after TCZ treatment is useless for evaluating or estimating the real disease activity in RA.
Our data provide new insight into the significance of the measurement of serum IL-6 in patients with RA. Serum IL-6 before treatment might be useful to estimate RA disease activity and to predict responsiveness to TCZ treatment. In addition, serum IL-6 after TCZ but not IFX administration could be a biomarker to evaluate potential disease activity at baseline. We propose that measurement of serum IL-6 concentration is a valuable factor in the selection of TCZ treatment, which is recommended for RA patients with low serum IL-6 concentration.
Acknowledgment
The authors thank Dr. Shirou Fukuhara for scientific advice and Ms. Mihoko Inoue and Ms. Mitsuko Ueda for manuscript preparation.
Footnotes
-
Supported by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology of Japan (grant numbers 21591289 and 24591472), Grants-in-Aid from The Japan Medical Association and Takeda Science Foundation, and Research Grant B from Kansai Medical University.
- Accepted for publication February 25, 2013.








{kind=link}
{kind=link}