

Abstract
Objective. We investigated changes in high-density lipoprotein (HDL) profiling in patients with rheumatoid arthritis who started treatment by taking tumor necrosis factor (TNF) inhibitors. The patients were stratified for European League Against Rheumatism (EULAR) response.
Methods. A group of 100 patients naive for TNF inhibitors at baseline were randomly selected from 204 adalimumab-treated and 203 etanercept-treated patients on the basis of their EULAR response. HDL profiling was measured using surface-enhanced laser desorption/ionization time-of-flight mass spectrometry.
Results. In EULAR good responders, mass charged markers representing serum amyloid A (SAA-1 and -2) decreased significantly after 4 months’ therapy. There were no significant differences in HDL profiling in EULAR nonresponders.
Conclusion. Effective suppression of inflammation with TNF inhibitors results in favorable changes in HDL composition.
- RHEUMATOID ARTHRITIS
- HIGH-DENSITY LIPOPROTEINS
- LIPID PROFILE
- TUMOR NECROSIS FACTOR INHIBITORS
- CARDIOVASCULAR RISK
There are abundant data that rheumatoid arthritis (RA) is associated with an increased cardiovascular (CV) risk1. Multiple studies have shown that tumor necrosis factor (TNF) inhibitors reduce the CV risk in patients with established RA2. Suppression of inflammation, e.g., as a result of antiinflammatory treatment with TNF inhibitors, leads to increased high-density lipoprotein (HDL) levels, but also to increased total cholesterol (TC) levels with virtually no change in the TC/HDL ratio3, an important predictor of CV events4. Hence, the atheroprotective effect of TNF inhibitors appears not to be mediated by quantitative changes in the lipid profile.
Data indicate that TNF inhibitors induce structural changes in lipid but also protein composition, such as decreasing levels of the atherogenic serum amyloid A (SAA) within HDL particles5. These findings are important because they may explain the beneficial effect of anti-TNF treatment on CV risk.
We investigated the changes in HDL profiling in patients with RA who started treatment with TNF inhibitors. The patients were stratified for European League Against Rheumatism (EULAR) response.
MATERIALS AND METHODS
From 2 simultaneously running prospective cohorts at the Rheumatology Department of the Jan van Breemen Research Institute | Reade, Amsterdam, 100 patients with RA who were TNF-naive at baseline were randomly selected. Treatment allocation was at the discretion of the treating rheumatologist. The etanercept RA cohort comprised 203 patients and the adalimumab RA cohort comprised 204 patients. To distinguish between patients with low-grade and high-grade inflammation, only patients with sustained EULAR good or nonresponse at 1 and 4 months of TNF-blocking therapy were included, and moderate responders were excluded. Etanercept-treated patients were matched to adalimumab-treated patients for age, sex, disease duration, and baseline Disease Activity Score. In total, 50 EULAR good responders and 50 EULAR nonresponders were enrolled in our study. Clinical data and blood samples were collected at baseline and after 1 and 4 months of therapy.
The study was approved by the local Medical Ethics Committee and all patients gave written informed consent.
Assessment of lipids and HDL protein profiling
TC and triglycerides (TG) were measured by enzymatic methods using clinical chemistry analyzers. HDL was determined enzymatically with PEG-modified enzymes. Direct low-density lipoprotein (LDL) measurement was done with a kit from Wako Chemicals. Apolipoproteins (apo) were measured by an immunoturbidimetric method, using assays supplied by Randox Laboratories Limited. TC/HDL ratio and apoB/apoA-I ratios were calculated.
HDL profiling was assessed with surface-enhanced laser desorption/ionization time-of-flight mass spectrometry (SELDI-TOF-MS)6,7.
HDL-associated proteins were measured directly from fresh frozen plasma and non-HDL components were eliminated using anti-apoA-I antibodies. SELDI-TOF-MS analysis was performed with a PBS IIc protein chip reader using an automated data collection protocol within protein-chip software. Data were collected up to 200 kDa. Laser intensity was set in a range from 190 to 220 relative units and the focus mass was set to 28 kDa for anti-apoA-I capture. Protein spectra were measured with about 100 shots at 13 positions per SELDI spot. The sensitivity of detection was set at signal/noise ratio > 5. Statistical analyses were performed using SPSS version 16.0. The differences between groups were tested using independent t test, chi-square test, or Mann-Whitney U test, as appropriate.
