

Abstract
Objective. Tumor necrosis factor (TNF) receptor 1–associated periodic syndrome (TRAPS) is an autoinflammatory disorder caused by autosomal dominantly inherited mutations in the TNF receptor superfamily 1A (TNFRSF1A) gene. The D12E substitution has been described only once to date, in a 4-year-old boy with fever.
Methods. For DNA sequence analysis of the TNFRSF1A gene, genomic DNA was isolated, amplified by PCR, purified, and sequenced.
Results. We describe 3 families (8 subjects) with the TNFRSF1A D12E substitution and TRAPS-related symptoms, in 4 cases associated with the autoimmune diseases multiple sclerosis and rheumatoid arthritis.
Conclusion. The clinical phenotype might be associated with the TNFRSF1A D12E mutation. There is a close pathophysiological relationship between TNF signaling and autoimmune disorders.
- TNF RECEPTOR SUPERFAMILY 1A GENE
- RHEUMATOID ARTHRITIS
- PHENOTYPE
- TNF RECEPTOR 1–ASSOCIATED PERIODIC SYNDROME
- GENOTYPE
- MULTIPLE SCLEROSIS
Tumor necrosis factor receptor 1-associated periodic syndrome (TRAPS) is an autosomal dominantly inherited autoinflammatory disorder caused mainly by mutations in exons 2, 3, 4, or 6 of the tumor necrosis factor (TNF) receptor superfamily 1A (TNFRSF1A) gene located on chromosome 12p13, which encodes the 55-kDa receptor for TNF-α1,2. TRAPS is characterized by recurrent, self-limiting attacks of fever, abdominal pain, myalgia, rash, arthralgia/arthritis, and rhinolaryngeal involvement with pharyngitis, as well as conjunctivitis and periorbital edema. More than 80 different TNFRSF1A mutations with a heterogeneous symptom spectrum have been identified to date3,4. The D12E substitution is a missense mutation that has been described only once to date, in a 4-year-old boy who experienced up to 60 fever episodes per year of 3 days’ duration each since the age of 1 year5. We describe 3 additional index cases and 5 family members also carrying the D12E exchange in heterozygous form.
MATERIALS AND METHODS
All individuals were seen in our outpatient clinic at the Institute for Clinical Neuroimmunology in Munich, Germany. All subjects/parents gave their written informed consent prior to the genetic testing, according to the Declaration of Helsinki. For DNA sequence analysis of the TNFRSF1A gene, genomic DNA was isolated, amplified by PCR, purified, and sequenced.
RESULTS
We identified 3 index cases and 5 additional family members who were heterozygous for the D12E/p.Asp41Glu substitution encoded by exon 2 of the TNFRSF1A gene. Clinical characteristics are shown in Table 1 and Figure 1. Seven of the 8 subjects (87.5%) presented with typical TRAPS-related health problems. The leading symptoms were arthralgias/arthritis (75%), followed by abdominal pain (50%). In 6 patients, laboratory testing was available and showed an intermittent elevation of acute-phase response markers in 5 of them. In 4 of our 8 patients, concomitant autoimmune diseases were present [4 with the relapsing-remitting form of multiple sclerosis (RRMS) and 1 with additional rheumatoid arthritis (RA); Figure 2]. Index patient 3 also tested positive for a heterozygous, combined P369S/R408Q mutation encoded by exon 3 of the MEFV gene. Because her symptoms (arthralgias/arthritis, myalgias) responded to steroid but not to colchicine therapy, her rheumatological symptoms were attributed to the TNFRSF1A D12E mutation.

