

Abstract
Objective. Promising therapeutic approaches have emerged in chronic periaortitis, whereas peripheral blood biomarkers are lacking. CC-chemokine ligand 18 (CCL18) is known as a marker of fibrotic activity and prognosis in pulmonary fibrosis. We investigated whether CCL18 levels are increased in patients with chronic periaortitis and are associated with clinical, laboratory, and imaging findings.
Methods. In this retrospective study, serum concentrations of CCL18 were assessed in 30 patients with chronic periaortitis and related to clinical data, laboratory variables, and imaging studies. Serum levels were compared to 15 apparently healthy volunteers and 15 controls with aortic sclerosis.
Results. Serum concentrations of CCL18 were increased in patients with chronic periaortitis (median 197.6 ng/ml, range 73.7–301.0) compared to healthy volunteers (median 34.6 ng/ml, range 22.6–70.4; p < 0.0001) and controls with aortic sclerosis (median 50.4 ng/ml, range 24.5–141.2; p < 0.0001). CCL18 levels correlated with (n = 30; r = 0.461, p = 0.01) and increased with the transversal diameter of the periaortic mantle < 5, 5–10, and ≥ 10 mm (p = 0.008). Contrast enhancement (p = 0.044), treatment naivety (p = 0.042), and the occurrence of systemic symptoms (p = 0.007) were associated with higher CCL18 levels. During followup, changes of CCL18 correlated with changes of the transverse diameter of the periaortic mantle (n = 17; r = 0.512, p = 0.033).
Conclusion. Serum concentration of CCL18 reflects fibroinflammatory activity and extent of disease in patients with chronic periaortitis.
Chronic periaortitis (CP) is characterized by fibroinflammatory tissue spreading from the abdominal aorta into the retroperitoneum, which often affects the ureters and the inferior vena cava, leading to obstruction of these structures1,2. Depending on the existence of aneurysmal dilatation of the abdominal aorta it was suggested to subdivide CP into a nonaneurysmal and an aneurysmal form, formerly known as idiopathic retroperitoneal fibrosis and inflammatory abdominal aortic aneurysm3. Although the etiology remains largely unknown, current research proceedings2,3,4,5,6 and the effectiveness of immunosuppressive treatment7,8,9,10,11,12,13,14,15,16,17,18,19,20 support the hypothesis of an autoimmune or immune-mediated pathogenesis. In the last decade, elevated serum levels of IgG4 and the presence of IgG4-secreting plasma cells in the affected tissues were identified in a subgroup of patients21,22,23,24. However, serum concentrations of IgG4 did not correlate with the extent or progress of the disease in a clinically relevant way23,25.
To date, no serum measure including C-reactive protein (CRP) has been reported to be informative in monitoring disease activity8. Identification of a serum biomarker reflecting disease activity and extent may reduce the necessity of frequent costly imaging and thus facilitate monitoring.
CC-chemokine ligand 18 (CCL18) was identified as a marker of fibrotic activity and prognosis in idiopathic pulmonary fibrosis, a rapid progressive interstitial lung disease26,27,28. Based on these data we retrospectively examined serum concentrations of CCL18 in patients with CP. CCL18 values were related to the patients’ symptoms, imaging findings, and laboratory parameters.
MATERIALS AND METHODS
Patients and imaging studies
Patients with CP and available serum samples referred to the University Medical Centre Freiburg between 2000 and 2010 were included in this retrospective study. In most patients (n = 27) the diagnosis of CP was based on imaging findings from contrast-enhanced computer tomography (CT) or magnetic resonance imaging (MRI), following the commonly accepted criteria (periaortic mass of soft-tissue density)29. In 3 patients the diagnosis was histologically verified. Patients with evidence or history for malignancy, documented use of ergot derivates, or other secondary causes were excluded, while patients with inflammatory aneurysms of the abdominal aorta (IAAA) were included for study. Apparently healthy volunteer controls, with no known cardiovascular morbidities, were recruited from medical staff. Patients treated in the Department of Cardiology, University Medical Centre Freiburg, with suspected or evident coronary heart disease were included as a validation cohort. Key inclusion criterion was documented aortic sclerosis in imaging studies (ultrasonography or CT). Patients with clinical or imaging signs of acute infection were excluded. Medical histories and cardiovascular risk factors [body mass index (BMI), diabetes mellitus, hypercholesterolemia, and hypertension], symptoms, and laboratory measurements were collected retrospectively from charts of patients with CP and aortic sclerosis.
