

Abstract
Objective. Citrullination, a reaction converting arginine residue into citrulline residue, is essential for autoimmunity of rheumatoid arthritis (RA). We conducted 2-dimensional Western blot analyses (2-D WB) to screen for novel citrullinated proteins in synovial tissues from patients with RA.
Methods. Total proteins were extracted from the synovial membranes of patients with RA (n = 10) and pooled. Four identical 2-D electrophoresis (2-DE) gels were prepared, and 2 gels were transblotted to polyvinylidene fluoride membranes that were separately probed with sera from patients with RA (n = 10) or an anticitrulline antibody. The protein profiles of the 2-DE gels were compared with the hybridization results on a global level. The immunoreactive protein spots were collected from the 2-DE gels and identified using mass spectrometry. Proteins that were detected by both RA sera and anticitrulline antibody were considered citrullinated proteins. The result was confirmed through routine WB, immunoprecipitation, and ELISA. Autoantibodies against these potential antigens were also examined in the blood of patients with RA by ELISA.
Results. RA sera and the anticitrulline antibody on 2-D WB detected α-1-antitrypsin (A1AT), dynein heavy-chain 3, fibrinogen β chain, keratin type II cuticular Hb4 (KRT84), lumican, tubulin β-chain (TUBB), and vimentin. A1AT, KRT84, and TUBB had high expression in the synovial membranes (n = 5) of patients with RA and A1AT and KRT84 had high expression in RA synovial fluids (n = 40). A1AT, KRT84, and TUBB immunoprecipitated from synovial tissues showed citrullination. A high level of autoantibodies against KRT84 was detected in the blood of patients with RA (n = 92) compared to that of healthy controls (n = 92).
Conclusion. Our study identified some new citrullinated proteins in RA synovial tissues using 2-D WB.
Rheumatoid arthritis (RA) is an autoimmune disease. Serum from patients with RA contains a spectrum of autoantibodies, such as rheumatoid factor (RF), antifilaggrin autoantibody, antikeratin antibody, antiperinuclear factor, antivimentin, and anticitrullinated protein antibodies (ACPA)1,2,3,4,5. B cell epitopes of most RA autoantibodies contain citrulline, an amino acid that is converted from arginine by posttranslational citrullination6,7,8. This protein modification catalyzed by Ca(2+)-dependent peptidylarginine deiminases has been shown to trigger immune responses including autoantibody generation9,10,11. The most commonly accepted molecular mechanism for citrullinated peptides/proteins in RA is that the modified antigen resulting from cell damage or uncontrolled apoptosis could evoke an immune response leading to autoantibodies against these peptides or the whole protein8. ACPA have recently emerged as sensitive and specific serological markers of RA, providing a superior alternative to the RF test in laboratory diagnostics12,13,14,15,16. Thus citrullination is essential for RA autoimmunity. To date, there have been many reports about screening citrullinated proteins in RA. They found that several proteins following citrullination induce autoimmunity in RA, such as filaggrin, fibrin collagen type II, α-enolase, and vimentin (VIME)2,13,17,18,19,20,21,22,23. However, most of those studies were completed with blood samples and synovial fluids from patients with RA. In our study, we screened the citrullinated proteins by 2-dimensional Western blotting (2-D WB). The 2-D WB result was confirmed by immunoprecipitation, WB, and ELISA within the synovial membranes and synovial fluids. ELISA was also used to determine the presence of autoantibodies against the candidate proteins in blood from the patients with RA. We aimed to identify citrullinated proteins in synovial tissues of patients with RA.
MATERIALS AND METHODS
Tissue collection
Synovial tissue samples were collected during knee joint replacement surgery in patients with RA (n = 10; 7 women and 3 men; ages 33–68 yrs, mean age 53 yrs). The diagnosis of RA fulfilled the American College of Rheumatology (ACR) criteria23. The patients had RA durations of 3–9 years and were classified as having erosive RA (Larsen class IV–V). Most patients with RA had high levels of C-reactive protein (CRP; 30–100 mg/dl, mean 24 mg/dl), ACPA (170–310 U/ml), and RF (80–1300 U/ml). Synovial tissues were also collected during joint replacement surgery for patients with osteoarthritis (OA; n = 10; 4 women and 6 men; ages 40–72 yrs, mean 62 yrs). Their symptoms fulfilled the modified New York criteria. The synovial samples were processed for 2-D WB. Other synovial samples from patients with RA (n = 5) and patients with OA (n = 5) that were independent from the samples used for 2-D WB were processed for WB. The clinical characteristics of the patients are shown in Table 1. The samples were dissected from the connective tissues and immediately stored at −80°C until use.