DNA sequence electropherograms of TNF receptor superfamily 1A exon 2 from a control (left) and index Patient 2 (right).
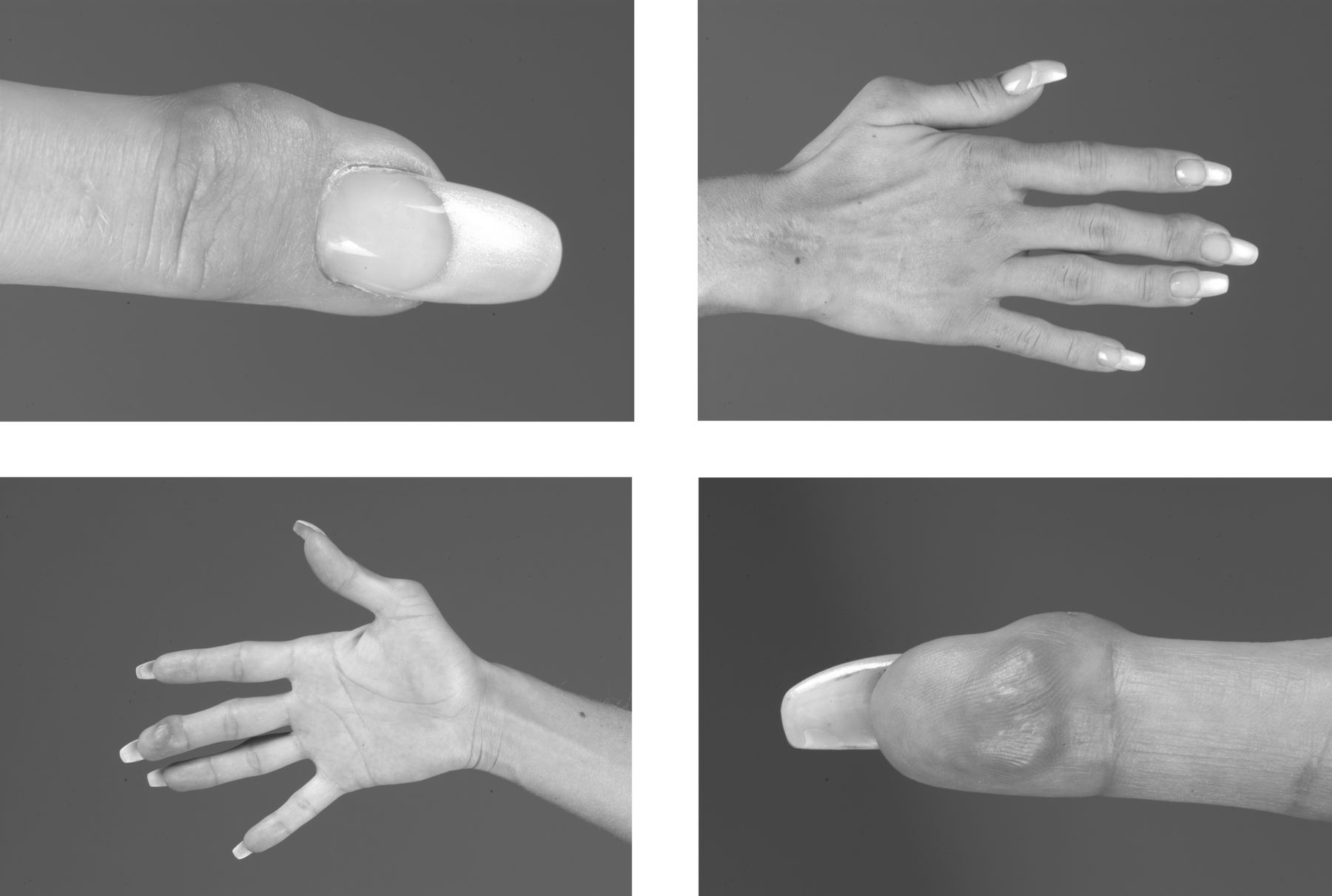
Joint destruction in index case 2.
Clinical characteristics of the mutation-positive patients.
Through genetic analyses in > 3000 patients with symptoms suggestive of an autoinflammatory disease, this alteration was detected to date in only 5 individuals, including the 3 index patients presented here (P. Lohse, unpublished observations). This argues against D12E being a common variant. Other exchanges were not observed at this amino acid position.
DISCUSSION
To our knowledge, there is only 1 patient with a TNFRSF1A D12E substitution and TRAPS-related fever described to date5. We described another 3 index cases as well as 5 additional family members carrying the D12E substitution, 7 of them presenting with TRAPS-related symptoms [mainly arthritis/arthralgia, diarrhea, and/or abdominal pain (Table 1)]. Overall, the phenotypes were mild with only slight elevations of acute-phase response markers and without signs of renal disease.
An association between autoinflammatory syndromes and autoimmune diseases has been investigated. The TNFRSF1A R92Q mutation is frequently observed in patients with RA6 and has been identified as a new susceptibility factor for MS, while the D12E exchange has not been described to date in patients with MS7,8. Four of the mutation carriers were diagnosed with RRMS and 1 patient had additional RA, supporting the view that TNFRSF1A mutations exert a proinflammatory role in autoimmune diseases, although the exact pathophysiological mechanisms are not completely understood. A few of the mutations interfere with the shedding of the TNF receptor 1 from the cell membrane into the extracellular compartment, thereby reducing its ability to neutralize TNF-α by binding5,9,10. Other genetic defects alter the 3-dimensional structure of the protein, resulting in misfolding of the extracellular receptor domain and in retention of the mutated TNFR1 in the endoplasmic reticulum11,12. Recently, it has also been shown that TRAPS mutants with major structural changes increase the mitochondrial production of reactive oxygen species, leading to sustained mitogen-activated protein kinase activity and thereby enhancing innate immune responses13. This could be an important common pathophysiological pathway in TRAPS patients with additional autoimmune diseases. However, because the TNFRSF1A D12E substitution has not been investigated in detail to date and PolyPhen-2 analysis predicts that it is a benign mutation, it remains unclear how this exchange contributes to the observed clinical phenotypes.
We have identified 8 subjects carrying the TNFRSF1A D12E substitution who displayed TRAPS-related symptoms. The mutation may enhance the inflammatory response, thereby contributing to the manifestation of MS and RA in 4 mutation carriers. This cohort thus highlights the close pathophysiological relationship between TNF signaling, TRAPS, and autoimmune diseases such as RA and MS.
Acknowledgment
Sabine Pitter provided excellent technical assistance.
Footnotes
-
Dr. Hohlfeld is supported by the Deutsche Forschungsgemeinschaft (SFB 571) and has received personal compensation from Bayer-Schering Pharmacy, TEVA, Merck-Serono, Biogen-Idec, and Novartis. Dr. Havla and Dr. Gerdes have received travel expenses and personal compensation from Merck-Serono, TEVA, Bayer-Schering, Novartis, and Biogen-Idec. Dr. Kümpfel has received travel expenses and personal compensation from Bayer-Schering Pharmacy, TEVA, Merck-Serono, and Biogen-Idec as well as grant support from Bayer-Schering AG.
- Accepted for publication November 27, 2012.








{kind=link}
{kind=link}