
To the Editor:
Takayasu arteritis (TA) is a systemic vasculitis that affects large-size vessels such as the aorta and/or its main branches. Persistent inflammation of TA leads to segmental stenosis, occlusion, dilatation, and/or aneurysm formation. TA is also accompanied by somatic symptoms, including fever, fatigue, and weight loss, and elevation of acute-phase reactants such as C-reactive protein (CRP) that correlate with disease activity. Although high-dose corticosteroid (CS) therapy is effective in TA, CS alone does not provide sustained remission in about half of patients1. CS-resistant patients with TA have been treated with immunosuppressants, including methotrexate (MTX) and azathioprine1,2. Anti-tumor necrosis factor (anti-TNF) therapy3,4 and anti-interleukin 6 receptor antibody5,6 are also promising treatments for TA. However, the new therapies for CS-resistant TA have yet to be standardized. We describe a patient with TA who was successfully treated with tacrolimus, a calcineurin inhibitor, after failed trial of conventional CS, MTX, and infliximab (IFX). This case suggests that tacrolimus is another potential alternative treatment option for refractory TA.
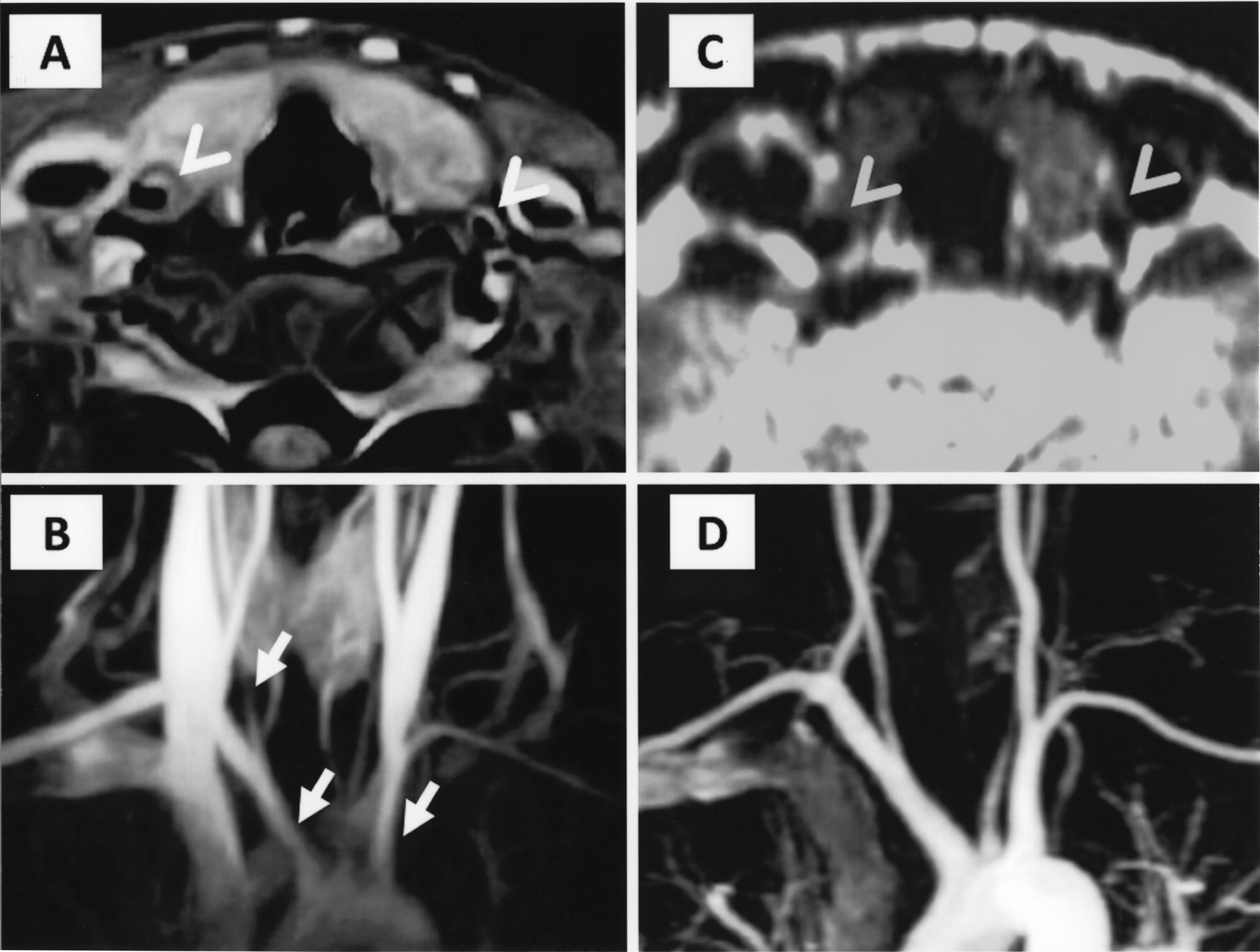
A 22-year-old woman was admitted to our hospital in August 2007 for persistent fever and neck pain. Examination showed tenderness around both carotid arteries, different blood pressures in the left and right upper extremities (right 109/54, left 90/47 mm Hg), weak left radial pulse, and murmur on the common carotid arteries and abdominal aorta. Blood analysis showed elevated CRP (10.3 mg/dl). Neck and chest magnetic resonance imaging (MRI) showed wall thickening and stenosis of the left common carotid artery and bilateral brachiocephalic arteries (Figure 1A, 1B). Based on these findings, she was diagnosed with TA. Treatment with 30 mg/day (0.6 mg/kg/day) prednisolone (PSL) relieved the symptoms and reduced CRP to within the normal range (< 0.05 mg/dl). The PSL dose was subsequently reduced to 10 mg/day.