Clinical characteristics of patients with rheumatoid arthritis (RA) or osteoarthritis (OA).
Synovial fluids were aspirated from the joints of patients with RA (n = 40; 24 women, 16 men; ages 23–73 yrs, mean 44 yrs), OA (n = 30; 16 women, 14 men; ages 47–66 yrs, mean 51 yrs), and ankylosing spondylitis (AS; n = 33; 7 women, 26 men; ages 26–54 yrs, mean 35 yrs).
Blood samples were obtained by standard venipuncture from patients with RA (n = 92; 70 women, 22 men; ages 23–68 yrs, mean 49 yrs). Ninety-two blood samples from healthy volunteers (72 women, 20 men; ages 19–48 yrs, mean 45 yrs) were used as controls. The patients with RA had received their diagnosis at least 3 years prior to the study and had high levels of CRP, ACPA, and RF.
All patients provided written informed consent, and the study protocol was approved by the local institutional ethics committee.
2-D WB analysis
The samples of synovial tissue from the patients with RA were homogenized in lysis buffer (7 M urea, 2 M thiourea, 4% CHAPS, 2% isopropylidene guanosine buffer, 65 mM dithiothreitol, and 1 mM phenylmethylsulfonyl fluoride) with a protease inhibitor cocktail (Sigma) on ice and then centrifuged at 14,000 g for 30 min. The cell lysates from patients with RA (n = 10) were pooled to obtain equal protein contents. Two sets of identical isoelectric focusing were performed using an Ettan IPGphor II instrument (GE Healthcare) with 7-cm Immobiline DryStrip Gels (pH 3–10; GE Healthcare). The protocol has been described in our previous study24. After electrophoresis, 1 gel was visualized by staining with Coomassie Brilliant Blue R350 and scanned with a UMAX PowerLook 2100XL (UMAX Technologies). Digitized images were analyzed with ImageMaster 2D Platinum software 5.0 (GE Healthcare).
Another gel was transblotted to a PVDF membrane using a Mini-Protean 3 vertical electrophoresis cell (Biorad) for the 2-D WB analysis. The 2-D WB analysis was performed using an anticitrulline antibody (Abcam) or sera from the patients with RA at a 1:2000 dilution. Equal volumes of sera were collected from 10 patients and were purified with Montage Antibody Purification Kits (Millipore). The diagnoses of the patients with RA (7 women, 3 men; ages 23–68 yrs, mean 49 yrs) fulfilled the ACR criteria23. The patients with RA had disease durations of 3–10 years, and they had high levels of CRP, ACPA, and RF. All primary and secondary antibodies were diluted in 5% nonfat dry milk in TBST (Tris base 0.02 M, NaCl 0.137 M in distilled water, pH 7.6, and 0.1% Tween 20). Immunoreactive signals were detected with alkaline phosphatase-conjugated secondary antibodies and visualized using the Western Blotting Luminol Reagent (Amersham). Images of the WB were acquired on a Typhoon Trio imager (GE Healthcare).
The protein profiles of 2-DE gels were compared to that of the WB. The immunoreactive spots were excised manually from the stained gels and identified by matrix-assisted laser desorption/ionization time-of-flight/time-of-flight mass spectrometry (MALDI-TOF/TOF MS) analysis.
WB analysis
Two hundred micrograms of the synovial tissues from the patients with RA (n = 5) and OA (n = 5) were homogenized in Cell Lysis Solution (Sigma) and centrifuged at 16,000 g for 5 min at 4°C. These synovial samples were independent from the samples used for 2-D WB. The supernatant was collected after centrifugation, and the protein concentration was determined using the BCA Protein Assay Kit (Pierce). Total protein was separated by sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE) and transblotted to nitrocellulose membranes (Amersham). WB analysis was conducted using antibodies against A1AT (Abcam), dynein heavy-chain 3 (DYH3; Abcam), lumican (LUM; Abcam), keratin type II cuticular Hb4 (KRT84; Lifespan), and tubulin β-chain (TUBB; Abcam). All primary antibodies were diluted 1:4000 in 5% nonfat dry milk in TBST. The secondary antibodies were diluted 1:10,000 in TBST with 5% nonfat dry milk. The immunoreactive signals were detected with alkaline phosphatase-conjugated secondary antibodies and visualized using the WB Luminol Reagent (Amersham). Images of the WB were acquired on a Typhoon Trio imager (GE Healthcare). The protein samples were also probed with a GAPDH antibody to normalize the sample loading.
