

Abstract
Objective. The quality of glucocorticoid-induced osteoporosis (GIOP) care [defined by bone mineral density (BMD) testing or osteoporosis treatment] is suboptimal and has been targeted for improvement. The assumption that improvements in GIOP preventive care will lead to better outcomes has not been tested.
Methods. We used linked healthcare databases to conduct a population-based study of all adults 20 years of age or older in Manitoba, Canada, who initiated longterm (> 90 days) systemic glucocorticoids (GC) between 1998 and 2008. High-quality GIOP care was defined by BMD testing or prescription osteoporosis treatment within 6 months. Outcomes were adjusted odds of major fractures within 1 year and 3 years.
Results. We studied 15,285 subjects who had just begun to take GC; 5804 (38%) were 70 years of age or older, 9185 (58%) were women, and 4755 (30%) received 10 mg or more prednisone equivalents daily. Overall, 3898 (25%) subjects received a BMD test or osteoporosis treatment within 6 months. Within 1 year of starting GC, there had been 206 major fractures (1%) and within 3 years, 553 major fractures (4%). High-quality GIOP preventive care was not associated with a reduced risk of major fractures within 1 year (adjusted OR 1.6, 95% CI 1.2–2.1) or within 3 years (adjusted OR 1.3, 95% CI 1.1–1.6).
Conclusion. Three-quarters of those initiating GC received suboptimal osteoporosis care. Conventional administrative database analyses could not demonstrate that better GIOP preventive care was associated with reductions in medically attended fractures. Clinically rich databases and different analytic techniques are needed to better evaluate the effectiveness of GIOP preventive care.
Glucocorticoid-induced osteoporosis (GIOP) is the most common cause of secondary osteoporosis, and up to 1% of all adults are exposed to longterm systemic glucocorticoids (GC) each year1,2. GIOP occurs rapidly, with dose-related increases in fracture rates occurring within 3–6 months and with a particular predilection for vertebral sites2,3,4. Experts and guidelines suggest bone mineral density (BMD) testing and prophylactic osteoporosis treatment in most patients newly initiating a course of 5–10 mg prednisone daily for 3 months or longer1,2,3,4. Despite this guidance, the quality of GIOP-related preventive care has not improved markedly over the last decade and it remains far from optimal1,5,6. For example, in a Canadian study of almost 18,000 subjects followed from 1998 to 2008, we reported rates of BMD testing or osteoporosis treatment after GC initiation of 25%1, and even multifaceted interventions directed at improving GIOP care have achieved rates on the order of only 40%–50%5,6.
Because of the continuing poor quality of care, GIOP-related preventive care has been targeted for performance measurement and quality improvement5,6,7,8. As in many other settings, easily measured quality metrics first need to be defined7,8,9,10,11,12. For GIOP, this has previously been defined as “receipt of BMD test or prescription osteoporosis treatment” after new GC initiation5,6,7,8. For such a quality metric reflecting the performance of a process-of-care measure to be considered valid, it ought to be evidence-based, and improvements in quality should be tightly linked with clinically important endpoints such as mortality, rehospitalizations, or fracture9,10,11,12,13. Research has supported the hypothesis that improvements in several different performance measures have led to improvements in morbidity and mortality in several disease settings, validating these measures for use in quality improvement or pay-for-performance settings10,11. But this improvement is not always the case; for example, in pneumonia, improvements in the performance of the quality measure of “diagnosis and treatment within 4 hours of presentation” led to increases in misdiagnosis and inappropriate antibiotic use12. Thus, it is imperative that performance measures that are targeted for quality improvement and pay-for-performance schemes are indeed associated with better outcomes of care9,10,11,12,13. Therefore, we conducted a population-based study to test the hypothesis that better quality of GIOP-related preventive care would be associated with better outcomes, i.e., lower rates of incident fracture over 1 year and 3 years.
MATERIALS AND METHODS
Study design
Our goal was to mimic the data collection that would be part of a large healthcare organization’s standard approach to using accredited performance measures to determine the quality of osteoporosis care delivered to patients newly initiating systemic GC. Thus, we undertook a population-based cohort study of all adults 20 years of age and older in Manitoba, Canada, who began longterm systemic GC between 1998 and 2008 and followed them for at least 3 years, as described1. We excluded those living in nursing homes and related institutions because of incomplete prescription data, and those who did not have continuous healthcare coverage for the duration of the study. Manitoba has a population of 1.3 million with universal healthcare coverage that includes comprehensive services regardless of age or income.