{kind=link}
Neck and chest MRI findings. The left common carotid artery of this patient branches from the left brachiocephalic artery. A. T1-weighted image shows wall thickening of the left common carotid artery and right brachiocephalic artery (arrowheads). B. Magnetic resonance angiography shows stenosis of the right common carotid artery and bilateral brachiocephalic arteries (arrows) at diagnosis in August 2007. C. Magnetic resonance imaging in February 2011 during treatment with tacrolimus and subsequent sustained clinical remission shows normal vascular wall and (D) absence of new stenosis of arteries.
However, in April 2008, the patient developed fever and tenderness at the same location around carotid arteries, with high CRP (1.57 mg/dl), suggesting relapse of TA. Accordingly, the dose of PSL was escalated to 30 mg/day and combined with MTX. The combination treatment induced remission of TA again. Nevertheless, the disease activity became exacerbated again after reduction of PSL dose to 12.5 mg/day despite continuation of MTX at 12.5 mg/week. IFX was added to the treatment in March 2009 (3 mg/kg at weeks 0, 2, and 6 and then at 8-week intervals). Although the dose of IFX was subsequently increased to 8.5 mg/kg and the administration interval was shortened to every 6 weeks, neck tenderness did not disappear and CRP levels remained positive (0.40–0.97 mg/dl), suggesting the arteritis was still active. Consequently, 3 mg/day tacrolimus was added in February 2010 and the dosage was increased to 4 mg/day to maintain an adequate serum trough level (∼5 ng/ml). The CRP level decreased to normal range 5 weeks after start of tacrolimus, and remained within the normal range even after discontinuation of IFX in June 2010. The dose of PSL was subsequently tapered to 6 mg/day. MRI in February 2011 showed disappearance of the vascular wall thickening and absence of new stenosis of arteries (Figure 1C, 1D).
There is only limited evidence for the efficacy of immunosuppressants or biologics for CS-resistant TA1,2. Molloy, et al4 reported an uncontrolled series of 25 patients with TA who received anti-TNF therapy; remission with discontinuation of PSL was achieved in 15 patients (60%) and remission with PSL ≤ 10 mg/day in an additional 7 patients (28%). Three patients did not respond to anti-TNF therapy, similar to our patient.
A thorough search of the PubMed database revealed that this is the first case of TA treated successfully with tacrolimus in spite of failure of anti-TNF therapy. In addition, we identified 2 patients with TA who improved significantly with calcineurin inhibitors. In the first patient, tacrolimus was effective in a patient resistant to CS and intolerant to MTX7. Cyclosporine was effective in another patient with CS- and MTX-resistant TA8. Cyclosporine is another calcineurin inhibitor that shares similar immunosuppressive action with tacrolimus. Studies in the field of organ transplantation suggest that tacrolimus is more efficacious than cyclosporine9. Therefore, for treatment of TA, tacrolimus may also be more useful, although there is not enough evidence to date to compare the efficacy between tacrolimus and cyclosporine.
Our case suggests that tacrolimus is a potential alternative therapy for patients with CS-resistant or anti-TNF-resistant TA; further studies with large number of patients are needed to confirm the efficacy of tacrolimus for TA.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.