Contrast-enhanced MRI scanning (1.5 Tesla body scanner; Siemens, Munich, Germany) was performed in 28 of 30 patients using a dedicated abdominal coil. Spin-echo T1-weighted transversal slices were obtained before and after intravenous administration of a gadolinium contrast enhancing agent (gadolinium-diethylene triamine pentaacetic acid 0.2 mmol/kg body weight). Additionally, fast spin-echo T2-weighted transversal and sagittal slices were obtained. Contrast-enhanced CT was performed in 2 patients. In 2 patients image scans were performed without contrast enhancement because of impaired renal function. The transverse diameter of the periaortic mantle, its longitudinal extension, contrast enhancement, and existence of urinary tract obstruction and vascular involvement (renal or iliac vessels or the inferior vena cava) were analyzed in a blinded manner (before determination of CCL18 serum concentrations). Contrast enhancement was compared to the adjacent psoas muscle (isointense = no contrast enhancement; hyperintense = contrast enhancement). For comparison, serum samples of 15 healthy controls were analyzed. The study was approved by our local ethics committee.
Measurement of CCL18 serum concentrations
Serum concentrations of CCL18 were analyzed using a DuoSet ELISA Development Kit (R&D Systems Europe, Bad Nauheim, Germany). All serum samples were measured as duplicates in 1 ELISA plate.
Statistical analysis
All measures are shown as median values and range. For comparison of subgroups either nonparametric Mann-Whitney U test (2 groups) or Kruskal-Wallis rank-sum test (more than 2 groups) was used. Spearman’s rank correlation coefficient was calculated to describe the relationship of different variables. Fisher’s exact test was used to compare the distribution of clinical characteristics between patients and controls. Probability values < 0.05 were considered significant. SPSS (version 17, IBM Corp., New York, NY, USA) and GraphPad Prism (GraphPad Software Inc., San Diego, CA, USA) were used for database management and statistical analysis.
RESULTS
Study subjects
A total of 30 patients with CP were eligible for study. Two patients had elevated serum IgG4 concentrations (> 135 mg/dl)22, whereas 6 patients had IAAA. No included patient had evidence of pulmonary fibrosis, whereas 5 patients had chronic obstructive pulmonary disease. Only 5 patients were treatment-naive; 25 patients had already received different immunosuppressive treatment regimens (oral corticosteroids, cyclophosphamide, azathioprine, methotrexate, or mycophenolic acid) at the time of serum sampling. Not all measures could be obtained for all patients. For comparison the CCL18 serum concentrations of healthy controls (n = 15) and controls with aortic sclerosis (n = 15) were measured. The demographic and clinical characteristics of patients with CP and controls with aortic sclerosis are shown in Table 1.
Demographics and clinical characteristics of subjects. Values are depicted as medians (quartiles) unless otherwise indicated.
CCL18 serum concentrations in patients with CP
Serum concentrations of CCL18 were increased in patients with CP (n = 30; 197.6, 73.7–301.0 ng/ml) in comparison to healthy controls (n = 15; 34.6, 22.6–70.4 ng/ml; p < 0.0001) and controls with aortic sclerosis (n = 15; 50.4, 24.5–141.2 ng/ml; p < 0.0001). CCL18 levels were slightly increased in patients with aortic sclerosis compared to healthy controls; however, this difference did not reach statistical significance (p = 0.065; Figure 1). There was no significant difference between healthy controls and patients with CP regarding age (57.0, 48.0–64.0 yrs, vs 59.0, 33.0–85.0 yrs, respectively; p = 0.181) and sex (female/male = 7/8 vs 14/16; p = 0.625). Also, controls with aortic sclerosis did not differ in age (66.0, 47.0–75.0 yrs; p = 0.181) and sex (female/male = 5/10; p = 0.526) compared to patients with CP.

