
Abstract
Objective. (1) To describe a series of adults assessed for suspected primary angiitis of the central nervous system (PACNS) and their final diagnosis; (2) to describe and compare presenting features of PACNS and reversible cerebral vasoconstriction syndrome (RCVS); and (3) to evaluate the specificity of the presenting features of RCVS.
Methods. Patients evaluated at our institution between 2000 and 2008 for a possible CNS vasculitis and investigated by conventional angiography and/or brain biopsy were retrospectively analyzed. The inclusion criteria were a clinicoradiological presentation and cerebral angiography and/or brain biopsy raising the hypothesis of isolated cerebral vasculitis; and absence of identifiable etiology at the time of conventional angiogram and/or brain biopsy.
Results. Among 58 cases evaluated, 37 met the inclusion criteria and 33 were included in the study. Thirteen patients had RCVS. Thunderclap headaches, the absence of a focal neurological deficit, a convexal subarachnoid hemorrhage and/or normal brain parenchyma on magnetic resonance imaging, and “string of beads” appearance on conventional angiography had high diagnostic value. Six patients had other noninflammatory vascular disorders (intracranial atherosclerosis, cryptogenic embolism, and genetic vasculopathy). Six patients had infection or malignancy. Eight patients were diagnosed with PACNS; their clinical presentation and disease course were heterogeneous. Brain biopsy was performed in 3 cases (positive in 1).
Conclusion. RCVS is an important differential diagnosis of CNS vasculitis. Its particular presentation should allow rapid identification in order to avoid pointless investigations and treatment. The frequent lack of histological proof and heterogeneous presentation of PACNS illustrated the nosological uncertainties of this label.
- CEREBRAL ARTERIAL DISEASES
- VASCULITIS
- CENTRAL NERVOUS SYSTEM
- INTRACRANIAL VASOSPASM
- DIFFERENTIAL DIAGNOSIS
Adult central nervous system (CNS) vasculitides are a heterogeneous group of diseases that can lead to severe disability and death. They can result from many causes such as infection, cancer, drug exposure, or systemic inflammatory disorders. Idiopathic cases are referred to as primary angiitis of the CNS (PACNS), a rare condition first reported a half-century ago that is still poorly understood1,2.
Given the limited diagnostic performance of current radio-diagnostic procedures3,4,5,6,7,8 and the large and increasing number of mimics of PACNS1,9, the diagnosis of PACNS is often challenging. Indeed, nothing but histopathology can definitively confirm the diagnosis1,2,3,4,5, even if high-resolution magnetic resonance imaging (MRI) with contrast enhancement has recently emerged as a promising approach to demonstrate intracranial vessel wall inflammation10,11,12.
Diagnostic criteria for PACNS proposed by Calabrese and Mallek almost 25 years ago are the following13: (1) the presence of an acquired otherwise unexplained neurological or psychiatric deficit; (2) the presence of either classic angiographic or histopathological features of angiitis within the CNS; and (3) no evidence of systemic vasculitis or any disorder that could cause or mimic the angiographic or pathological features of the disease. Hence, the exclusion of alternative diagnoses is an essential part of the approach to CNS vasculitides1,2,9. However, studies investigating the differential diagnosis of PACNS are scarce. Further, they likely do not reflect the whole spectrum of PACNS mimics since they arise from tertiary care centers and include a high proportion of patients who had undergone a brain biopsy3,5. This increases diagnostic certainty but may result in recruitment bias toward more severe and/or rare diseases.
The reversible cerebral vasoconstriction syndrome (RCVS) is a recently delineated and probably underrecognized entity that can be easily mistaken for CNS vasculitis. It is characterized by the association of recurrent “thunderclap” headaches with or without neurological symptoms and dynamic angiographic abnormalities consisting of multifocal cerebral artery narrowings that resolve spontaneously within 1 month to 3 months. Whereas the initial clinicoradiological presentation of RCVS has recently been clarified14,15, its specificity has not been evaluated. Therefore, the diagnosis of RCVS is often retrospective14,16, which can pose difficult diagnostic and therapeutic dilemmas in severe cases.
The objectives of our study were (1) to describe a series of adults assessed for a suspected primary angiitis of the central nervous system and their final diagnosis; (2) to describe and compare presenting features of PACNS and RCVS; and (3) to evaluate the specificity of the clinicoradiological features of the RCVS at presentation.