The Health Research Ethics Board of the University of Manitoba approved the study and Manitoba Health Information Privacy Committee approved data access.
Data sources
The main data source for our study was the Manitoba Population Health Research Data Repository14,15. This is a comprehensive collection of continuously updated and longitudinal anonymized health services datasets housed at the Manitoba Centre for Health Policy14,15. Data in the repository include sociodemographic characteristics, vital statistics, physician claims, hospital discharges, and prescription drug dispensations. These data are well validated and have been used extensively in previous research1,16,17. A deidentified unique personal health information number permits linkage to clinical registries such as the Manitoba Bone Density Program Database16. All clinical dual-energy x-ray absorptiometry (DEXA) tests conducted in Manitoba are performed within this single program and the registry has been described and validated16.
New prescription of longterm systemic GC
For these analyses we were interested only in new users, and so any subject who had been dispensed oral systemic GC in the previous year was excluded. By convention, 90 days or more of GC therapy was considered longterm treatment, and subjects with shorter courses of treatment were excluded. We converted all systemic GC dispensations to daily prednisone equivalents (e.g., 20 mg hydrocortisone = 5 mg prednisone) and then averaged this over the course of therapy to obtain average daily dose in prednisone equivalents1. We then categorized the daily dose dispensed as low (< 5 mg prednisone daily), medium (5–10 mg daily), or high (> 10 mg daily).
High-quality GIOP preventive care
The independent variable of interest was the quality metric or performance measure of high-quality GIOP preventive care. This was set as the composite endpoint of a BMD test or a dispensation for prescription osteoporosis medications within 6 months of a new longterm systemic GC initiation1,5,6,7,8. Osteoporosis medications considered appropriate for GIOP prevention included the bisphosphonates, calcitonin, raloxifene, and teriparatide but not estrogen or other hormone therapies2,3,4.
Major osteoporotic fractures
The outcome of interest was incident major osteoporotic fracture as defined under the World Health Organization formulation (any nontraumatic fragility fracture of the forearm, humerus, clinically diagnosed vertebrae, or hip) occurring within 1 year and 3 years. We used previously validated case definitions of osteoporosis-related fractures based on diagnostic codes given in physician claims and hospital discharges16,17. In addition, we required that hip and forearm fractures be accompanied by site-specific fracture reduction, fixation, or casting codes to enhance diagnostic and temporal specificity for acute fracture. As a sensitivity analysis, we examined incident hip fracture within 3 years as the outcome of interest.
Other measurements and potential confounders
We considered sociodemographic characteristics including age in 10-year bands, sex, and location of residence (urban vs rural). We defined burden of comorbidity using the Johns Hopkins ACG® Case-Mix System (version 9)18. The number of aggregated diagnosis groups (ADG) was analyzed as follows: 0–2 ADG (reference) vs 3–5 ADG vs > 5 ADG. While we could record the burden of comorbidity in this fashion, we could not determine the specific indications for GC therapy. As proxies for “frailty” not recorded by these comorbidities, we considered 2 measures: first, all-cause hospitalization in the 1 year prior to GC initiation (0 as reference vs 1 vs > 1 hospitalization), and second, any use of home healthcare visits in the 1 year prior to initiation (0 as reference vs 1 or more visits). Lastly, GC exposure was characterized by remote exposure (i.e., any prolonged episode of GC use of 90 days or longer more than 1 year prior to study entry vs not) and dose (i.e., high dose as 10 mg per day or more prednisone equivalent vs lower doses).
Statistical analysis
We computed descriptive statistics and tabulated data according to the presence or absence of high-quality GIOP preventive care defined as BMD test or prescription of osteoporosis medication. We adjusted all subsequent analyses for age, sex, residence, comorbidities, proxies for frailty, and remote prior GC exposure and current doses dispensed. We did not adjust for persistence or adherence with osteoporosis treatment itself, other than its inclusion in our composite performance measure of high-quality GIOP preventive care. We used multivariable logistic regression analyses and calculated adjusted OR with 95% CI for major osteoporotic fractures within 1 year and 3 years. As suggested by Schneeweiss and colleagues, in administrative database analyses that do not have clinical information and do not have information on many potential confounders, careful restriction analyses may yield less biased estimates of effect and better control confounding by indication or treatment bias19. Thus, we undertook a restriction sensitivity analysis and created a far more homogenous subgroup of subjects who were at uniformly much higher predicted risk of fracture. Specifically, we restricted analyses to those who were 60 years of age or older, who were women, who had 3 or more comorbidities, and who used high-dose GC. In this restricted subgroup [n = 1194 (8%) of the parent cohort of n = 15,825], we repeated all analyses. In theory, because this restricted subgroup is at so much higher risk of fracture and is so much more alike than the overall population, issues related to confounding by indication or treatment bias should be substantially reduced if not nearly eliminated19. All analyses were conducted using SAS (version 9.2; SAS Institute).
