
Abstract
Objective. To review patients with rheumatoid arthritis (RA) receiving biologic therapy following a diagnosis of nontuberculous mycobacterial (NTM) lung disease and to evaluate disease deterioration according to clinical and radiological features and anti-NTM therapy.
Methods. We retrospectively analyzed medical records of 11 human immunodeficiency virus-negative patients with RA (median age, 64 years) receiving biologic therapy following diagnosis of NTM lung disease.
Results. NTM species included Mycobacterium avium complex in 9 patients (81.8%) and M. gordonae in 2 (18.2%). Underlying respiratory disease was present in 6 patients (54.5%), and most (81.8%) had radiographic features of nodular/bronchiectatic disease. Extent of NTM disease was 1–2 pulmonary lobes in 6 patients (54.5%), 3–4 lobes in 5 patients (45.5%), and 5–6 lobes in none. The results of radiological evaluations were unchanged or improved in 7 patients (63.6%) and worsened in 4 (36.4%). Radiological outcome was worse in patients with poor RA control despite their receiving biologic therapies for RA. Two of 3 patients receiving anti-NTM therapy as initial management for NTM improved, and 1 worsened. Three of 4 patients with worsened radiological outcome had high erythrocyte sedimentation rate (> 50 mm/h).
Conclusion. Radiological deterioration was not observed in the majority of patients with RA receiving biologic therapy with NTM lung disease, and radiological outcome of pulmonary NTM was favorable in some patients undergoing anti-NTM therapy. Further studies focusing on disease deterioration according to biologic therapy received during NTM followup are warranted to determine appropriate treatment of RA patients with NTM lung disease.
- RHEUMATOID ARTHRITIS
- NONTUBERCULOUS MYCOBACTERIAL LUNG DISEASE
- BIOLOGIC THERAPY
- RADIOLOGICAL DETERIORATION
- DRUG TOXICITY
A high frequency of infections complicating patients with rheumatoid arthritis (RA) has been reported in comparison with patients without RA1. This was presumed to be the result of the immunomodulatory effects of RA or agents with immunosuppressive effects used in its treatment1. Tuberculosis and nontuberculous mycobacterial (NTM) infections in association with concurrent administration of biologic therapies have been reported2,3. Further, in regions with low prevalence of tuberculosis, NTM infections may be an important complication of anti-tumor necrosis factor (anti-TNF) therapy as the biologic agent2. Contrary to that of tuberculosis, NTM incidence is increasing within the United States and Europe, particularly among older women4. Winthrop, et al2 reported that the incidence rate of NTM among patients with RA undergoing anti-TNF therapy was more than 5-fold higher vs RA patients not exposed to anti-TNF therapy. Further, 39% of patients in the group administered anti-TNF therapy after NTM diagnosis died2. Unlike the process in tuberculosis infection, there is no evidence of a latent phase in NTM infection. Therefore, screening and preventive treatments against NTM infection in patients scheduled to begin anti-TNF therapy might not be feasible5. Thus, the timely diagnosis of pulmonary NTM disease is critical during biologic therapy for RA.
We previously classified antirheumatic drugs during NTM lung disease followup along with the risk of combination therapy, e.g., TNF antagonists/tocilizumab, methotrexate (MTX), and corticosteroid, but their contribution to radiological deterioration was not assessed6. The most important point is the relation between NTM lung disease and these biologic agents. Because it is difficult to conduct a prospective study of biologic therapy for RA patients with NTM lung disease, there is a paucity of available reports, so our study should be valuable. Our aims were to retrospectively review patients with RA receiving biologic therapies following diagnosis of NTM lung disease and to evaluate disease deterioration according to clinical and radiological features and anti-NTM therapy received. This investigation was clinically relevant and important to determine appropriate treatment of RA patients with NTM lung disease.
MATERIALS AND METHODS
Patients
We studied 11 patients with RA over 18 years of age who received biologic therapies following diagnosis of NTM lung disease, fulfilled 2007 American Thoracic Society/Infectious Disease Society of America (ATS/IDSA) NTM diagnostic criteria7, and were newly diagnosed from 1993 through July 2012. NTM lung disease diagnosis and therapy were conducted at the Saitama Cardiovascular and Respiratory Center, Saitama, Japan. All patients fulfilled revised criteria for RA of the American Rheumatism Association8. RA diagnosis and therapy were conducted by rheumatologists at other institutions.