MATERIALS AND METHODS
Patients
The computerized database of the Neuroradiology Department of Nantes University Hospital was searched for patients who had undergone cerebral angiography between January 1, 2000, and January 1, 2008, and cases in which the keywords “vasculitis,” “angiitis,” “arteritis,” or “angiopathy” appeared in the report and/or in the requisition report. Further, the computerized database of the Pathology Department was searched for patients who had undergone brain biopsy in the same period, for which a diagnostic code of vasculitis was used. Inclusion criteria were (1) clinicoradiological presentation and cerebral angiography and/or brain biopsy raising the hypothesis of cerebral vasculitis; (2) absence of identified etiology at the time of the first invasive procedure (i.e., conventional angiogram or brain biopsy); (3) at least 1 clinical evaluation performed at our center; and (4) age > 18 years at presentation.
Neuroimaging review, data collection and reporting
For each patient, all computed tomography (CT) scans, MRI scans, and cerebral angiographies were reviewed by a senior neuroradiologist (EAC).
The histopathologic diagnosis of PACNS required a transmural inflammation of small or medium-size blood vessels of the meninges and/or cortex of the brain. Inflammation could or could not be granulomatous. Perivascular mononuclear infiltrates without vessel wall damage were not considered as diagnostic of vasculitis. All brain biopsies were performed before initiation of treatment. Appropriate stainings and lymphocyte markers were performed to exclude infection and lymphoma. Electron microscopy was not performed.
Clinical data were obtained through extensive medical chart review (by AN). Followup information was also obtained from telephone interviews with patients and/or general practitioners. Data collection included demographic data, time from symptom onset to neurological investigation, clinical presentation at onset of disease and during followup, cardiovascular risk factors, medications, drug abuse, cardiovascular assessment, and laboratory, imaging, and pathological findings. Treatment and response to therapy were collected from the chart, and the Rankin score at presentation was calculated retrospectively, based on clinical notes.
All cases were evaluated by a senior neurologist (BG) and a senior neuroradiologist (EAC), both trained in neurovascular diseases, as well as 2 senior internists trained in rare systemic and immune-mediated diseases (AN, MAH). All patients had undergone extensive investigations in order to rule out infection, malignancy, hypercoagulability, and systemic or neurologic immune-mediated diseases.
Diagnostic criteria
The diagnosis of PACNS relied on diagnostic criteria proposed by Calabrese and Mallek13. When neither conventional angiogram nor brain biopsy were informative (2 cases) the diagnosis relied on the following: (1) clinical signs of focal or global cerebral injury; (2) ischemic, hemorrhagic, and/or inflammatory lesion(s) on MRI; (3) worsening or relapsing clinical course; and (4) no identifiable alternative diagnosis after extensive investigation and 2 years of followup. Patients with either positive biopsy or vessel wall inflammation on MRI, or both typical angiogram and meningitis, were considered as having definite PACNS. Patients who did not undergo brain biopsy and who had a normal angiogram were considered as possible PACNS. Others were considered probable PACNS.
The diagnostic criteria of RCVS in our study were comparable to those suggested previously14,15,16: (1) recent onset headaches with or without associated neurological deficits and/or seizures; (2) multiple intracranial artery stenosis; (3) complete resolution of symptoms within 2 months; (4) exclusion of alternative diagnosis; and (5) regression of vascular abnormalities within 4 months. When imaging followup was not available before this timepoint the patient had to have fully recovered without specific treatment (including steroids) and fulfill the diagnostic criteria of benign angiopathy of the CNS (an older term for RCVS), as described in the International Classification of Headache Disorders (ICHD), second edition17.
The diagnosis of neoplastic, infectious, and genetic diseases relied on appropriate laboratory tests. All other diagnoses, including intracranial atherosclerosis and cryptogenic embolism, were made by consensus (AN, MAH, BG, and EAC). Data are summarized as frequencies and percentages for categorical variables. Quantitative variables are presented as mean (range).
Statistical analysis
Differences between patients with RCVS and patients with PACNS were analyzed using a nonparametric Mann-Whitney U test for quantitative variables, Fisher’s exact probability test for frequency comparisons, and chi-square with simulation for qualitative variables.
