

Abstract
Objective. Previously we demonstrated that kynurenic acid (KYNA), an endogenous metabolite of kynurenine, is present in the synovial fluid of patients with rheumatoid arthritis (RA). KYNA inhibits proliferation of synoviocytes in vitro. The goal of our study was to compare KYNA concentrations in synovial fluid and blood of patients with RA, inflammatory spondyloarthropathies (SpA), and osteoarthritis (OA).
Methods. Serum and synovial fluid samples were obtained from 189 patients with RA, 56 patients with SpA, and 32 patients with OA. KYNA was separated using a high-performance liquid chromatography system and measured fluorometrically.
Results. KYNA concentration in synovial fluid obtained from patients with RA and SpA was significantly lower than that in patients with OA (p < 0.05). The concentration of KYNA in serum of patients with RA, SpA, and OA did not differ among all groups studied. The positive correlation between KYNA content in synovial fluid and serum was found in patients with RA (p < 0.05). Univariate linear regression analysis demonstrated that fibrinogen was significantly associated with KYNA in synovial fluid (p < 0.05), and red blood cell counts, morning stiffness, and pain scores were significantly associated with KYNA level in serum (all p < 0.05). Multivariate regression analysis revealed correlation between the following independent variables: hemoglobin level, hematocrit, red blood cell count in conjunction with age and KYNA content in synovial fluid. A lack of correlation was observed between KYNA content in synovial fluid of patients with RA and other clinical and laboratory measures of disease activity.
Conclusion. Our data show a local deficit of KYNA in inflammatory states.
Rheumatoid arthritis (RA) is a chronic, progressive, inflammatory, systemic autoimmune disease leading to progressive destruction of joint cartilage and bone. It is accompanied by swelling of the joints, chronic pain, fatigue, loss of function, disability, and an increased risk of coronary heart disease and premature death. RA affects about 1% of the general population1,2.
The spondyloarthropathies (SpA) are a group of arthritic disorders that share several common features such as inflammation of the spine and peripheral joints. SpA is characterized by ankylosing spondylitis, psoriatic arthritis, reactive arthritis, spondyloarthropathy associated with inflammatory bowel disease, and undifferentiated spondyloarthropathy. Additionally, numerous patients experience inflamed areas in eye, genital tract, or skin. A high percentage of people with these diseases share a similar gene, HLA-B273,4.
Osteoarthritis (OA) is a progressive, noninflammatory, disabling disorder characterized by degenerative joint cartilage destruction. Symptoms are joint pain, tenderness, stiffness, locking, and joint effusion. OA becomes more common with age5.
Despite longterm, intensive investigation, the etiology and pathogenesis of RA and SpA have not been fully elucidated. Multiple genetic, immune, and environmental factors are thought to interact, triggering disease onset2,6,7,8. To date, the focus has been on the immune system and on the pivotal role of T lymphocytes and monocytes in the pathogenesis of RA9. Further, B cells were found to play an important role in the pathophysiology of RA10,11, and evidence has accumulated that the inflammatory process in the synovial tissue is dominated by activated fibroblasts12,13. It was suggested that the synovial fibroblast may be a key agent in joint destruction and matrix remodeling in inflammatory synovitis12,13.
The kynurenine pathway of tryptophan metabolism has been implicated in the pathogenesis of inflammation. It is widely accepted that the activity of indolamine 2,3-dioxygenase (IDO), a rate-limiting tryptophan-degrading enzyme, is stimulated by the proinflammatory cytokines tumor necrosis factor-α and interferon-γ. Kynurenic acid (KYNA) is an endogenous metabolite of kynurenine with intriguing pharmacological properties. It is a broad-spectrum glutamate antagonist14, a noncompetitive alpha7 nicotinic receptor antagonist15, and an agonist of G protein-coupled receptor GPR3516. In a previous study, we demonstrated that KYNA is present in synovial fluid of patients with RA. We also showed that KYNA inhibits proliferation of synoviocytes in vitro and enhances the antiproliferative action of nonsteroidal antiinflammatory drugs17. Here we extend our study and investigate the KYNA content in synovial fluid and blood of RA, SpA, and OA patients. Moreover, we determined the correlation between KYNA content and selected clinical and laboratory data related to disease status and progression.