Study design
This was a retrospective study for which clinical data were collected from medical records. Baseline clinical characteristics were obtained within 1 month of initial NTM diagnosis. Radiographic abnormalities of NTM lung disease were classified according to the following 4 disease patterns seen on chest high-resolution computed tomography (HRCT): nodular/bronchiectatic (NB), fibrocavitary (FC), FC+NB, and unclassifiable9. No patient had an unclassifiable pattern. Underlying respiratory diseases were classified as usual interstitial pneumonia (UIP), emphysema, previous pulmonary tuberculosis, and bronchiolitis. No patients had ≥ 2 underlying respiratory diseases. Because bronchiectasis and NTM often coexist, making causality difficult to determine10, bronchiectasis was not counted as an underlying respiratory disease9. If drug administration for NTM lung disease was initiated within 6 months after diagnosis and continued for > 3 months, we considered this as initial management9. If no treatment was initiated within 6 months after diagnosis, we considered initial management to be observation. Patients were followed through March 2013.
Evaluation of chest HRCT findings
If the antirheumatic drug was not changed during the observational periods and HRCT was performed each year, assessment of radiologic change was independently performed by 2 radiologists and classified as improvement, no change, or deterioration. To quantify observer variation, κ coefficients of agreement were calculated for assessment of radiologic changes. The important problem was how to differentiate NTM lung disease from normal colonization with regard to sputum culture results in the patients with RA. We first searched the database of NTM cultures of our hospital and selected patients with RA. Then, we removed the patients with normal chest CT findings. If patients had only bronchiectasis without centrilobular nodules of different sizes or cavities, we considered this to be colonization. Time to radiologic deterioration was evaluated for the period from the date of the first HRCT to the date when deterioration was first observed.
Data analysis
Categorical baseline characteristics are summarized by frequency and percentage, and characteristics are reported as median (range). We compared baseline characteristics for each NTM species, each radiographic feature, each underlying respiratory disease, each antirheumatic drug for radiological evaluation, anti-NTM therapy, and antirheumatic drugs during the NTM followup period. We collected demographic characteristics, body mass index (BMI; we used the current World Health Organization BMI cutoff value for underweight of < 18.5 kg/m2), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), anti-cyclic citrullinated peptide (anti-CCP) antibody, rheumatoid factor (RF), IgG, NTM species, radiographic features, underlying respiratory disease, and RA data including disease duration, disease activity, and antirheumatic drugs used at NTM diagnosis and post-NTM diagnosis. We also evaluated radiological outcome for antirheumatic drugs and anti-NTM therapy. Our study was approved by the institutional review board of the Saitama Cardiovascular and Respiratory Center (2012047).
RESULTS
Characteristics of patients with RA receiving biologic therapies after diagnosis of pulmonary NTM
Of the 11 patients, 8 (72.7%) were women, and 4 (36.4%) had a history of smoking. No patients were infected with human immunodeficiency virus (HIV). NTM species included Mycobacterium avium complex (MAC) in 9 patients (81.8%) and M. gordonae in 2 (18.2%). Median patient age was 64 years (range: 44–82 yrs). Median BMI was 20.2 kg/m2 (range: 14.1–29.0 kg/m2). Underlying respiratory disease was present in 6 patients (54.5%): 3 patients had bronchiolitis, 1 had emphysema, 1 had UIP, and 1 had previous pulmonary tuberculosis. Radiographic features on HRCT included NB disease in 9 patients (81.8%), FC disease in 1 (9.1%), and FC+NB disease in 1 (9.1%). Extent of NTM disease was 1–2 pulmonary lobes in 6 patients (54.5%), 3–4 lobes in 5 patients (45.5%), and 5–6 lobes in none. Median serum level of lymphocytes was 1300/μl (range: 500–3300/μl), albumin was 3.8 g/dl (range: 3.2–4.1 g/dl), ESR was 28 mm/h (range 5–93 mm/h), CRP was 0.74 mg/dl (range: 0.02–3.21 mg/dl), and IgG was 1725 mg/dl (range: 1115–2967 mg/dl). Ten patients (90.9%) were positive for serum RF, 7 (63.6%) were positive for anti-CCP antibody, and status was unknown in 3 patients. No patient had other concomitant collagen diseases such as Sjögren syndrome, systemic sclerosis, or dermatomyositis/polymyositis.