Immunoprecipitation
Total protein was purified from the synovial tissues of patients with RA (n = 5) using the Total Protein Extraction kit (Biochain) according to the manufacturer’s instructions. A1AT, keratin type II cuticular Hb4, and TUBB were immunoprecipitated from the protein samples using a Protein G Immunoprecipitation kit (Sigma) according to manufacturer’s instructions. Tissue lysates were incubated with the anti-A1AT antibody, the anti-KRT84 antibody, and the anti-TUBB antibody overnight at 4°C. The protein G beads provided with the kit were added to the mixtures and incubated for 2 h at 4°C. After a thorough wash, the extracts were eluted with 1× Laemmli Sample Buffer (Sigma). The concentrations of the immunoprecipitates were determined using the BCA Protein Assay kit (Pierce). Five micrograms of protein were separated by SDS-PAGE and transblotted onto PVDF membranes using a WB apparatus. Two membranes were prepared using an identical protocol. One membrane was probed with antibodies against A1AT, KRT84, or TUBB, and the other membrane was probed with the anticitrulline antibody (Abcam). The immunoreactive signals were detected with alkaline phosphatase-conjugated secondary antibodies and visualized as above.
Detection of the levels of candidate proteins in synovial fluid using ELISA
The synovial fluid samples were centrifuged at 3000 g for 10 min at 4°C. The levels of A1AT, KRT84, and TUBB in the synovial fluid were measured using ELISA. The fluid samples were diluted 50-fold in 0.05 M carbonate-bicarbonate buffer (pH 9.6). Two hundred microliters of diluted fluid was coated onto 96-well microplates (Costar) by overnight incubation at 4°C. After 3 brief washes with phosphate buffered saline (PBS; 8 g NaCl, 0.2 g KCl, 1.15 g NaHPO4, and 0.2 g KH2PO4/l, pH 7.4–7.6) containing 0.1% Tween 20 (PBST), the plate was blocked with 5% nonfat dry milk for 1 h at room temperature. The antibodies against A1AT, KRT84, and TUBB were diluted 5000-fold with PBST, added to the plate, and then incubated for 2 h at room temperature. After 3 washes with PBST, the plate was incubated with a 10,000-fold dilution of anti-rabbit IgG or anti-mouse IgG phosphatase-conjugated antibody (Sigma) for 30 min at room temperature. Following 3 washes with PBST, the signal was developed by adding the alkaline phosphatase yellow (pNPP) liquid substrate system for ELISA. The absorbance of the reaction was measured at 405 nm using a plate reader (Synergy HT, Bio-Tek).
Detecting the levels of novel autoantibodies in the blood of patients with RA using ELISA
Recombinant full-length human A1AT (aa 25–418, 395 amino acids, 44.4 kDa) was obtained from Abcam. The synthetic peptide ESY ITN LRR QLE VLV SDQ ARL QAE RNH LQD VLE GFK KKY EEE VVC RAN AE against KRT84 was conjugated with bovine serum albumin and prepared by Shanghai ImmunoGen Biological Technology. The full-length recombinant protein corresponding to human TUBB was prepared by Origene. The recombinant A1AT protein was diluted in 0.05 M carbonate bicarbonate buffer (pH 9.6) at a concentration of 1 μg/ml, the recombinant tubulin β protein was diluted at 1 μg/ml, and the synthetic peptide of KRT84 was diluted at 2.5 μg/ml. These synthetic proteins were coated onto 96-well EIA/RIA microtiter plates (Costar) by incubation at 4°C overnight. After a brief wash with PBST, the plate was blocked with 5% nonfat dry milk for 2 h at room temperature. The blood samples were diluted 10-fold with PBST, added to the plate, and incubated for 2 h at room temperature. After washing with PBST, the plate was incubated with anti-human IgG/IgM/IgA alkaline phosphatase conjugate (1:3000; Millipore) for 30 min at room temperature. Following a wash with PBST, the signal was detected by adding pNPP liquid substrate system for ELISA (Sigma). The absorbance of the reaction was measured at 405 nm using a plate reader. Negative controls consisted of wells containing carbonate-bicarbonate buffer instead of recombinant proteins and wells containing PBST instead of blood samples. Before the experiment, a series of synthetic protein concentrations was incubated with various concentrations of human serum to establish the optimal experimental conditions.