CCL18 serum concentrations of patients with chronic periaortitis (CP) in comparison to healthy controls and controls with aortic sclerosis. CCL18 serum concentrations of patients with CP (n = 30) were significantly increased compared to healthy volunteers (n = 15). Bars represent median values. **p < 0.001.
CCL18 serum concentration and clinical/laboratory data
CCL18 serum concentrations were not correlated with age (n = 30; r = 0.196, p = 0.299) and there was no difference between female (n = 14) and male (n = 16) patients (187.4, 125.8–293.6 ng/ml, vs 208.5, 73.7–301.0 ng/ml; p = 0.506). CCL18 levels were not different between smokers (n = 23; 206.8, 73.7–301.0 ng/ml) and nonsmokers (n = 4; 173.1, 125.8–201.7 ng/ml; p = 0.172). Patients with systemic symptoms such as night sweats, fever, or weight loss (n = 5) showed higher serum concentrations of CCL18 compared to patients without systemic symptoms (293.6, 210.1–301.0 ng/ml, vs 181.2, 73.7–294.9 ng/ml; p = 0.007); whereas the presence of pain (n = 9) was not associated with significantly higher levels of CCL18 (250.6, 140.2–301.0 ng/ml, vs 181.2, 73.7–294.9 ng/ml; p = 0.118). Patients without immunosuppressive pretreatment (n = 5) showed significantly higher serum concentrations of CCL18 (258.6, 201.7–301.0 ng/ml, vs 181.2, 73.7–294.9 ng/ml; p = 0.042; Figure 2). There was no significant difference of CRP or erythrocyte sedimentation rate (ESR) values in the subgroups’ systemic symptoms (p = 0.082; p = 0.228), pain (p = 0.339; p = 0.287), and immunosuppressive pretreatment (p = 0.296; p = 0.228).

CCL18 serum concentrations and clinical findings. There was a difference between CCL18 serum concentrations of patients with systemic symptoms (n = 5) compared to patients without symptoms (n = 25). Patients with previous immunosuppressive treatment (n = 25) revealed lower CCL18 concentrations in comparison to treatment-naive patients (n = 5). Bars represent median values. *p < 0.05.
There was no significant difference of CCL18 levels between aneurysmal (n = 6) and nonaneurysmal forms of CP (p = 0.407). CCL18 serum concentrations did not correlate with CRP (n = 23; r = 0.397, p = 0.061), ESR (n = 19; r = 0.243, p = 0.316), or leukocytes (n = 28; r = −0.168, p = 0.394).
CCL18 serum concentrations and imaging studies
There was a significant positive correlation between CCL18 and the transverse diameter of the periaortic mantle (n = 30; r = 0.461, p = 0.01; Figure 3), whereas no correlations of diameter were observed with CRP (n = 23; r = 0.382, p = 0.072) or ESR (n = 19; r = 0.252, p = 0.298). Serum CCL18 concentrations increased with the transverse diameter of the periaortic mantle (< 5 vs 5–10 vs ≥ 10 mm; p = 0.008; Figure 3). Extensive vascular involvement (n = 25; p = 0.211) and urinary tract obstruction (n = 6; p = 0.233) were not associated with higher concentrations of CCL18. Patients with contrast enhancement of the lesions in imaging studies (n = 18; either MRI or CT) showed higher CCL18 serum concentrations compared to patients without (n = 10; 234.8, 140.2–301.0 ng/ml, vs 179.2, 73.7–225.1 ng/ml; p = 0.044; Figure 3). CRP and ESR values did not differ between patients with and those without contrast enhancement in imaging studies (p = 0.107; p = 0.983).

CCL18 serum concentrations and imaging findings. CCL18 serum concentrations were found to increase with the transverse diameter of the periaortic mantle (Kruskal-Wallis rank-sum test). There was a correlation between the transverse diameter and CCL18 serum concentration (n = 30; r = 0.461, p = 0.01). Patients with contrast enhancement on imaging studies (n = 18) had significantly higher CCL18 serum concentrations than patients without enhancement (n = 10). Bars represent median values. *p < 0.05.