Microbiological examination of patients diagnosed as having pulmonary NTM
Culture results from at least 2 separate expectorated sputum samples were positive in 8 patients, and culture results from at least 1 bronchial wash or lavage were positive in 3 patients (Cases 3, 6, and 7). Only 1 patient (Case 8) had a specimen that was positive for acid-fast bacilli smears at NTM diagnosis; acid-fast bacilli were cultured later in the other patients.
Biologic therapies administered during pulmonary NTM followup
Median duration of RA was 15 years (range 2 months–24 years). Biologic agents were administered as an antirheumatic therapy for RA at NTM diagnosis in 4 patients (36.4%). Biologic therapies administered during pulmonary NTM followup included etanercept (ETN) in 8 patients (72.7%), tocilizumab (TCZ) in 2 patients (18.2%), and infliximab (IFX) in 1 patient (9.1%). In the 3 patients receiving anti-NTM therapy as the initial management for NTM, 2 patients improved [Cases 6, 7 (Case 7; Figure 1)] and 1 patient worsened (Case 11; Table 1). There was a tendency for ESR to be high (> 50 mm/h) in 3 of the 4 patients with worsened radiological outcome (Cases 9–11; Table 2).
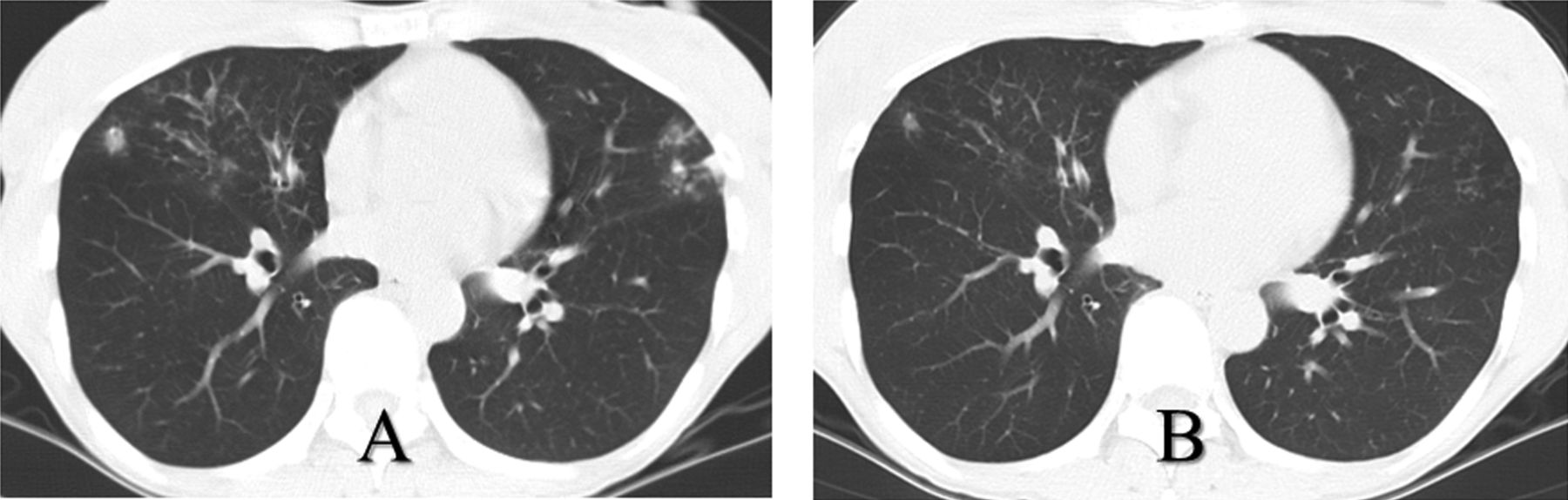
Chest computed tomography of Case 7 at diagnosis of pulmonary nontuberculous mycobacteriosis (NTM) showed patchy infiltrations in the right middle lobe and the left lingular segment lobe (A). After receiving 6 months of anti-NTM therapy with etanercept, infiltrations improved (B).