MATERIALS AND METHODS
Patients
Two hundred seventy-seven white patients (189 with RA, 56 with SpA, and 32 with OA) treated in the Department of Rheumatology and Connective Tissue Diseases, Medical University of Lublin, were enrolled. The study was approved by the Ethical Committee of the Medical University of Lublin and written informed consent was obtained from patients. All patients fulfilled international criteria for these diseases: the patients with RA fulfilled the 1987 American College of Rheumatology (ACR) criteria for diagnosis of RA18, the patients with SpA fulfilled the European Spondylarthropathy Study Group (ESSG) criteria for SpA19, and patients with OA met the 1986 ACR criteria for symptomatic knee OA20.
Patients who had arthrocentesis of the knee within 3 months before sampling of synovial fluid for KYNA determination were excluded from the study.
Laboratory tests
The following laboratory measurements were performed as part of routine clinical practice: erythrocyte sedimentation rate (ESR, Westergren method, mm/h), C-reactive protein (CRP, nephelometry, mg/l; normal < 5 mg/l), morphology of peripheral blood (hemoglobin, hematocrit, red blood cells, white blood cells, platelets), biochemical variables in serum (total protein, albumin, fibrinogen), rheumatoid factor (by ELISA; positive result > 10 U/ml), anticitrullinated protein antibodies (ACPA; by ELISA; positive result > 5 RU/ml).
Clinical assessment of RA activity
The clinical evaluation was performed by experienced rheumatologists. The following clinical variables were recorded: morning stiffness (min), pain score [visual analog scale (VAS); range 0–100 mm], tender joint count (range 0–28), swollen joint count (range 0–28) and Disease Activity Score (DAS28).
Blood and synovial fluid collection
Synovial fluid samples were obtained by sterile aspiration from knees of all studied patients when aspiration was indicated as part of routine clinical practice. Total white blood cell count, lymphocyte count, neutrophil count, and albumin and total protein concentrations were determined in synovial fluid. The samples for KYNA determination were stored at −80°C until used. Venous blood samples were obtained as part of routine clinical practice. Samples were centrifuged at 2000 rpm for 10 min. Serum was collected and frozen at −80°C until used.
Kynurenic acid determination
Proteins were precipitated and removed by centrifugation at 10,000 rpm for 10 min. Supernatants were applied to cation-exchange columns (Dowex 50 W+). KYNA content in serum and synovial fluid was measured using a high-performance liquid chromatography system with fluorescence detection (excitation 334 nm; emission 398 nm).
Data analysis
Data are expressed as mean ± standard error (SEM). Statistical analysis of data was performed using ANOVA with posthoc Dunnett testing. The determination of correlations was performed with univariate and multivariate linear regression (SPSS software). P values < 0.05 were considered statistically significant.
RESULTS
The demographic characteristics of the 3 study groups are summarized in Table 1. The majority of patients were female in RA (85.2%) and OA (81.3%) and male (60.7%) in the SpA group. The average ages were 53.0, 41.4, and 63.5 years in RA, SpA, and OA groups, respectively. The differences were statistically significant. The average disease duration did not differ between groups. The average height of patients with RA and OA was less than that of patients with SpA. The average weight of patients with OA was greater than that of patients with RA or SpA. The average body mass index (BMI) value was lowest in patients with SpA and highest in patients with OA.
Demographic characteristics of patients with rheumatoid arthritis (RA), spondyloarthropathy (SpA), and osteoarthritis (OA). Data are expressed as mean ± SEM.
The values of serological measures of the study groups are summarized in Table 2. The average values of ESR, CRP, white blood cell count, and platelet count did not differ in the RA and SpA groups and were higher in comparison to those of the OA group. The average hemoglobin level and hematocrit values were lowest in RA, moderate in SpA, and highest in OA. Fibrinogen content was lowest in OA, moderate in SpA, and highest in RA. Values for red blood cell counts and serum albumin content did not differ in SpA and OA patients, and were higher in comparison to RA patients.
Laboratory measurements, clinical findings, and content of kynurenic acid (KYNA) in synovial fluid and serum of patients with rheumatoid arthritis (RA), spondyloarthropathy (SpA), and osteoarthritis (OA). Data are mean ± SEM.
Presence of KYNA was detected in all samples of synovial fluid studied. The mean concentrations of KYNA in patients with RA, SpA, and OA were 18.88, 21.46, and 30.52 pmol/ml, respectively. The concentrations of KYNA in synovial fluid samples from patients with RA and SpA were significantly lower than those in OA patients (p < 0.05). The KYNA content in synovial fluid in RA and SpA patients was lower than the measures in serum (p < 0.05). There was no difference between the content of KYNA in synovial fluid and that in serum in patients with OA. The concentration of KYNA in serum did not differ among all the study groups (Table 2).