For 17 patients, serum CCL18 measurements and imaging studies were available during the followup of immunosuppressive treatment (median followup time 11, 2–40 mo). A correlation between the changes of diameters and the changes of serum CCL18 concentrations was observed (n = 17; r = 0.512, p = 0.033; Figure 4). These patients received immunosuppressive treatment with cyclophosphamide and oral corticosteroids (n = 5), azathioprine and oral corticosteroids (n = 5), methotrexate and oral corticosteroids (n = 3), oral corticosteroids alone (n = 3), or mycophenolic acid and oral corticosteroids (n = 1).
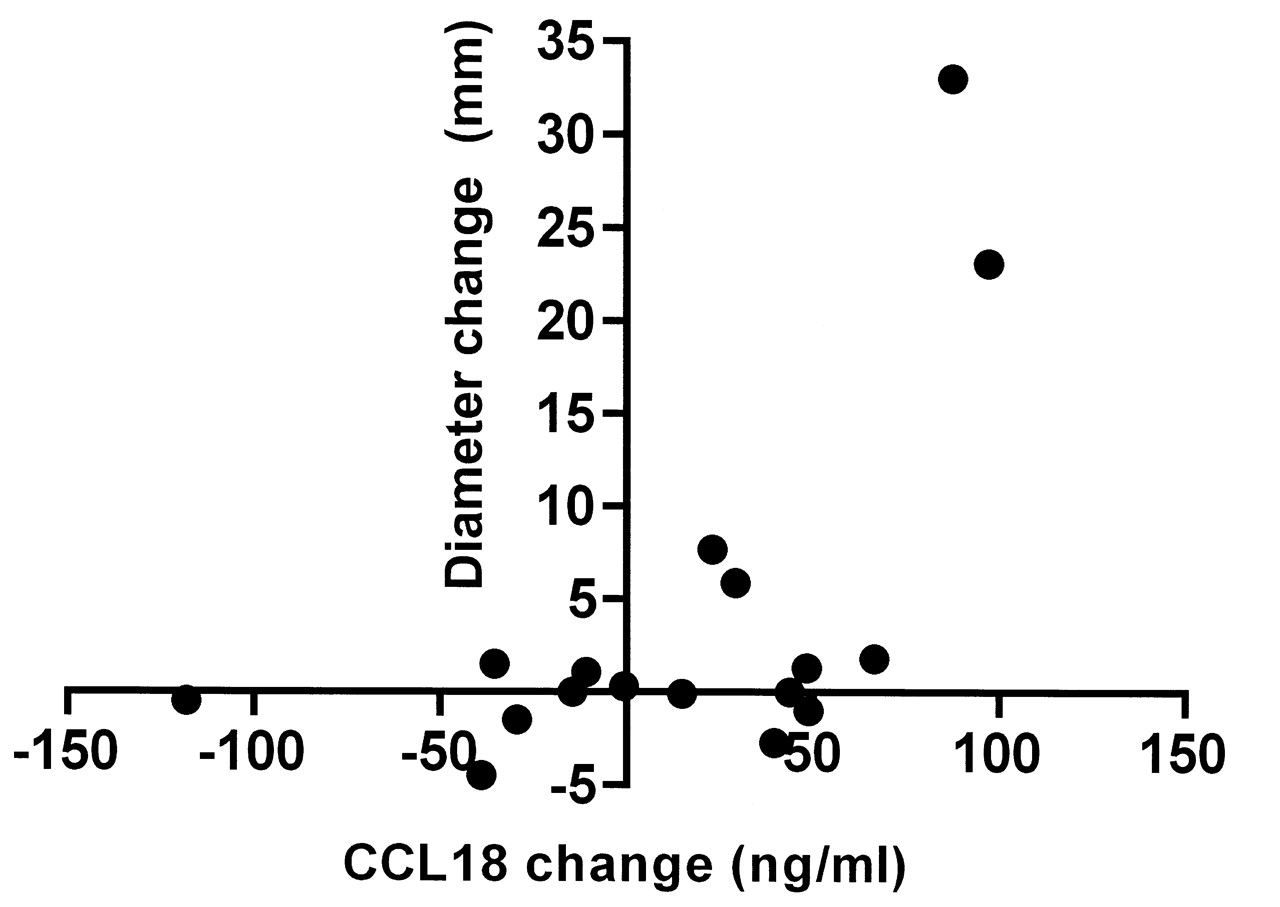
CCL18 concentrations in followup. A correlation was observed between changes of diameters of the periaortic mantle in imaging studies and CCL18 serum concentrations (n = 17; r = 0.512, p = 0.033).
