
Ocular involvement in rheumatoid arthritis (RA) can arise independently of articular and extraarticular disease1. RA is the most common underlying condition associated with destructive corneal disease2,3. Peripheral ulcerative keratitis (PUK) develops in the form of crescent-shaped stromal inflammation on the limbal edge of the cornea, characterized by local thinning of the affected area. PUK is typically a disease of long-standing seropositive, erosive RA, which may have serious ocular complications4. Symptoms and signs include ocular redness, pain, tearing, photophobia, and decreased vision secondary to induced astigmatism or corneal opacity in advanced cases. Urgent ophthalmic referral is recommended if the patient describes these symptoms. Biomicroscopic examination may show corneal opacity due to cellular infiltrates within the stroma adjacent to the limbus. Later, crescent-shaped corneal ulcers develop with breakdown of the overlying epithelium.
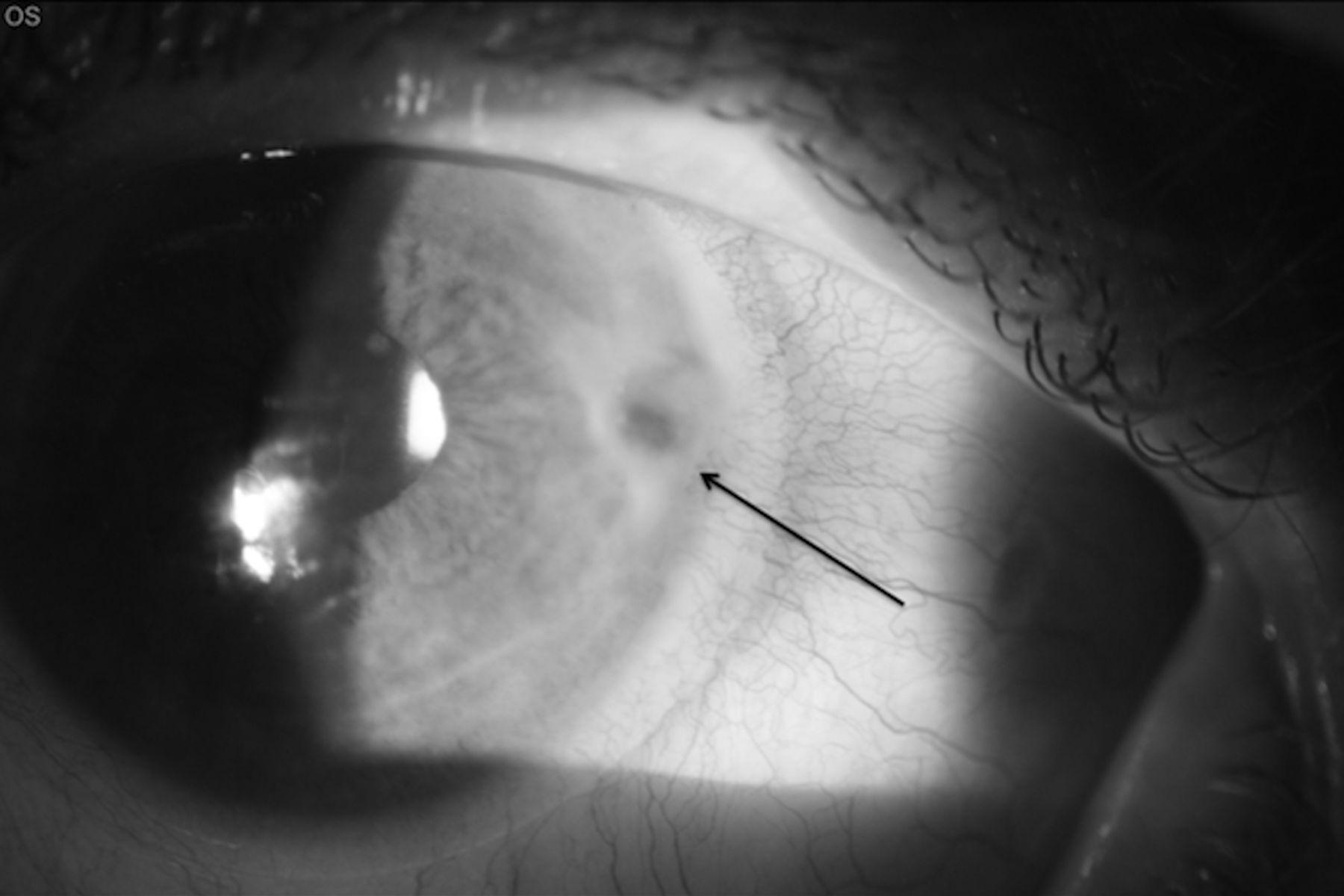
A 51-year-old woman with seropositive RA presented with recurrence of PUK. A new crescent-shaped corneal ulcer running parallel to the limbus, with breakdown of the overlying epithelium, was noted. There was dramatic corneal thinning and imminent risk of corneal perforation (Figure 1).

A 51-year-old woman with seropositive RA. Recurrence of PUK with a new crescent-shaped corneal ulcer running parallel to the limbus (arrow) and breakdown of the overlying epithelium. There is dramatic corneal thinning and imminent risk of corneal perforation.
With PUK, varying degrees of vascularization and corneal thinning due to tissue loss in the underlying stroma can occur. The marginal furrow may progress by circumferential or central extension rather than local ulceration5. The depth of peripheral corneal thinning is variable. In severe cases, tissue loss may progress to perforation, with or without trauma.
An 84-year-old woman with seropositive RA presented with spontaneous corneal perforation in a localized peripheral ulcer in the left eye. There was adjacent conjunctival inflammation. A therapeutic contact lens is in place. Surgical repair was required (Figure 2).

{kind=link}
{kind=link}
Spontaneous corneal perforation (arrow) in a localized peripheral ulcer in the left eye of an 84-year-old woman with seropositive RA. There is adjacent conjunctival inflammation. A therapeutic contact lens is in place prior to surgical repair.
Adjacent conjunctival, episcleral, and scleral inflammation are usually apparent with corneal thinning due to tissue loss. A small subset of patients with long-standing RA develop severe corneal and/or necrotizing scleral inflammation, indicative of a vasculitic stage of the underlying disease2,4. PUK associated RA should be treated with vigorous immunosuppressive treatment. Collaboration between rheumatologists and ophthalmologists is also necessary for adequate treatment of eye disease.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.