There was no difference in KYNA content in synovial fluid and in serum in patients with RA classified according to the Steinbrocker criteria21, stage I–IV. The content of KYNA in synovial fluid (20.24 ± 1.60 pmol/ml for Steinbrocker stage II patients; 18.14 ± 0.68 pmol/ml for stage III patients; and 19.86 ± 1.20 pmol/ml for stage IV patients) was lower than that in serum samples (31.13 ± 2.16, 30.46 ± 1.64, and 31.95 ± 3.32 pmol/ml, respectively) in patients with RA (p < 0.05).
There was no difference in KYNA content in synovial fluid and in serum in patients with RA classified according to the presence of rheumatoid factor (RF). The content of KYNA in synovial fluid (18.67 ± 0.76, 20.13 ± 1.07 pmol/ml) was lower than that in serum (30.29 ± 1.61, 31.39 ± 1.84 pmol/ml), in both RF-positive and RF-negative patients, respectively (p < 0.05).
There was no difference in KYNA content in synovial fluid and in serum in patients with RA classified by the presence of ACPA. The content of KYNA in synovial fluid (19.34 ± 0.85, 19.36 ± 1.56 pmol/ml) was lower than in serum (28.13 ± 1.30, 32.06 ± 3.01 pmol/ml) in both ACPA-positive and ACPA-negative patients, respectively (p < 0.05).
There was no difference in KYNA content in synovial fluid and in serum in RA patients classified according to DAS28 values. That is, the content of KYNA in synovial fluid was lower than that in serum in patients with low, moderate, and disease high activity (p < 0.05; Table 3).
Content of kynurenic acid (KYNA) in synovial fluid and serum of patients with rheumatoid arthritis (RA) classified according to DAS28 value. Data are mean ± SEM.
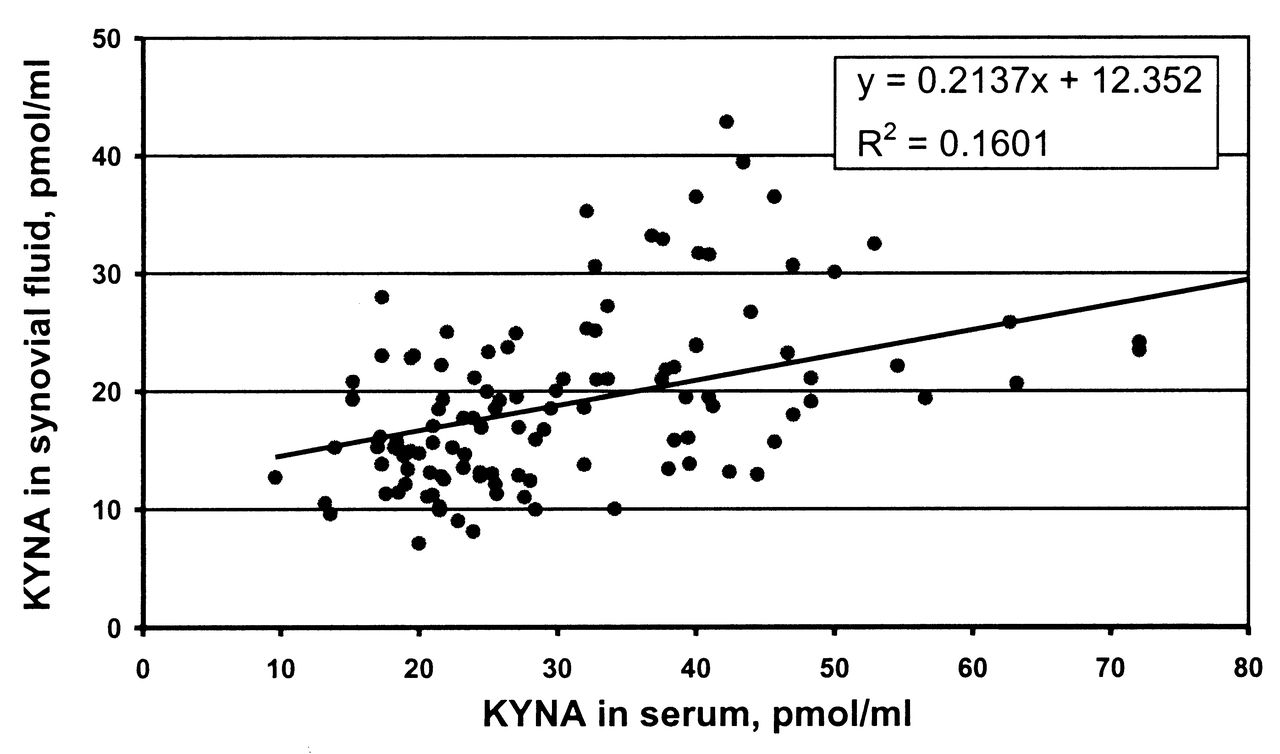
A positive correlation between KYNA content in synovial fluid and in serum was found in RA patients (p < 0.05; Figure 1). Univariate linear regression analysis demonstrated that sex, age, disease duration, weight, BMI, ESR, CRP, hemoglobin level, hematocrit value, red blood cell count, white blood cell count, platelet count, total serum protein, serum albumin, tender joint count, swollen joint count, and DAS28-ESR were not significantly associated with KYNA content in either synovial fluid or serum in patients with RA (Table 4). Fibrinogen was significantly associated with KYNA level in synovial fluid (p < 0.05; Table 4). Red blood cell count, morning stiffness, and pain scores were significantly associated with the KYNA level in serum (all p < 0.05; Table 4). Multivariate regression analysis revealed correlations between the independent variables hemoglobin level, hematocrit, and red blood cell count, in conjunction with age and KYNA content in synovial fluid. There was no correlation between KYNA content in synovial fluid of patients with RA and any clinical or laboratory disease activity measures (as described in Materials and Methods).

Correlation of kynurenic acid (KYNA) content in synovial fluid and serum of patients with rheumatoid arthritis (RA). Solid line represents trend.
Correlations between demographic data, selected laboratory measurements, and clinical findings and kynurenic acid (KYNA) content in synovial fluid or serum of patients with rheumatoid arthritis (RA) according to a univariate model of linear regression analysis.
DISCUSSION