The specificity of the presenting clinicoradiological features of RCVS was evaluated by focusing on 24 patients presenting with an acute angiographically defined CNS vasculopathy, as follows: (1) abrupt onset of headaches and/or focal deficits, (2) disease duration < 3 weeks before admission, and (3) multiple (≥ 2) stenoses on multiple (≥ 2) intracranial arteries at angiography. Hence these patients fell into 2 categories: RCVS (n = 13) and other acute angiographically defined CNS vasculopathies (n = 11: infection or malignancy in 4, intracranial atherosclerosis in 3, PACNS in 3, and cryptogenic embolism in 1). These 2 groups were compared using the above tests. Sensitivity, specificity, and predictive value of features overrepresented in the RCVS group were determined using the group of 24 patients as the denominator.
RESULTS
Cohort characteristics and final diagnoses
The selection process for cases for study is illustrated in Figure 1. The database search identified 58 patients. Seventeen patients were excluded because neither clinical, radiological, nor pathological findings suggested cerebral vasculitis. Their diagnoses are reported in Figure 1. Eight additional patients were excluded because they had not been clinically evaluated at our institution and/or due to missing data.

Selection process of cases for study. PACNS: primary angiitis of the central nervous system; RCVS: reversible cerebral vasoconstriction syndrome.
Thirty-three patients were included in the study. There were 26 women and 7 men, with mean age 49 years (range 21–71 yrs). At the end of the study (June 2009) mean followup was 33 months (range 0–108). Among these 33 patients, 13 had RCVS, 8 had PACNS, 6 had cerebral vasculopathy related to infection or malignancy, 3 had intracranial atherosclerosis, 2 had cryptogenic embolism, and 1 had a rare late-onset genetic vasculopathy.
Most patients (31 of 33) were hospitalized at our institution through the emergency department because of a recent history of acute-onset focal neurological deficit (27 of 31), headaches (22 of 31), and/or seizures (2 of 31). Two other patients were referred for a 6-month history of progressive focal neurological deficits.
The mean intervals from first symptoms to neuroradiological examination (CT or MRI) and first invasive procedure (angiogram or brain biopsy) were as low as 16.3 days and 63.5 days, respectively. The median intervals were 2.5 days and 11 days, respectively. The suspicion of cerebral vasculitis was raised at presentation in all patients, based on clinical history and neuroradiological findings.
Neuroradiological examination (CT and/or MRI and/or conventional angiogram) was abnormal in all 33 cases. Cerebromeningeal abnormalities were found in 31 cases (90%), mainly consisting of cerebral infarct (15 of 31) and/or intracranial hemorrhage (13 of 31). Only 4 patients had nonischemic abnormalities (focal intracerebral mass or inflammatory process in 3 cases, diffuse meningeal enhancement and cerebral edema in 1 case). All patients but 1 had cerebral angiography, which was abnormal in 27/31 (84%) cases. Only 4 patients underwent a brain biopsy.
Miscellaneous
Six patients had various noninflammatory vascular disorders other than RCVS, including intracranial atherosclerosis in 3, cryptogenic embolism in 2, and COL4A1 gene mutation-related vasculopathy in 1. The latter presented with brain stem hemorrhage, diffuse leukoencephalopathy, and a highly abnormal cerebral angiogram and was suspected of having PACNS for several years before a correct diagnosis of genetic vasculopathy was made. Family history and retinal vasculopathy, 2 suggestive features of the disease, were recognized only during followup.
Six patients had malignancy or infection-related cerebral vasculopathy. In most cases, radiological presentation and/or routine biological tests pointed to the underlying disease, which could be identified within days to weeks after disease onset. However, in 2 cases of primary cerebral lymphoma, the correct diagnosis was made after several months. In 1 case, a first brain biopsy disclosed a granulomatous angiitis and led to a diagnosis of mass-lesion type PACNS. Corticosteroid therapy resulted in clear clinicoradiological improvement, but neurological status worsened after steroid tapering, warranting a second brain biopsy that yielded the correct diagnosis. Among these 6 patients with malignancy or infection, 5 died. In 3 cases death occurred within 3 months after presentation.
Reversible cerebral vasoconstriction syndrome
Thirteen patients had RCVS (Table 1), 12 women and 1 man, with mean age 52.9 years. Mean followup was 33 months (range 3–98 mo).
Characteristics of patients with reversible cerebral vasoconstriction syndrome (RCVS) and primary angiitis of the central nervous system (PACNS) and comparison of initial features.
Whereas time from disease onset to presentation was similar in both groups, clinicoradiological presentations of PACNS and RCVS were strikingly different. The main clinicoradiological features of RCVS and comparison with PACNS are reported in Table 1.