Statistical analysis
Statistical analysis of the data was performed using SPSS V.16 software (SPSS). The median differences were tested with the Mann-Whitney U test. P values < 0.05 were considered significant. When 3 groups were compared, a Kruskal-Wallis test was conducted first.
RESULTS
Screening autoantigens by 2-D WB
Following a computational analysis, about 300 spots were visualized on each 2-DE gel loaded with total protein from the synovial membranes of patients with RA. The expression patterns on the 2-DE gels were compared with the expression profiles of a parallel 2-D WB on a global level. The proteins that were immunostained with RA sera or the anticitrulline antibody were excised from the gels and identified with MALDI-TOF/TOF MS. The 2-DE gels and the WB results are shown in Figure 1. The results of the 2-DE gel and 2-D WB experiment were highly reproducible over 3 experiments. By comparing the 2-DE pattern with the corresponding WB probed with RA sera, 37 spots were selected for mass-spectrometric identification. Meanwhile, 45 spots were selected for mass-spectrometric identification by comparing the 2-DE and its corresponding WB probed with the anticitrulline antibody. Among these spots, 12 were recognized by both the RA sera and the anticitrulline antibody in the patients with RA. These protein spots were A1AT, DYH3, fibrinogen β chain (FIBB), KRT84, LUM, TUBB2A, TUBB2B, TUBB2C, TUBB3, TUBB4, TUBB5, and VIME. The result is shown in Table 2.

Two-dimensional (2-D) polyacrylamide gel electrophoresis of RA synovial proteins and parallel 2-D Western blotting. The 2-DE gels were prepared with total proteins extracted from synovial tissues of RA patients and visualized by staining (A, B). Synovial proteins were transblotted from gels to membranes and probed with sera from RA patients (C) or the anticitrulline antibody (D). Protein spots were identified by MALDI-TOF/TOF mass spectrometry.
Identification of spots immunostained with rheumatoid arthritis (RA) sera and anticitrulline in RA synovial membrane by proteome analysis.
Expression of candidate proteins in synovium of patients with RA
To verify the above 2-D WB results, WB analysis was performed with the antibodies against the aforementioned candidate proteins and GAPDH for normalization. A1AT, KRT84, and TUBB had significantly increased expression in the synovial membranes of the patients with RA compared with the patients with OA. DYH3 and LUM were not detected in any synovial samples. It is likely that the molecular weight of DYH3 is too large for transblotting onto a PVDF membrane. The result is shown in Figure 2.

Qualitative (series 1) and semiquantitative (series 2) Western blot analysis of (A) the candidate proteins α-1-antitrypsin (A1AT), (B) keratin type II cuticular Hb4 (KRT84), and (C) tubulin β-chain (TUBB) in RA and OA synovial tissues. The loaded tissue extracts were also probed with an antibody to GAPDH to normalize the loading volume.