Treatment regimens and radiologic outcome for rheumatoid arthritis (RA) and pulmonary nontuberculous mycobacteriosis (NTM) diseases.
Characteristics and radiologic outcome of pulmonary nontuberculous mycobacteriosis (NTM) disease patients receiving biological therapies.
Of the 11 patients receiving biologic therapies, 4 began taking those drugs after confirmed negative study of 3 sputum specimens for acid-fast bacilli smears, but nontuberculous mycobacteria were cultured after starting biologic therapy (Cases 1–3, 9), and 2 patients with these same results in microbiological studies were continued on biologic therapy already in progress (Cases 5, 10). Biologic therapy was continued in these 6 patients, including the 2 patients with insufficient RA control (Cases 9, 10). The other 5 patients were diagnosed as having NTM lung disease at the start of biologic therapy, which was administered after we received informed consent from these patients because control of their RA was poor (Cases 4, 6–8, and 11).
Radiological outcome was unchanged or improved in 7 patients (63.6%) and worsened in 4 patients (36.4%). The patients with poor control of RA tended to have worsened radiological outcome despite receiving biologic therapies for RA (Cases 9–11). Interobserver agreement on radiologic changes was good (κ = 0.816, 95% CI 0.578–1.055).
Treatments and outcomes of patients with worsened pulmonary NTM disease during biologic therapy for RA
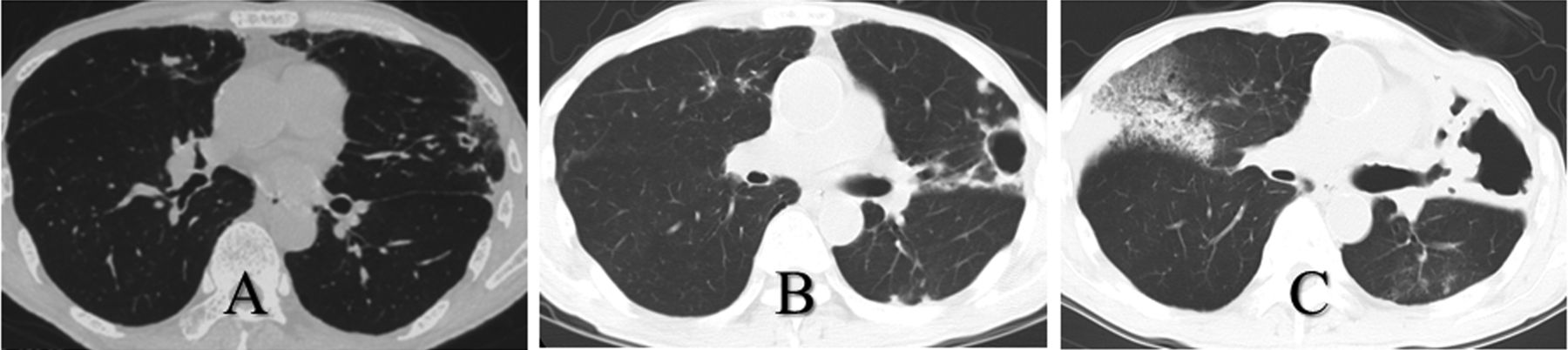
With the exception of 1 patient (Case 10), 3 of 4 patients stopped biologic therapy when pulmonary NTM disease worsened (Table 3). In Case 9, ETN was stopped for 5 months, antirheumatic drug was changed to MTX without anti-NTM therapy, and no radiological deterioration occurred for 16 months. One patient received anti-NTM therapy and stopped ETN, which resulted in improved radiological outcome for 1 month (Case 8). The remaining patient received TCZ with anti-NTM therapy (clarithromycin, ethambutol, and rifampicin) as initial management, but worsened. Therefore, TCZ was then discontinued, and anti-NTM therapy was reinforced with streptomycin. However, radiological outcome worsened, and this patient was complicated by chronic pulmonary aspergillosis (Case 11; Figure 2). He died 10 months later with a final diagnosis of chronic pulmonary aspergillosis. In Case 10, biologic therapy was changed from IFX to ETN without anti-NTM therapy, and no radiological deterioration occurred for 19 months while receiving ETN. Afterward, control of RA was poor, ETN was changed to TCZ, and the patient’s condition worsened for 5 months (Figure 3).