RCVS occurred during the postpartum period (under bromocriptine therapy) in 1 case, and after cocaine intake in the only male patient. Neither nasal decongestant nor antidepressant-related cases were seen.
Recent-onset headaches were a prominent feature of clinical presentation in all patients and were described as similar to a thunderclap in 10 of 13 cases. Half the patients suffered focal deficits. Brain imaging revealed acute infarct and/or hemorrhage in 10 of 13 (67%) patients. The most frequent abnormality was convexal subarachnoid hemorrhage (cSAH; Figure 2). Of note, this picture was not seen in other conditions.

Reversible cerebral vasoconstriction syndrome: A. Computed tomography scan shows cortical subarachnoid hemorrhage (star). B. Conventional angiogram shows “string of beads” appearance on several medium-size arteries. C. Angiogram shows regression of arterial abnormalities 3 months later.
Six patients received no other therapy than analgesics, 5 were treated with calcium channel blockers, and 4 with steroids. The regression of vascular abnormalities could be demonstrated in 9 of 13 patients (70%), using either repeated conventional angiography (n = 4) or noninvasive vascular imaging (MR or CT angiography; n = 5). The first followup vascular imaging was performed within 4 months in 77% of cases (mean 3.7 months, range 1–8). For the remaining 4 patients, the regression of vascular abnormalities could not be assessed. In 3 cases initial angiographic lesions were below the resolution threshold of the noninvasive vascular imaging and followup conventional angiography was not performed because of the favorable clinical course. A single patient did not undergo any followup vascular imaging. However, these 4 patients had a typical clinicoradiological presentation and a rapid resolution of their symptoms without specific therapy. Further, they fulfilled the International Classification of Headache Disorders diagnostic criteria for benign angiopathy of the CNS and had prolonged followup (mean 36 months, range 24–85).
Patients who had received steroids did not differ from other RCVS cases in terms of disease presentation and outcome. Treatment duration was 3 weeks in 1 patient and 3, 5, and 12 months for the other 3 patients. Reversibility of vascular lesions was demonstrated within 4 months in these 4 cases.
At last followup, 2 patients had neurological sequelae. One patient had a well-documented second episode within minutes after the followup angiography performed 9 months after the first attack.
In order to assess the specificity of the clinicoradiological presentation of the RCVS at onset, we compared initial characteristics of these patients with those of 11 other patients who also presented with an acute angiographically defined CNS vasculopathy. Of note, 4 of 11 patients from the control group worsened within 3 months after presentation, including 3 patients who died. Univariate analysis revealed that several clinical and radiological features were highly associated with the diagnosis of RCVS (Table 2). Expectedly, this included thunderclap headaches, the absence of a focal neurological deficit, a low modified Rankin score, cSAH, and/or a normal brain parenchyma on MRI, and “string of beads” appearance on conventional angiography (all p < 0.05). Sensitivity, specificity, and predictive value of these features are reported in Table 3.
Reversible cerebral vasoconstriction syndrome (RCVS) versus other acute angiographically defined central nervous system vasculopathies. Data are mean (range) or proportions.
Diagnostic value of the RCVS features at onset.
Patients with PACNS
Eight patients were considered as having PACNS, 5 women and 3 men, with mean age 41 years (range 26–60 yrs). Mean followup was 44 months (range 18–108 mo). Three patients had definite PACNS, 4 had probable PACNS, and 1 had possible PACNS.
Six of 8 patients presented with a cryptogenic cerebral infarct. In all but 1 case, signs of past ischemic brain injury (5 of 6) and/or intracerebral arterial narrowing (3 of 6) were noted at first evaluation and led to suspicion, among other possibilities, of cerebral angiitis. Five of 6 patients had angiographic abnormalities at presentation and/or during followup (Table 1). These were heterogeneous and frequently mild. Further, they could appear and/or worsen over time, as seen for 3 of 4 patients who underwent 1 or more followup angiograms. One patient with a prominent angiogram and cerebrospinal fluid abnormalities was reexamined 1 month after initiation of immunosuppressive therapy and showed a slight improvement. The other 3 patients were investigated after the onset of a new neurological deficit, 5 to 12 months after their first angiogram, performed at presentation. The followup angiogram found a new vascular lesion in all 3 cases, the initial angiogram being normal in 2 cases. A brain biopsy was performed in only 1 case and was inconclusive.