CCL18 serum concentrations and cardiovascular morbidities
Cardiovascular morbidities of patients with CP and controls with aortic sclerosis are shown in Table 1. There were no differences of CCL18 serum concentrations in CP patients with diabetes mellitus (n = 5; p = 0.198), arterial hypertension (n = 19; p = 0.198), hypercholesterolemia (n = 12; p = 0.983), obesity (BMI ≥ 30 kg/m2, n = 3; p = 0.178), coronary heart disease (n = 5; p = 0.330), and peripheral vascular disease (n = 5; p = 0.706). These cardiovascular morbidities were similarly distributed among the subgroups analyzed (contrast enhancement vs no enhancement, systemic symptoms vs no symptoms, immunosuppressive pretreatment vs no pretreatment; p > 0.1 for all comparisons).
DISCUSSION
While effective immunosuppressive treatment regimes are available for CP7,8,9,10,11,12,13,14,15,16,17,18,19,20, monitoring the therapeutic response still requires numerous costly imaging studies (MRI or CT) because of the lack of a specific and suitable biomarker. Neither CRP nor ESR is effective to reveal the severity of disease in CP8,25. Our study shows for the first time that serum concentrations of CCL18 were elevated in patients with CP compared to healthy controls. Serum levels of CCL18 correlated with the extension of fibroinflammatory tissue in CP and the inflammatory activity indicated by contrast enhancement in MRI or CT scans4. The presence of systemic symptoms (fever, weight loss, night sweats) was associated with higher levels of CCL18 and the initial values of untreated patients were higher than respective values of treated patients. On the other hand, CCL18 levels were not different in aneurysmal and nonaneurysmal forms of CP, nor in smokers and nonsmokers, rendering CCL18 a valuable serum marker for extent of disease and disease activity independent of these potentially confounding factors. In addition, CCL18 serum concentrations were significantly correlated with reduction of the transverse diameter of the periaortic mantle during followup.
CCL18 is known to stimulate collagen synthesis of fibroblasts and plays an important role in wound healing and fibrogenesis26. In pulmonary fibrosis, CCL18 has become a known marker of disease activity. It has been shown that macrophages produce elevated levels of CCL18 in serum and bronchoalveolar lavage26,27,28. These macrophages are characterized by a phenotype of alternative activation and are known to play an important role in the pathogenesis of pulmonary fibrosis29. For peritoneal fibrosis due to dialysis it has also been shown that alternatively activated macrophages are associated with fibrosis of the peritoneal membrane. Moreover, CCL18 concentrations were elevated in peritoneal effluents of these patients30,31. The retroperitoneal fibroinflammatory tissue in CP contains lymphocytes, plasma cells, and eosinophils in addition to numerous macrophages32. To date, the role of macrophages in the pathogenesis of CP has not been analyzed in depth. Our data suggest for the first time the possible involvement of alternatively activated macrophages in the fibrotic process occurring in CP, indicated by the highly elevated serum concentrations of CCL18. CCL18 is also expressed in macrophages associated with atherosclerotic plaques, and plasma concentrations of CCL18 are increased in patients with refractory angina pectoris33,34. Because there are some links between CP and atherosclerosis35, we analyzed serum levels of CCL18 with regard to cardiovascular morbidity. Moreover, we compared the CCL18 serum concentrations that were obtained with those of a cohort of 15 controls with aortic sclerosis. However, there were no associations between CCL18 and cardiovascular morbidities.
Our study is limited by the small number of patients, especially in the subgroups. Several statistical analyses suggest a relationship between CCL18 serum concentrations and disease activity and extent, but larger prospective trials are needed to verify these first promising results.
Our study reveals that serum concentrations of CCL18 are highly elevated in patients with CP and reflect disease extent and activity throughout the disease course. Further studies are required to estimate the value of CCL18 for diagnosis and monitoring purposes in CP.
- Accepted for publication March 29, 2012.








{kind=link}
{kind=link}
{kind=link}
{kind=link}