Chest computed tomography of Case 11 at diagnosis of pulmonary nontuberculous mycobacteriosis (NTM) showed a small cavity and infiltrations in the left lingular segment lobe and opacity in the right middle lobe (A). After 6 months of tocilizumab (TCZ) and anti-NTM therapy, the cavity shadows had extended (B). After 4 months of reinforced anti-NTM therapy and discontinuation of TCZ, the radiological outcome worsened and was complicated by chronic pulmonary aspergillosis (C).
{kind=link}
{kind=link}
{kind=link}
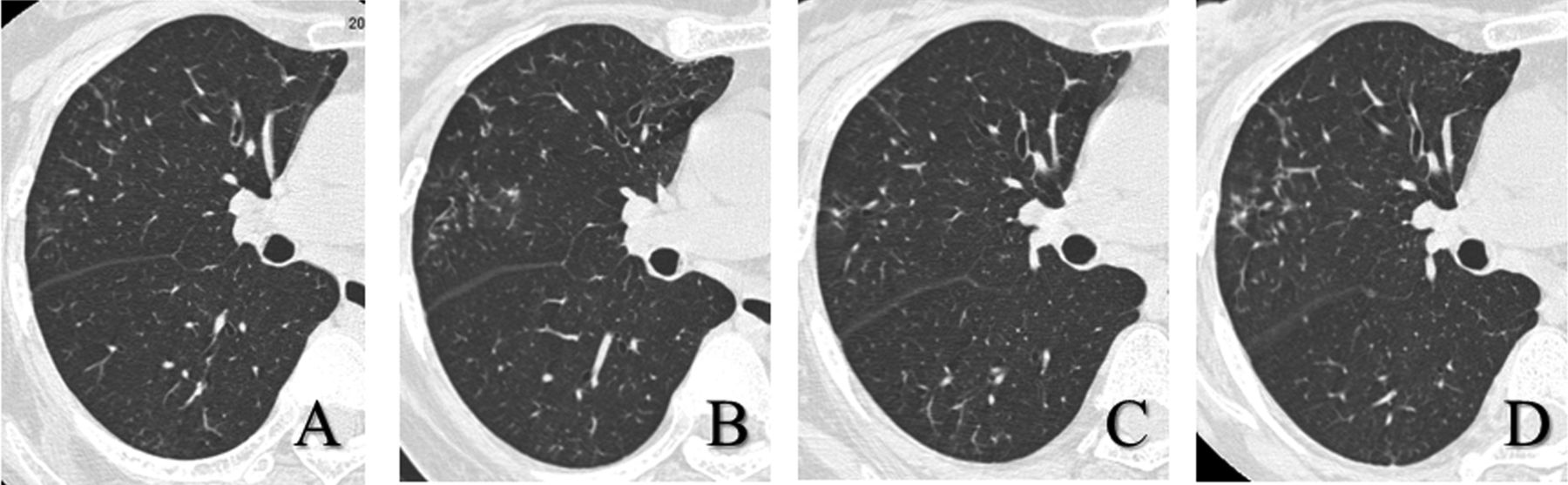
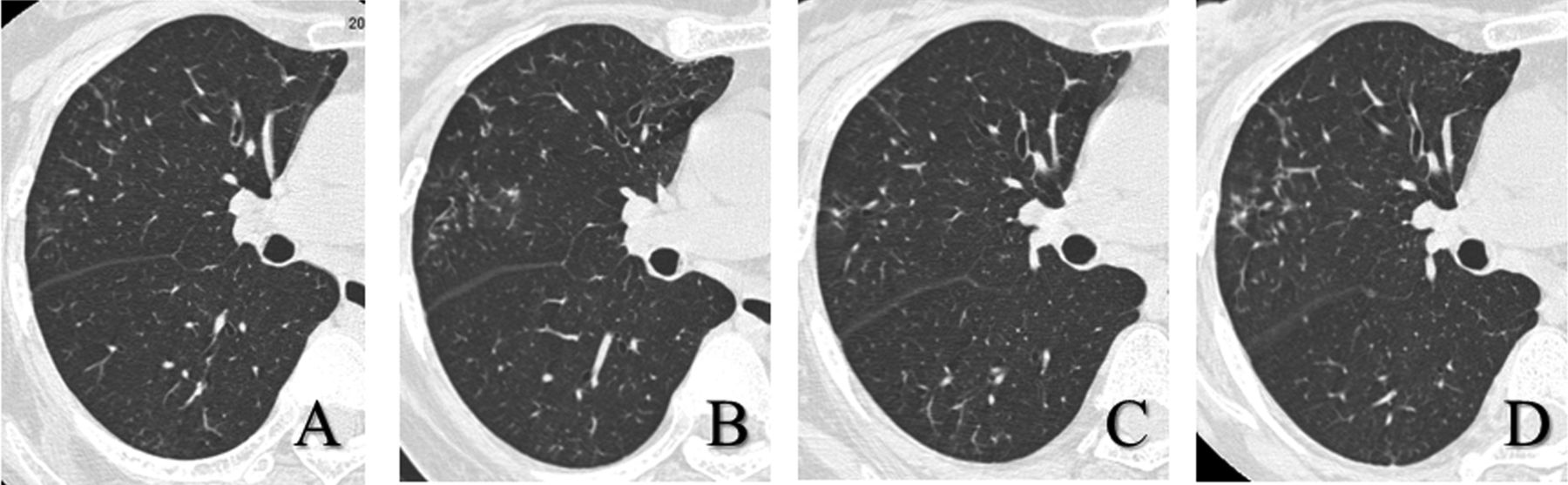
Chest computed tomography of Case 10 at diagnosis of pulmonary nontuberculous mycobacteriosis (NTM) showed centrilobular small nodules in the right middle lobe (A). After 2 months of infliximab (IFX), the small nodule shadows had extended slightly (B). After 19 months of etanercept therapy following discontinuation of IFX, there was no radiological deterioration (C). After 5 months of tocilizumab therapy following discontinuation of the etanercept, the small nodule shadows had worsened slightly (D).
Treatment regimens for rheumatoid arthritis (RA) and pulmonary nontuberculous mycobacteriosis (NTM) diseases postradiological deterioration.
DISCUSSION
We investigated patients with RA receiving biologic therapy following a diagnosis of NTM lung disease, and evaluated disease deterioration according to clinical and radiological features and anti-NTM therapy. In the 11 patients studied, NTM species included MAC in 9 patients (81.8%) and M. gordonae in 2 (18.2%). The results of radiological evaluations were unchanged or improved in 7 patients (63.6%) and worsened in 4 patients (36.4%). The patients with poor control of RA despite receiving biologic therapies for RA tended to have worsening of radiological outcome. Of the 3 patients receiving anti-NTM therapy as initial management for NTM, 2 patients improved, but 1 patient worsened. Of the 4 patients with worsening of radiological outcome, ESR was high in 3 patients.
RA is known to be associated with an increased risk of infectious diseases. In the later decades of the last century, controlled observational studies found that age-adjusted mortality in patients with RA increased by about 2-fold compared with the general population, and infectious diseases were 1 of the 3 leading causes of premature death in RA cohorts in the United States and Europe11,12,13,14. Listing, et al reported that chronic comorbidity, smoking, active RA, high-dose corticosteroid, and TNF inhibitor are associated with an increased risk of infection15, and the most common events are respiratory infections15,16. Takayanagi, et al reviewed 149 Japanese cases of pulmonary infections in patients with RA and found that NTM disease was the most frequent pulmonary infection, accounting for 40% of cases17.
We previously reported that 98 HIV-negative patients with RA who had NTM lung disease had overall cumulative 5- and 10-year mortality rates of 33.9% and 52.6%, respectively. MAC was the most frequent pathogen (83.7%), followed by M. kansasii (6.1%), M. gordonae (6.1%), and others (4.1%). Antirheumatic drugs received at NTM diagnosis included MTX in 31.6% of patients, of whom 12.2% concomitantly received corticosteroid, corticosteroid without MTX in 27.6% of patients, and biologic agents only in 6.1% of patients6.