Among the remaining 2 patients, 1 presented with an ischemic and contrast-enhancing intracerebral lesion and the other with an unexplained meningoencephalitis, with intracranial hypertension, white-matter lesions, and papilloedema. The hypothesis of CNS vasculitis was raised by MRI findings in both cases. These patients underwent a brain biopsy, which showed evidence of CNS vasculitis in 1 patient, consisting of vasculocentric lymphocytic inflammatory infiltrates that penetrated the vessel wall. Both patients responded to corticosteroids. After 2 years of followup, no infectious, immune-mediated, or malignant disease had emerged, and the disease had not relapsed.
Six of 8 patients were treated with corticosteroids and/or immunosuppressants, generally within the first weeks to months after first symptoms. Three patients presenting with cerebral infarcts were initially left untreated for more than 2 years because of a favorable clinical course, which left doubts about the diagnosis of PACNS. Two of them had no further neurological episodes after 26 months and 30 months of followup. However, the third case, who had been left untreated for almost 8 years, silently developed multiple intracranial arterial stenoses, eventually causing several strokes over a few months (Figure 3). Vessel-wall enhancement on MRI and clinical and radiological responses to immunosuppressive therapy (steroids plus cyclophosphamide, then azathioprine) led to retention of the diagnosis of PACNS.

{kind=link}
{kind=link}
{kind=link}
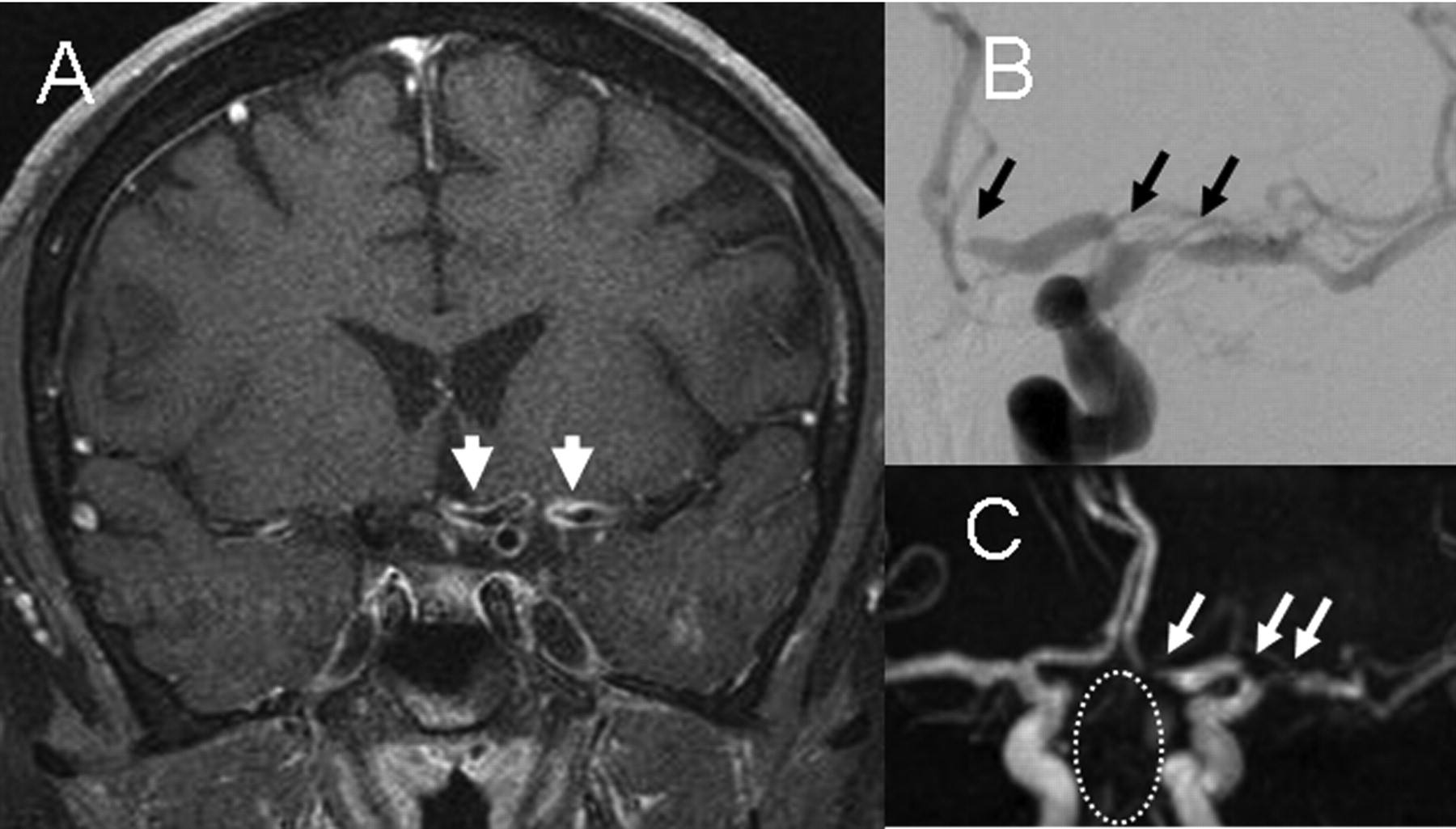
Primary angiitis of the central nervous system: A. Vessel wall contrast enhancement on coronal contrast T1-weighted brain magnetic resonance imaging (MRI; arrowheads). B. MR angiogram; C. conventional angiogram showing stenosis of middle and anterior cerebral arteries (arrows) and basilar artery occlusion (circle).