RESULTS
From 1998 to 2008, there were 15,285 subjects who began longterm systemic GC and entered our cohort. The mean age of the study cohort was 60 years (SD 18), 38% were 70 years of age or older, 58% were women, and 66% resided in urban regions. One-third (n = 4755) of subjects newly initiated high-dose GC and 851 (6%) subjects had had a remote exposure to GC (more than 1 year prior to study entry).
Receipt of high-quality GIOP preventive care
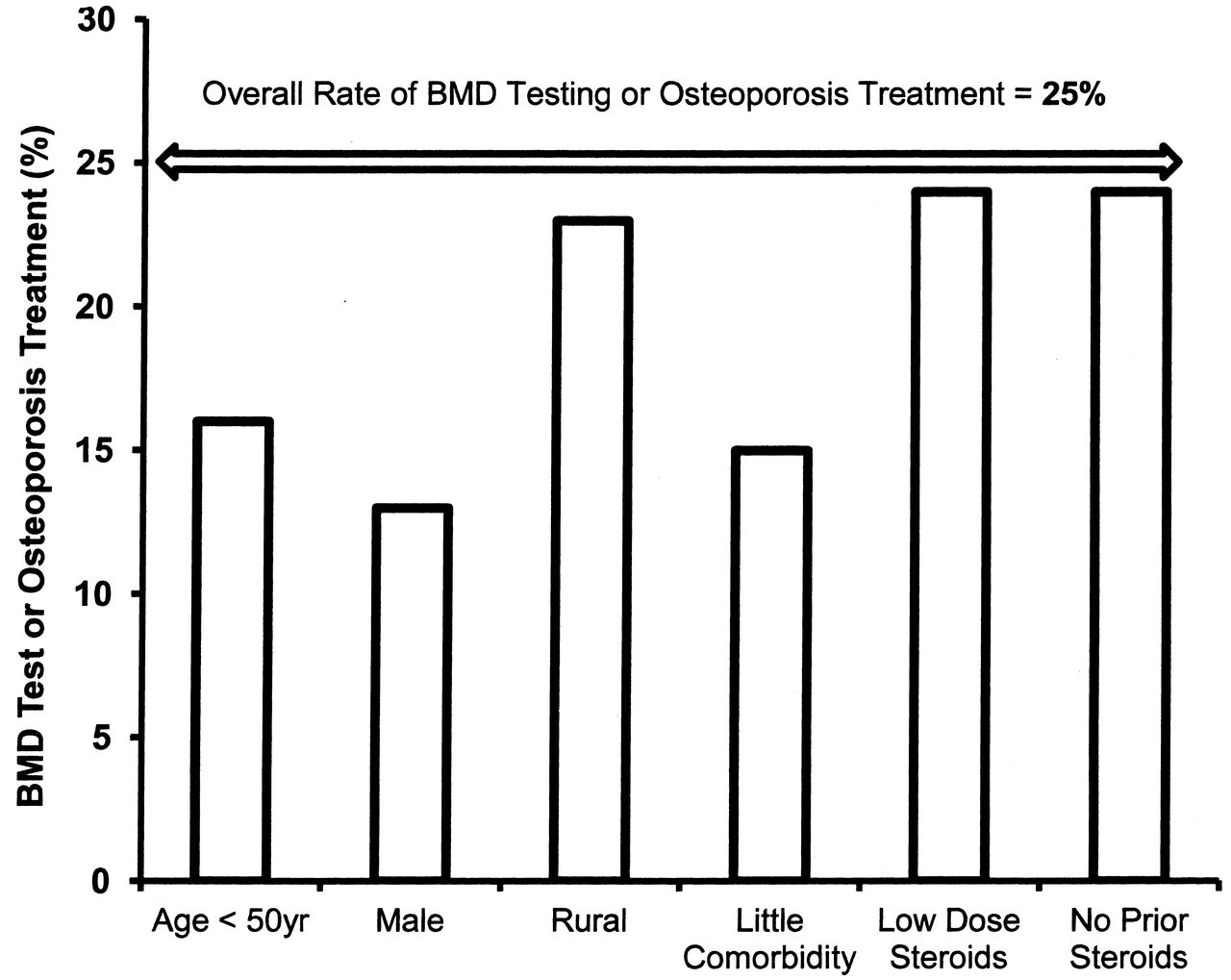
Overall, 3898 subjects (25%) received a BMD test or were prescribed osteoporosis medication within 6 months of GC initiation and 90% of those who received this high-quality GIOP preventive care were managed with osteoporosis medications. Table 1 presents subject characteristics according to whether high-quality GIOP preventive care was received. In general, those who did not receive BMD tests or osteoporosis treatments were significantly younger, more likely to be men, had fewer comorbidities, and were exposed to lower doses of GC than those who received BMD tests or treatments (Figure 1).