The risk of serious infections in RA corresponds to an OR of about 1.2–1.4 in TNF antagonist-treated patients18,19. Similar OR were found for abatacept (1.4) and TCZ (1.3)20,21. The ATS/IDSA guidelines for NTM diseases state that patients with active NTM disease should receive TNF-α blocking agents only if they are also receiving adequate therapy for the NTM disease7. In addition, the Japanese guidelines for use of infliximab and etanercept in RA recommend that TNF antagonists be avoided in patients with a history of NTM infection22. Some cases of fatal NTM lung disease occurring during biologic therapy for RA were reported, which included NTM species of M. abscessus in 2 cases and M. xenopi and M. peregrinum in 1 case each23,24,25,26. Therefore, most rheumatologists avoid the use of biologic therapies in RA patients with NTM with a poor prognosis such as cavity type or with wide extent of pulmonary disease, the presence of concomitant serious pulmonary disease, or rapid worsening of disease. Thus, is biologic therapy absolutely contraindicated in RA patients with NTM lung disease?
In our present study of biologic therapies administered during pulmonary NTM followup, 5 patients (45.5%) experienced no radiological deterioration despite receiving no anti-NTM therapy. Moreover, radiologic findings improved in 3 patients, 2 of whom received anti-NTM therapy as initial management (Cases 6, 7). In fact, Mori, et al reported favorable therapeutic outcomes of NTM lung diseases in patients with a history of NTM infection; NTM species included MAC (92.3%) and M. abscessus (7.7%)27. However, 1 of our patients worsened severely despite stopping biologic therapy and receiving anti-NTM therapy (Case 11). The 11 patients in the present study tended to have a mild form of NTM lung disease such as that with NB-type radiologic features (81.8%) and negative acid-fast bacilli smears from respiratory specimens (90.9%). Further studies are needed to assess the safety of biologic agents used in moderate to severe forms of NTM lung disease.
We also previously reported that ESR > 50 mm/h was a negative prognostic factor for radiological deterioration of NTM lung disease in patients with RA6. In our present study, the ESR was > 50 mm/h in 3 of the 4 patients with worsened radiological outcome (Cases 9–11). Control of RA in these patients was poor despite biologic therapies. Therefore, the cause of the high ESR was considered to be due not only to NTM activity but also to RA activity. High RA disease activity leads to an increased risk of serious infection in RA patients28. From this point of view, in reality, some RA patients with NTM lung disease in whom RA activity is difficult to control will require biologic therapy clinically. In regard to biologic agents, the use of IFX or adalimumab rather than ETN is a strong and significant predictor of infection29,30. In our present study, for the observational period that was not limited only to the period that the biologic therapy was administered, 2 (22.2%) of 9 patients receiving ETN worsened. However, 1 patient receiving IFX worsened (Case 10), as did 2 of 3 patients receiving tocilizumab (Cases 4, 11). In Case 10, there was no radiological deterioration for 19 months with ETN, whereas deterioration occurred for 2 months with IFX and for 5 months with TCZ. Therefore, the relation between each biologic agent and pulmonary NTM deterioration must be elucidated.
No radiological deterioration occurred in some RA patients with NTM lung disease receiving biologic therapy. Although the radiological outcome of pulmonary NTM treated with anti-NTM therapy was favorable in some patients, it worsened in others despite administration of anti-NTM therapy. It is important to stress both that potent drugs available to control NTM infection are scarce and that suppression of host immunity with biologic therapy for RA may be catastrophic for the patient. Therefore, further studies focusing on disease deterioration according to biologic therapy received during NTM followup are warranted and will be necessary for determining appropriate treatment of RA patients with NTM lung disease.
Acknowledgment
We offer our sincerest thanks to Drs. Naho Kagiyama, Kazuyoshi Kurashima, Tsutomu Yanagisawa, and Yotaro Takaku of the Department of Respiratory Medicine, Saitama Cardiovascular and Respiratory Center.
- Accepted for publication August 16, 2013.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.