At last followup, all but 1 patient had had several neurological events (Table 1). The first recurrence occurred within 6 months of followup in 5 of 7 cases. The mean number of flares per patient was 2.5 flares (range 1–6): 3 patients had 2 or 3 flares and 2 had 4 or more (a flare defined as a period of disease activity that could include several neurological events).
DISCUSSION
The first aim of our study was to analyze a cohort of patients suspected of having isolated CNS vasculitis and to describe the spectrum of differential diagnosis of PACNS. We found that 24 of 33 (72%) patients were diagnosed as having another disease, including RCVS in 13, other noninflammatory vascular disorders in 6, malignancy in 4, and infection in 2.
The large predominance of RCVS in our study (39%) confirms that this condition is probably underrecognized, and represents a major diagnostic challenge1,2,18,19. However, this is in contrast with the findings of Duna and Calabrese, who retained this diagnosis in only 6 of 30 cases (20%) referred for a suspicion of PACNS5. This discrepancy may be explained by referral bias.
As expected, the presentation and disease course of RCVS were strikingly different from those of PACNS. Headaches were the main clinical complaint in our 13 RCVS cases, and presented as thunderclap headache in 10 of 13 cases. This finding is in accord with recent prospective and retrospective series of RCVS, which revealed that recurrent thunderclap headaches are a key symptom at the onset of the RCVS14,15. However, thunderclap headache was also seen, albeit infrequently, in 2 patients with other conditions in our series (1 PACNS and 1 infectious meningovasculitis). The most frequent brain imaging abnormality in our series was cSAH, found in 8 of 13 patients (61%). This imaging finding is increasingly recognized as a suggestive feature of RCVS14,15,20,21,22. Of note, it has also been reported occasionally in cerebral amyloid angiopathy, dural sinus, or cortical vein thrombosis and infective endocarditis21,22.
Another aim of our study was to evaluate the specificity of the clinicoradiological presentation of RCVS. For this purpose, we focused on patients with an acute angiographically defined CNS vasculopathy. Our data confirmed the specificity of the clinicoradiological picture of RCVS at onset; i.e., thunderclap headache, the absence of a focal neurological deficit, a low modified Rankin score, cSAH, and/or a normal brain parenchyma on MRI, and “string of beads” appearance on conventional angiography. In the setting of an acute angiographically defined CNS vasculopathy, the positive predictive value of thunderclap headache, normal brain MRI, and cSAH were 82%, 100%, and 100%, respectively. These findings and other recent data14,15 strongly suggest that a diagnosis of RCVS can be highly suspected within the first days after disease onset, long before the reversibility of arterial narrowing, which occurs within 1 to 3 months14,15,16. Only vascular followup imaging can definitively confirm the diagnosis of RCVS14,15,16. However, a prompt recognition of this entity may avoid needless investigations, such as extensive screening for infection, immune-mediated diseases, or malignancy, as well as unwarranted brain biopsy and aggressive treatments15,16.
Expectedly, we found that several common diseases could present diagnostic challenges, such as intracranial atherosclerosis, cryptogenic embolism, infection, and malignancy. Interestingly, 1 patient in our series, who was suspected of having PACNS for several years, had a COL4A1 gene mutation-related genetic vasculopathy, a recently characterized entity23,24. Several cases of similar inherited late-onset CNS vasculopathies, such as CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy), have been misdiagnosed as PACNS25,26,27,28. These observations emphasize the value of family history information and ophthalmologic examination in the evaluation of atypical CNS vasculopathies.