Factors significantly associated with a reduced likelihood of receiving GIOP-related preventive care, in unadjusted analyses. GIOP: glucocorticoid-induced osteoporosis; BMD: bone mineral density.
Characteristics of 15,285 new initiators of systemic glucocorticoids, according to whether they received high-quality GIOP preventive care.
Major osteoporotic fractures within 1 year
Within 1 year of GC initiation there had been 206 major fractures (1%), of which 97 were vertebral fractures and 49 were hip fractures. Those who received a BMD test or osteoporosis treatment within 6 months of a new GC use were more likely to have a major fracture within 1 year than those who did not receive high-quality GIOP preventive care [83 of 3898 (2%) vs 123 of 11,927 (1%) among those who did not receive high-quality care; p < 0.001 for difference]. In adjusted analyses, receipt of BMD test or osteoporosis treatment was not independently associated with a lower risk of major fracture within 1 year (adjusted OR 1.6, 95% CI 1.2–2.1). Findings were nearly identical in analyses restricted to the high-risk subgroup, who had 4 times the rate of major fractures at 1 year [42 fractures in 1194 subjects (4%) vs 1% in the overall cohort (adjusted OR 2.3, 95% CI 1.2–4.4)]. Older age, female sex, more than 1 hospitalization in the prior year, and high-dose GC were significantly associated with an increased risk of fracture within 1 year (Table 2).
Independent correlates of major fracture within 1 year of initiating glucocorticoids: multivariable logistic regression analyses.
Fractures within 3 years
Within 3 years of GC initiation there had been 553 major fractures (4%), of which 272 were vertebral and 129 were hip fractures. Again, those who received a BMD test or osteoporosis treatment within 6 months of a new GC treatment were more likely to have a major fracture within 3 years than those who did not receive high-quality GIOP preventive care [200 (5%) of 3898 vs 353 (3%) of 11,927 among those who did not receive high-quality care; p < 0.001 for difference]. In adjusted analyses, BMD test or osteoporosis treatment was not independently associated with a lower risk of major fracture (adjusted OR 1.3, 95% CI 1.1–1.6) or a lower risk of hip fracture (adjusted OR 1.0, 95% CI 0.6–1.4) within 3 years of newly initiating GC. Findings were nearly identical in analyses restricted to the high-risk subgroup, which had twice the rate of major fractures over 3 years [99 fractures (8%) vs 4% in the overall cohort (adjusted OR 1.8, 95% CI 1.2–2.7)]. Variables independently associated with an increased risk of a major osteoporotic fracture within 3 years were similar to those observed at 1 year (Table 3).
Independent correlates of major fracture within 3 years of initiating glucocorticoids: multivariable logistic regression analyses.
DISCUSSION
Our intent was to confirm or refute the validity of the commonly used performance measure of high-quality GIOP preventive care received after new systemic GC initiation5,6,7,8. In our cohort of more than 15,000 subjects starting longterm systemic GC, only one-quarter received high-quality GIOP preventive care, defined as a BMD test or osteoporosis treatment within 6 months of initiation. Despite this lack of attention to GIOP prevention, rates of major osteoporotic fracture were relatively low, with only 1% of subjects having a fracture within 1 year and 4% within 3 years.
Better-quality GIOP preventive care was not, as we had hypothesized or as is commonly assumed5,6,7,8, associated with a reduction in major fractures. Indeed, rates of fracture were significantly increased among those who received BMD testing or osteoporosis treatment. This is most likely a result of a treatment bias (i.e., confounding by indication), because patients who received better GIOP preventive care were older, frailer, more likely to receive bisphosphonates, and at generally higher risk of incident fracture than those who were neither tested nor treated for osteoporosis. We speculate that our counterintuitive findings occurred because the rates of BMD testing and osteoporosis treatment were so low. In other words, if appropriate GIOP-related care were more routine, with performance rates of 70%–80% (commonly attained in other settings, such as antiplatelet or ß-blocker use after acute coronary syndrome10), we may not have seen such profound treatment bias and confounding by indication.