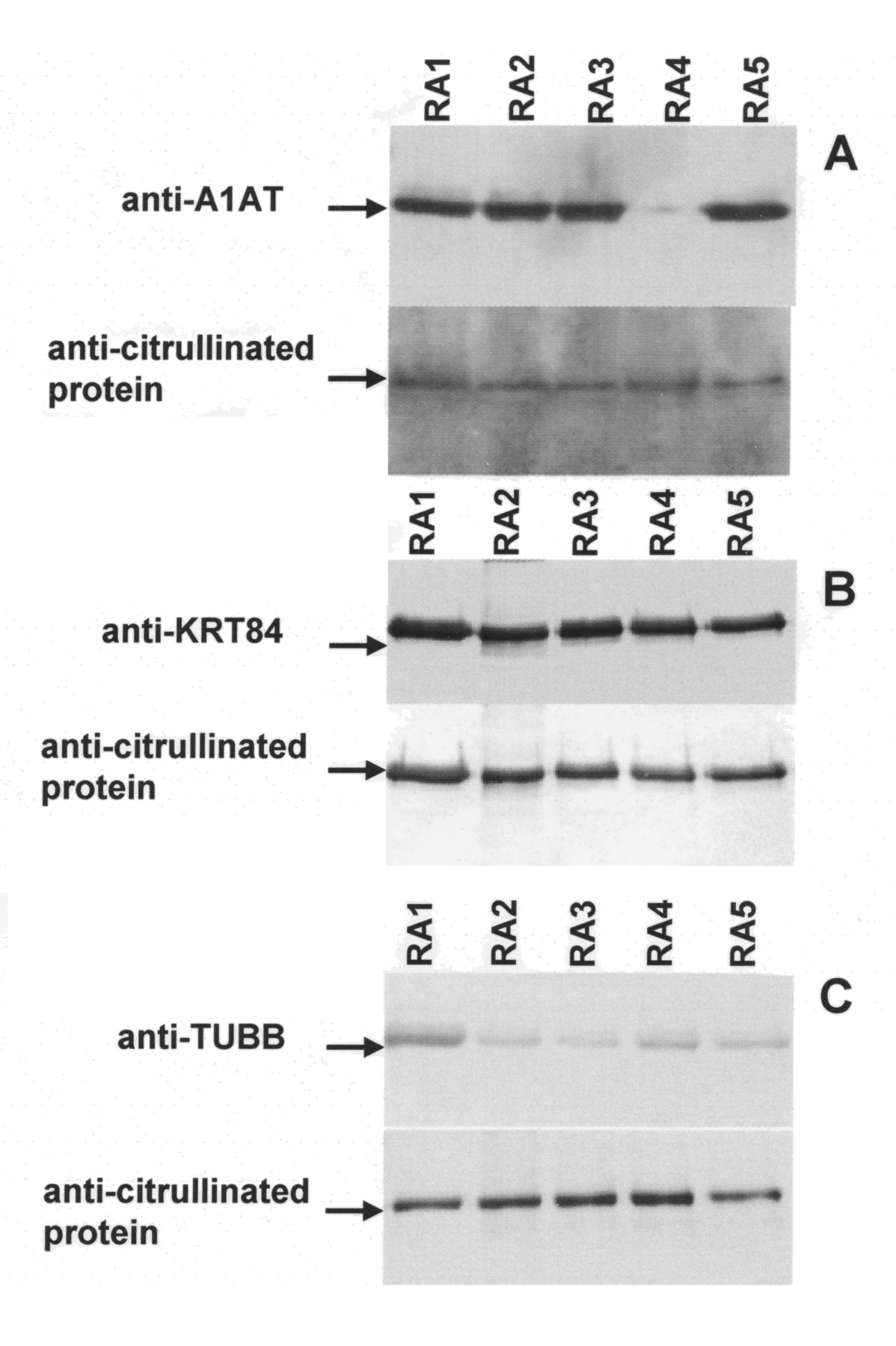
Immunoprecipitation was performed using antibodies against A1AT, KRT84, and TUBB with total protein extracts of the RA synovial tissues. WB revealed that A1AT (47 kDa), KRT84 (65 kDa), and TUBB (50 kDa) were immunoprecipitated from the total protein extracts of the patients with RA. Further, WB analysis demonstrated that A1AT, KRT84, and TUBB were recognized by the anticitrulline antibody. This result indicates that A1AT, KRT84, and TUBB were present and citrullinated in RA synovial tissues. The results of immunoprecipitation are shown in Figure 3.