We found that the content of KYNA among blood samples from patients with RA, SpA, or OA did not vary. Nevertheless, the concentration of KYNA in synovial fluid was lower in RA and SpA patients in comparison to patients with OA. The determination of KYNA in synovial fluid from healthy controls was not possible for ethical reasons. Importantly, the content of KYNA in patients with RA or SpA was also lower in synovial fluid than in blood. In patients with OA, the concentration of KYNA in synovial fluid and plasma did not differ.
Similar results were reported originally in the publication by Igari and Tsuchizawa in 196922 and were repeated by Igari, et al in 198723. Although that study was performed on small groups of 5 subjects each, a significantly lower concentration of KYNA in synovial fluid was found in patients with RA in comparison to patients with OA. However, it should be noted that the mean amount of KYNA in synovial fluid reported by Igari was 4.29 and 9.54 μg/ml in RA and OA patients, respectively, which was more than 1200 times higher than the amount observed in our study. Since the content of KYNA found in serum in our study corresponds well with the results of others24, it seems that the difference is due to the less precise analytical methods available in the 1960s.
KYNA content has been determined in blood and tissue in numerous inflammatory diseases. In contrast to our findings, an increase of KYNA content was found in human blood in conditions of sepsis25, HIV-1 infection26, and chronic kidney disease27. Locally, an increase of KYNA was found in cerebrospinal fluid of patients with tick-borne encephalitis28, HIV-126,29,30, and other bacterial, viral, fungal and parasitic infections of the central nervous system31. In our study, the content of KYNA in synovial fluid was lower in the inflammatory diseases RA and SpA in comparison with noninflammatory OA. A reduced level of KYNA was reported in cerebrospinal fluid of patients with relapsing-onset multiple sclerosis during remission32 and in blood of patients with irritable bowel syndrome33. It should be emphasized that in our study the content of KYNA in serum did not differ between the groups of patients with inflammatory and noninflammatory rheumatic diseases. The weak positive correlations between KYNA content in synovial fluid and serum and synovial fluid and age were found in patients with RA. Moreover, univariate linear regression analysis demonstrated that fibrinogen was significantly associated with KYNA levels in synovial fluid, whereas red blood cell counts, morning stiffness, and pain scores were significantly associated with KYNA levels in serum. Multivariate logistic regression analysis showed correlation between KYNA content in synovial fluid and age, and hemoglobin level, hematocrit, and red blood cell count. No other correlations between KYNA content in synovial fluid and laboratory values measured in blood and synovial fluid were detected. No difference in KYNA content in synovial fluid and in serum was found in patients with RA classified according to DAS28 value or the score by Steinbrocker criteria. These findings point to the local phenomenon. The reason for the reduction in KYNA content in the synovial space in inflammatory diseases remains unknown. KYNA is catalyzed from kynurenine by kynurenine aminotransferases (KAT). The activity of KAT in constituents of synovium has never been investigated. Thus, reduced expression of KAT in patients with RA and patients with SpA cannot be ruled out. In addition to this expression issue, other mechanisms should be considered.