RESULTS
Clinical and demographic characteristics of all patients are shown in Table 1. There were no significant differences between etanercept- and adalimumab-treated patients (data not shown).
Demographic and clinical characteristics at baseline. Mean values (SD), or mean ± SD, or count (percentage) are shown unless indicated.
Absolute changes in lipid levels were assessed using generalized estimating equation analysis. HDL and apoA did not change in EULAR nonresponders. In the EULAR good responders, however, HDL and apoA-II increased significantly after 1 and 4 months of therapy (Table 2).
Changes in lipid levels according to EULAR response at 1 and 4 months of therapy.
At baseline there were no significant differences in HDL profiling between EULAR good responders and nonresponders. In total, 14 out of 133 mass charge markers changed during therapy, of which 4 were associated with SAA-1 and -2 (11092, 11540, 11696, 11750 m/z)7. After 1 month of therapy, marker 11750 was significantly higher in nonresponders compared to good responders (p = 0.036; Appendix 1 and Appendix 2). After 4 months of therapy, all markers representing SAA-1 and -2 were significantly higher in nonresponders than in good responders (all p < 0.05).
In addition, dynamics in markers associated with SAA-1 and -2 were assessed in EULAR good and nonresponders. SAA did not change in nonresponders at both 1 and 4 months of therapy. In contrast, in good responders after 1 month of therapy, marker 11750 decreased significantly compared to baseline (p < 0.05), whereas a clear decreasing trend in signal was observed in the other 3 markers. After 4 months of therapy, markers 11092, 11540, 11696 (p < 0.05), and 11750 (p < 0.001) decreased significantly compared to baseline (Figure 1).
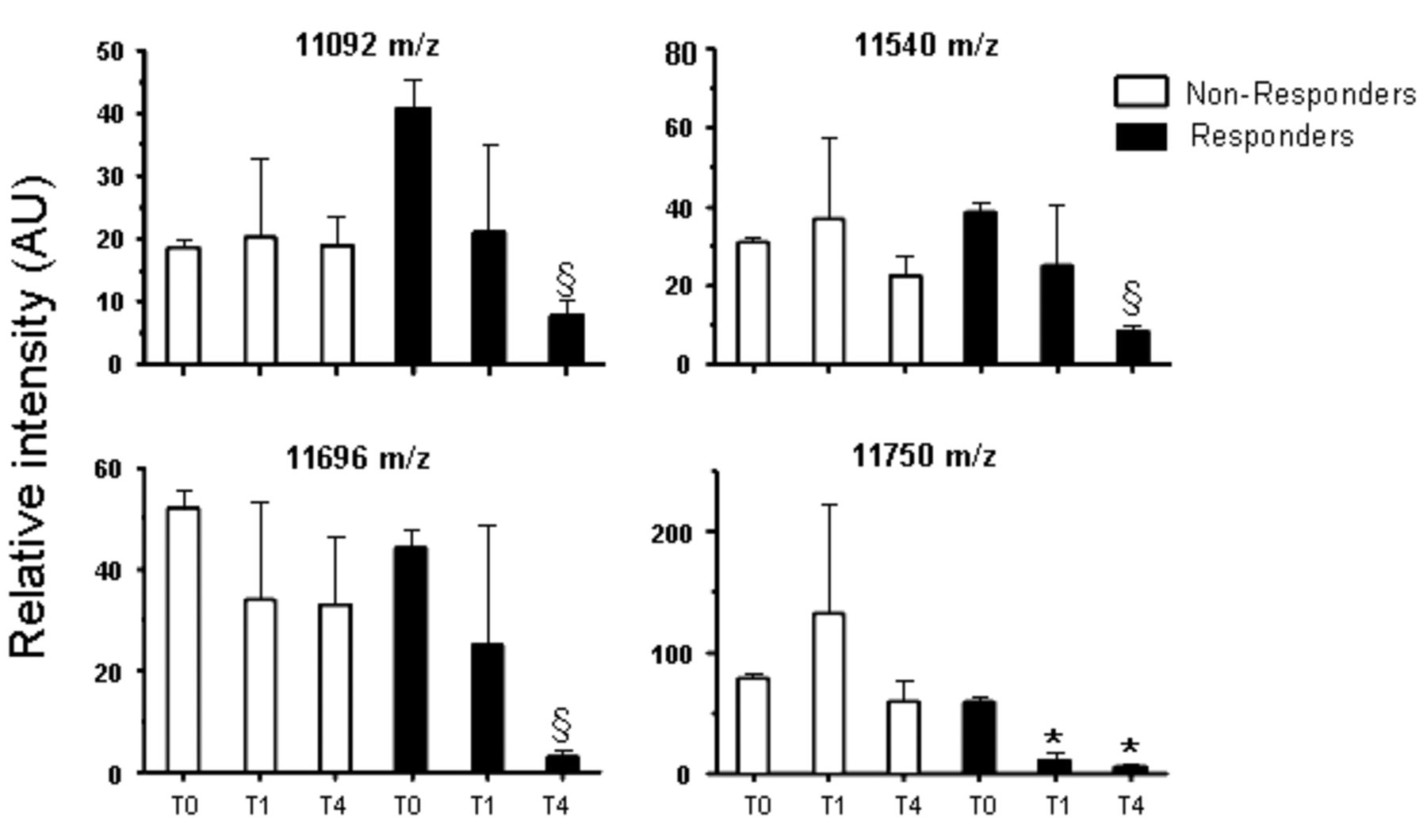
Dynamics of the serum amyloid A (SAA)-1 and -2 markers stratified for EULAR response. The mean values (± 1 SD) of the 4 markers correspond with the SAA isoforms as present in the nonresponders and responders. The corresponding timepoints are baseline (T0), 1 month (T1), and after 4 months after the start of therapy (T4). §p < 0.05, *p < 0.001 using 1-way ANOVA with Bonferroni multiple comparison. AU: arbitrary unit.
DISCUSSION
Our study reaffirms the beneficial effect of TNF inhibitors on structural changes in HDL protein composition5,8 and demonstrates, to our knowledge for the first time, that these findings apply only to RA patients with a good EULAR response, because HDL profiling did not change in EULAR nonresponders.