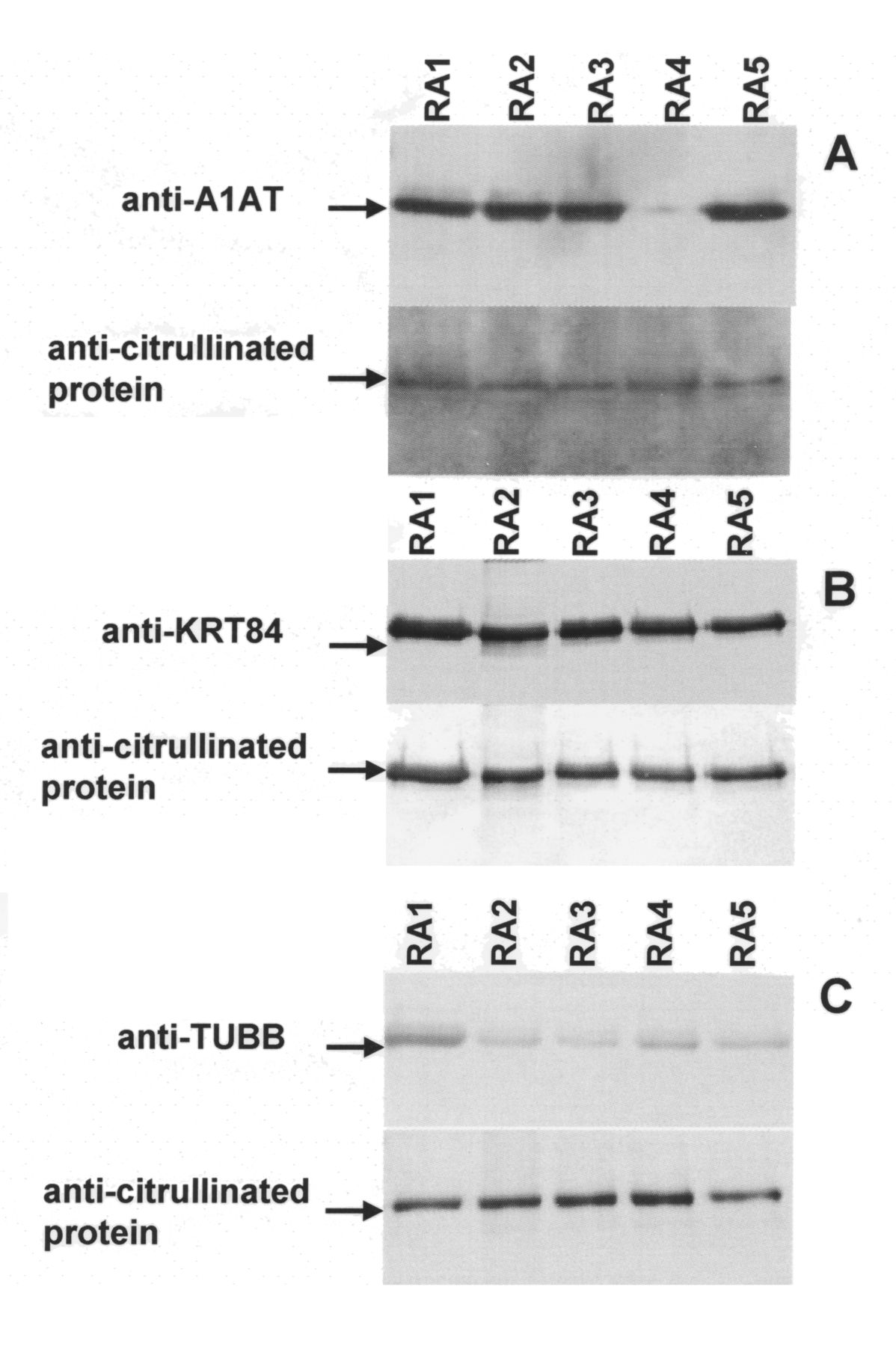
Immunoprecipitation and Western blotting of (A) α-1-antitrypsin (A1AT), (B) keratin type II cuticular Hb4 (KRT84), and (C) tubulin β-chain (TUBB) from RA synovial tissue using antibodies specific to the corresponding proteins. Anticitrullinated protein antibody was used to determine the citrullination status of the specific immunoprecipitates.
ELISA was applied to detect the expression of candidate proteins in synovial fluids. Compared with the synovial fluids of patients with OA and patients with AS, A1AT and KRT84 were significantly elevated in the synovial fluid of patients with RA, but TUBB was relatively low in the fluid of patients with RA. The tissue distribution of these proteins is shown in Figure 4.

Levels (mean ± SEM) of (A) α-1-antitrypsin (A1AT), (B) keratin type II cuticular Hb4 (KRT84), and (C) tubulin β-chain (TUBB) in synovial fluids of patients with RA (n = 40), OA (n = 30), and ankylosing spondylitis (AS; n = 33). A1AT and KRT84 levels were increased in RA fluids. Levels are represented as absorbance (OD) values at 405 nm.