It has been documented that KYNA production depends on precursor availability. However, the kynurenine content in synovial fluid of RA patients was found to be not lowered, but distinctly elevated22,23,34,35. Kynurenine is formed from tryptophan by the activity of IDO. It was found that dendritic cells and tissues from synovial joints of patients with RA expressed higher levels of IDO in comparison to healthy sample donors36, and that the activity of the enzyme was elevated in the synovial membrane and synovial fluid in RA23,37. Tryptophan level has been reported to increase or decrease in RA synovial fluid23,37. The kynurenine level in synovial fluid obtained from patients with septic arthritis was higher compared with samples from patients with noninfectious inflammatory arthropathy or OA35. There is no evidence for reduced content of KYNA precursors in RA synovial fluid in the literature; therefore, this seems not to be the reason for the low level of KYNA that was observed.
Another scenario to be considered is the regulation of KYNA production at the level of KAT activity. It was demonstrated that KYNA production can be affected by numerous substances. In the medium deprived of glucose, KYNA synthesis was diminished in rat cortical slices but unaffected in liver and kidney slices38. Glutamate inhibited production of KYNA in brain and spinal cord slices39,40,41. High level of homocysteine reduced production of KYNA in rabbit hippocampus42, rat cortical slices41,42, rat aortic rings in vitro43, and cultured bovine aortic endothelial cells44.
Interestingly, it was found that glucose content is reduced in synovial fluid of patients with RA45 and the concentration of homocysteine is enhanced46. Glutamate was found to be released to the knee joint in a rat model of arthritis47, and was remarkably elevated in synovial fluid of patients with RA48. The possible involvement of glutamatergic signaling in the pathogenesis of joint diseases such as RA was recently reviewed34. Thus, it seems plausible that the local regulation of KYNA synthesis determines its level in synovial fluid.
The role of KYNA in tissue of the joint cavity remains unknown. KYNA is an antagonist of ionotropic glutamate receptors14. The presence of glutamate receptors on synovial joint tissue has been reported and the role of glutamate in nociception and inflammatory mechanisms was suggested34,35,47,49,50. The effect of the glutamate antagonists KYNA and memantine was investigated in collagen-induced arthritis in DBA/1 mice. It was found that memantine ameliorates and delays the development of arthritis, but KYNA does not51. The lack of influence of KYNA can be attributed to a very low dose (2.5 mg/kg) used in that study51. On the other hand, doses of KYNA in the range of 25–500 mg/kg were used by others52,53,54,55.
KYNA is also an agonist of the orphan G protein-coupled receptor GPR35, which is predominantly detected in immune cells16. There is growing evidence that KYNA possesses antiinflammatory and antioxidative activity. Because RA is a chronic inflammatory disease characterized by synovial hyperplasia leading to joint destruction56, it is remarkable that both KYNA and its immediate precursor kynurenine possess antiproliferative activity. Kynurenine was found to inhibit proliferation of the chondrocyte cell line ATDC535. As we reported, KYNA inhibited proliferation of rabbit synoviocytes and enhanced the antiproliferative action of the antirheumatic drugs celecoxib and nimesulide17. Later studies showed that KYNA inhibits the proliferation and viability of colon cancer cells in vitro57, and the proliferation, DNA synthesis, and migration of renal cancer Caki-2 cells58.
We have documented that KYNA is a constituent of synovial fluid in patients with RA, SpA, or OA and that its level in synovial fluid is lower in RA and SpA in comparison with OA. Unique pharmacological properties of KYNA predispose this compound as a potential regulator of inflammatory processes in arthritic joints.
Footnotes
-
Supported by the State Committee for Scientific Research (Poland), grant 2P05A03827.
- Accepted for publication February 4, 2013.








{kind=link}