There is strong evidence that HDL is atheroprotective, although during inflammation the HDL protein composition changes, rendering HDL to a proinflammatory and atherogenic state9. For example, in response to inflammation, SAA replaces apoA-I from the HDL particle, resulting in a decreased ability of HDL to protect LDL from oxidation10.
The CV risk reduction by TNF inhibitors in patients with RA appears not to be mediated by quantitative changes of the lipids, because the effect on the atherogenic index is very modest3. Our data suggest that atheroprotective changes in HDL particle are the consequence of inflammation reduction by potent anti-TNF therapy. This was illustrated by the mass charge markers representing HDL-associated SAA-1 and -2, because these markers decreased significantly in good EULAR responders but did not change in EULAR nonresponders.
Inherent to the design of our study, selection bias should be taken into account. Moreover, the SELDI-TOF-MS approach was used to assess HDL profiling because of its strong applicability in high-throughput sample measurement. This method has limitations such as lack of direct protein identification6. However, protein profiling and not protein identification was the major objective in our study, justifying this approach.
Despite the limitations, our study clearly demonstrates that successful reduction of inflammation in RA patients with anti-TNF therapy restores the HDL protein composition to an atheroprotective profile, underscoring the need for tight inflammation control in patients with RA, to decrease the CV risk. However, it remains to be determined in longterm prospective studies whether these changes in the HDL protein composition translate into meaningful reduction of CV risk in patients with RA.
Acknowledgment
We are grateful to the Division of Research and Education of the Jan van Breemen Research Institute | Reade, which receives support from the Dutch Arthritis Foundation, for help in conducting the study. We thank the research nurses Marga Kammeijer-Rippen, Anne-Marie Abrahams, Martine Kos, and Astrid Twisk for performing clinical assessments. We also thank Margret de Koning for preparation of the assays.
Appendix 1
Details of mass charge markers in nonresponders (signal in relative units).
Appendix 2
Details of mass charge markers in responders (signal in relative units).
Footnotes
-
Supported by Pfizer (Wyeth) Pharmaceuticals and Abbott Laboratories; and facilitated by the Division of Research and Education of the Jan van Breemen Research Institute | Reade. Dr. Nurmohamed has received consultancy fees from Abbott, Roche, Pfizer, MSD, UCB, BMS, and Wyeth, and payment for lectures from Abbott, Roche, and Pfizer.
- Accepted for publication February 22, 2013.








{kind=link}