In general, a valid quality metric or performance measure should be evidence-based and tightly linked to clinically important endpoints such as mortality or recurrent events. That is the standard that has been used in many other settings9,10,11,12,13. In the setting of fragility fracture, in 1 small randomized trial, adherence to the performance measure of “BMD test and bisphosphonate treatment if bone mass low” after a hip fracture was independently associated with a reduction in mortality and fracture20; in GIOP, Thomas and colleagues were able to demonstrate a reduction in clinical fractures with oral bisphosphonates in a sample of women, all of whom were already receiving bisphosphonates and subsequently began taking GC21. To our knowledge, the association between better performance of GIOP preventive care and outcomes has not otherwise been previously reported.
This study had several limitations. First, in attempting to replicate the performance measurement setting, we did not consider information related to subsequent GC exposures or adherence or persistence with osteoporosis treatments or even the type of osteoporosis medication dispensed. Our intent was not to examine the association between GC exposure and fracture nor the effectiveness of bisphosphonates in reducing fracture — rather, it was to determine whether better performance on a widely accepted quality metric would yield better outcomes. Our results suggest that there may not be an appropriate outcome to be measured using administrative data alone. An alternative outcome, such as increase or preservation of lumbar bone density or reduction in symptomatic major fractures and radiographically detected vertebral fractures, might be reasonable, but it would require a clinically rich database, with routine BMD testing and spinal radiographic followup.
Second, our definition of major fractures was based on claims data and by definition these were clinically symptomatic fractures that required medical attention16,17. Thus, we did not identify asymptomatic vertebral compression fractures, and these fractures are the type most commonly associated with GC exposure and the type of fracture most likely to be prevented by appropriate treatment with bisphosphonates or other agents2,3,4. While this means our overall recording of “major fractures” systematically underestimates the true fracture burden associated with GC initiation, it accurately reflects what would occur in any setting where serial spinal radiographic assessment is not the standard of care.
Third, we did not have detailed information regarding total absolute fracture risk, remote history of fragility fracture, or even BMD results, although our results do suggest that physicians were able to some degree to identify the patients with the very highest risk. Regardless, because of their age, need for immune suppression, and exposure to supraphysiologic doses of GC, most of these subjects would have been considered at clinically high risk of fracture.
Fourth (in terms of quality of care delivered), we do not know whether physicians ordered BMD tests that were not undertaken by patients or whether treatments were prescribed but not filled by patients. Of course, this is a major concern related to any audit activities addressing quality measurement. Lastly, although large and population-based, the study sample was drawn from only 1 Canadian province with universal healthcare coverage, and the results may not generalize to other patients or settings.
Using conventional administrative database analyses, we could not demonstrate that better compliance with the performance measure of BMD test or osteoporosis treatment after initiating longterm systemic GC therapy was associated with better outcomes, i.e., we did not observe a reduction in medically attended fractures. This does not mean that efforts to improve BMD testing or osteoporosis treatment in the setting of GIOP should be abandoned. But to better evaluate the true effectiveness of GIOP-related preventive care, more clinically rich databases and different (if not more sophisticated) analytic techniques will be needed. In the meantime, efforts should continue to improve the quality of GIOP-related preventive care as a general principle — although our results suggest that the “test or treat” quality metric is not sufficiently valid that it should be used as the basis for financial incentive or financial penalty programs such as pay-for-performance.
Acknowledgment
The authors acknowledge the Manitoba Centre for Health Policy for use of data contained in the Population Health Research Data Repository (HIPC project 2008/2009-16).
Footnotes
-
Supported by an unrestricted research grant from Amgen Canada Ltd. SRM holds the Endowed Chair in Patient Health Management (Faculties of Medicine and Dentistry and Pharmacy and Pharmaceutical Sciences, University of Alberta) and receives salary support as a Health Scholar (Alberta Heritage Foundation for Medical Research and Alberta Innovates — Health Solutions). LML is the recipient of a Manitoba Research Chair. SNM is a Clinical Research Fellow of the Fonds de la Recherche en Santé du Quebec.
- Accepted for publication April 4, 2013.








{kind=link}