Eventually we identified 8 patients considered to have PACNS, with histological documentation in only 1 case. The most striking feature of this group was the diversity of clinicoradiological presentation and disease course, which suggests that these patients do not have the same disease. In the older literature, PACNS is reported to carry a poor short-term prognosis if left untreated13,29,30,31, in sharp contrast with the indolent course observed in several of our patients. Three of them remained relapse-free after a followup of 2 years or more without treatment. Indeed, some cases of biopsy-proven PACNS with a remitting-relapsing course have been reported29. Further, in 1 series of biopsy-proven PACNS, time from disease onset to diagnosis was as long as 3 years30, whereas in a recent report of 21 European cases of PACNS the time from first presentation to diagnosis could reach 184 months (mean 18 months)32. Accordingly, 1 of our patients who presented with 2 unexplained strokes at the age of 30 years was followed and left untreated for 8 years before he had additional strokes, disclosing multiple intracranial arterial stenoses with contrast enhancement on MRI. This recently reported sign may be of valuable interest for the diagnosis of large-vessel intracranial vasculitis10,11,12.
Our study has several limitations. First, it was retrospective; therefore investigations and followup of patients were not standardized. Hence, several RCVS cases had suboptimal monitoring of vascular imaging, preventing observation of the reversibility of angiographic abnormalities in 30% of cases, as in other recent retrospective studies15,21. However, these patients did not differ from others in terms of presentation, disease course, and longterm outcome. Further, they fulfilled the International Classification of Headache Disorders diagnostic criteria for benign angiopathy of the CNS17.
Second, intracranial vessel-wall imaging (fat and blood signal-suppressed T1-weighted precontrast and postcontrast MRI), first reported in 200811, was not routinely performed at our center during the 2000–2008 period. It was available for only 1 case, where it proved to be extremely useful.
Third, in order to assess the specificity of the clinicoradiological presentation of the RCVS, we compared these cases with a group of 11 patients with heterogeneous underlying diseases. We used these patients as comparators because, like patients with RCVS, they presented to clinicians in a similar manner, i.e., with acute angiographically defined CNS vasculopathy. Of note, the 23 patients included in this analysis accounted for 70% of the overall cohort. A similar approach has been used previously to investigate the operating characteristic of angiography and brain biopsy in suspected PACNS5.
Eventually, only a small number of our patients had undergone a brain biopsy. However, this would have been inappropriate for patients with RCVS and other noninflammatory cerebrovascular disorders. Yet this leaves significant uncertainty regarding the underlying diagnosis of our 6 patients suspected of having PACNS, but lacking histological proof and vessel-wall imaging abnormalities. Indeed, some of them may not have had PACNS. Nevertheless, diagnostic uncertainty is a key issue for the management and study of PACNS, a fact stressed by investigators for decades9,32,33,34 and which is still apparent from recently published case series35,36,37,38. Indeed, in the Mayo Clinic cohort of 101 cases of PACNS reported by Salvarani, et al only 31 cases were proven pathologically37. Similarly, among 21 cases reported by Kraemer and Berlit, only 6 were biopsy-proven38.
Overall, our results emphasize the role of RCVS as a frequent mimic of CNS vasculitis and confirm the suggestive features of its presentation. Clinicians must be aware of this condition in order to facilitate identification of precipitating factors and avoid unneeded investigations and aggressive treatment. Cerebral lymphoma, advanced carcinoma, and infection as well as intracranial atherosclerosis and cryptogenic embolism represented other diagnostic pitfalls. Eventually, the heterogeneity of our patients with PACNS showed that in clinical practice, as well as in scientific investigation, this label remains a frail working diagnosis, unless formal pathological proof has been obtained9,32,33,34. Unfortunately, this is true for only one-third of cases, even in the best-trained hands13,37. Just as the oldest series of patients with PACNS probably included patients with RCVS13, one may speculate that some patients considered as having PACNS actually suffer from different inherited or acquired noninflammatory vasculopathies33. Only multicenter prospective initiatives will clarify the numerous uncertainties surrounding PACNS and help clinicians to manage patients with unexplained CNS vasculopathy.
- Accepted for publication January 26, 2012.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.