Measurement of autoantibodies in the blood of patients with RA
ELISA was used to measure the levels of autoantibodies against A1AT, KRT84, and TUBB in sera from patients with RA and to compare them to those from healthy controls (Figure 5). Full-length A1AT, full-length TUBB, and the synthetic peptide against KRT84 were coated onto plates to extract the corresponding autoantibodies from the blood of the patients. Anti-KRT84 autoantibody was significantly elevated in the blood of patients with RA compared to that of the healthy controls. Compared with its average level in the healthy control samples, the anti-KRT84 autoantibody was significantly increased in over half of the blood samples from patients with RA (52/92). The average levels of anti-A1AT autoantibody and anti-TUBB autoantibody were not significantly different between patients with RA and controls. However, one-third of patients with RA had relatively high expression levels of the A1AT autoantibody and the TUBB autoantibody in their blood.

Levels (mean ± SEM) of (A) autoantibodies to α-1-antitrypsin (A1AT), (B) keratin type II cuticular Hb4 (KRT84), and (C) tubulin β-chain (TUBB) in the serum of RA patients (n = 92) and healthy controls (n = 92). Levels are represented as absorbance (OD) values at 405 nm. Anti-KRT84 levels were elevated in patients with RA.
DISCUSSION
Several groups have investigated citrullinated autoantigens in RA using a proteomic approach. Liao, et al used 2-D liquid chromatography-coupled tandem mass spectrometry to determine protein profiles of synovial fluid from patients with RA25. They found that the protein levels of CRP [S100A8 (calgranulin A), S100A9 (calgranulin B), and S100A12 (calgranulin C)] were elevated in the serum of patients with erosive RA compared to serum of patients with non-erosive RA or healthy individuals. Tabushi, et al investigated citrullinated proteins in synovial fluids derived from patients with RA using a proteomics-based analysis26. In that study, synovial fluids from patients with RA were subjected to SDS-PAGE and WB analysis to detect citrullinated proteins. The authors identified citrullinated fibrinogen, citrullinated fibronectin, and citrullinated VIME in synovial fluids from patients with RA. Kinloch, et al performed 2-D WB with synovial fluid and immunoblotted with citrullinated proteins, α-enolase, and the deiminating enzymes peptidylarginine deiminase type 2 and type 427. Citrullinated polypeptides were detected in synovial fluid from patients with RA and patients with AS, but not in OA samples. They found that α-enolase was citrullinated in RA synovial fluid. In addition, Goëb, et al analyzed HL-60 cell extract by 2-D WB using sera of untreated patients with early RA28. They identified RA antigens including heterogeneous nuclear ribonucleoprotein A2/B1, aldolase, α-enolase, calreticulin, 60 kDa heat shock protein, BiP, phosphoglycerate kinase 1, stress-induced phosphoprotein 1, and the far-upstream element-binding proteins (FUSE-BP) 1 and 2. They also showed that antigenicity of the FUSE-BP peptide was highly dependent on citrullination.
Darrah, et al identified citrullinated autoantigens by immunoblotting control and ionomycin-activated human primary neutrophil lysate with RA sera18. Autoantigen identity and citrullination sites were defined by mass spectrometry. Their study identified β- and γ-actins as novel citrullinated autoantigens in RA. Matsuo, et al were the first to examine citrullinated autoantigens by 2-D WB29. They conducted 2-D WB with a synovial tissue sample from a 53-year-old woman with RA and hybridized the transblot using pooled sera from 5 patients with RA and ACPA. The authors detected 3 fibrinogen derivatives and several novel citrullinated autoantigens, including asporin and F-actin capping protein α-1 subunit. The experimental design was similar to that of our study, but those authors performed 2-D WB with only 1 synovial tissue.
In our study, 2-D WB analyses were conducted to screen citrullinated proteins in 10 synovial tissues of patients with RA using sera from those patients and an anticitrulline antibody as a probe. Immunoreactive protein spots were identified by mass spectrometry. Both RA sera and the anticitrulline antibody by 2-D WB recognized A1AT, DYH3, FIBB, KRT84, LUM, TUBB, and VIME. WB analysis detected high levels of expression of A1AT, KRT84, and TUBB in the synovial membrane of patients with RA. ELISA detected high levels of expression of A1AT and KRT84 in the synovial fluids of patients with RA. Further, immunoprecipitation not only verified the expression of A1AT, KRT84, and TUBB in the RA synovial tissues, but it also detected the citrullination of these proteins. The result suggests that A1AT, KRT84, and TUBB are citrullinated in the synovial tissues of patients with RA, although we did not determine the citrullination sites in these candidate proteins by MALDI-TOF/TOF MS analysis. FIBB and VIME have previously been reported to be autoantigens. Using 2-D WB, we further confirmed that citrullinated fibrinogen/fibrin and VIME are candidate autoantigens for RA. The concordance of our findings with those of others also demonstrates the feasibility of our protocol and the reliability of our results.
Our study confirmed the presence of citrullinated keratin as an autoantigen in the synovium of patients with RA. KRT84, also referred to as type II hair keratin Hb4, is a basic protein that heterodimerizes with type I keratins to form hair and nails. This hair keratin is also contained primarily in the filiform tongue papilla30,31. Keratin is the main component of cellular intermediate filaments. We previously conducted immunohistochemistry using an AE1/AE3 antibody mixture that broadly recognizes various keratin forms32. In that experiment, we detected cytokeratin in many cells in the area lining the synovial membranes of patients with RA. Further, double-immunofluorescent labeling showed that the cells expressing cytokeratin were also positive for citrulline when they were in the vicinity of extracellular deposits or when they approached the exterior of the synovial membrane. WB analysis demonstrated the citrullination of keratin purified from RA synovial tissue by immunoprecipitation32. In addition, Franch, et al detected autoantibodies to intermediate filament proteins, both cytokeratin and VIME, in sera from rats with adjuvant arthritis33. These results suggest the presence of citrullinated cytokeratin in the synovial membranes of patients with RA. It can be hypothesized that the citrullination of keratin in the synovial tissues of patients with RA disrupts the tolerance of the immune system and drives the autoimmune response as an antigen. Lundberg, et al reported that the immunogenicity and arthritogenicity of citrullinated proteins could be increased by immunizing rats with citrullinated serum albumin and collagen type II34. In our study, high levels of anti-KRT84 autoantibody were detected in the blood of patients with RA compared with controls, indicating that KRT84 may stimulate an autoimmune reaction in patients with RA.
One of the main limits for our study was the selection of seropositive patients with RA for the initial screening. Because ACPA specificities are different and may coexist, ACPA-negative patients with RA should be screened to minimize the bias linked to cross-reactivity. Proteins that were detected by both RA serum and anticitrulline antibody were considered citrullinated proteins in RA in our study. In this way, we can effectively minimize the bias linked to cross-reactivity. Further, the result was verified with immunoprecipitation, routine WB, and ELISA. The second limitation for our study is that we should have performed an ELISA to analyze the reactivity of RA sera to the citrullinated versus uncitrullinated forms of the new protein targets proposed. In fact, we had conducted an ELISA to determine the reactivity of RA sera to the citrullinated versus uncitrullinated forms of KRT84. We citrullinized KRT84 recombinant protein with commercial rabbit peptidylarginine deiminase. As a result, there was no significantly increased binding activity of citrullinated KRT84 to RA sera. It is possible that citrullination of KRT84 is different from that in physiological condition. We should have located the citrullination site in the protein and then conducted ELISA to determine the binding activity of citrullinated KRT84 with RA sera. Using proteomic analyses, Ordóñez, et al revealed 9 additional citrullines in antithrombin35. They subsequently conducted ELISA using a specific monoclonal antibody against the citrullinated antithrombin. They detected an increased level of citrullinated antithrombin in the plasma of patients with RA and colorectal adenocarcinoma36. We intend to do the same type of study. Additionally, the possible role of cigarette smoking in RA has been studied37,38. We did not obtain significantly different observations between smokers and nonsmokers.
Our study identified citrullinated proteins in synovial tissues of patients with RA, including A1AT, FIBB, KRT84, TUBB, and VIME, using 2-D WB probed with RA sera and ACPA. A1AT, KRT84, and TUBB were confirmed to be highly expressed in the synovial membranes and synovial fluids of patients with RA. Further, high levels of an autoantibody against KRT84 were detected in the blood of patients with RA.
Footnotes
-
Supported by the National Natural Science Foundation of China (30972720, 81171990), the National Basic Research Program of China (2010CB529105) and the Shandong Taishan Scholarship.
- Accepted for publication November 6, 2012.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}