
Abstract
Objective. To evaluate the effect of home total parenteral nutrition (HTPN) on the nutritional and functional status of patients with systemic sclerosis (SSc).
Methods. Retrospective review of SSc patients from the HTPN database at the University Health Network, Toronto, Canada, from 1998 to 2010.
Results: In total 12 subjects (9 females, 3 males) with SSc were identified. At initiation of HTPN, the age was 48.75 ± 3.94 years and the median body mass index was 16.8 kg/m2 (range 12.3–21.3). This significantly increased to 18.3 kg/m2 (17.0–21.7) at 6 months and to 19.7 kg/m2 (17.0–24.6) at 12 months. The mean Karnofsky score at baseline was 58.00 ± 3.27, and the score at 12 months of 39.00 ± 13.29 did not change significantly.
Conclusion. HTPN improved the nutritional status of these patients with SSc but it did not improve their functional status.
- HOME PARENTERAL NUTRITION
- SYSTEMIC SCLEROSIS
- SCLERODERMA
- INTESTINAL PSEUDOOBSTRUCTION
- BACTERIAL OVERGROWTH
Systemic sclerosis (SSc) is a progressive, multisystem disorder that has significant morbidity and mortality1. About 50% to 90% of patients have gastrointestinal (GI) involvement, which includes gastroesophageal reflux disease, gastroparesis, intestinal pseudoobstruction, and malabsorption2. A recent study looking at 586 Canadian patients with SSc revealed that 18% were at high risk of malnutrition with significant correlates being disease duration, number of GI complaints, diffuse disease, physician global assessment of disease severity, hemoglobin, oral aperture, abdominal distention, and possible malabsorption3.
There is minimal literature providing guidance on how to manage malnourished patients with SSc and on the effect of home total parenteral nutrition (HTPN) on nutritional characteristics, functional status, and survival in patients with SSc. The aim of our study was to evaluate these outcomes.
MATERIALS AND METHODS
Patients
Charts of University Health Network patients receiving HTPN were reviewed from 1998 to 2010, and 12 subjects with SSc were identified. These subjects were either already receiving HTPN or started HTPN during the study period. For HTPN, patients were assessed by a multidisciplinary nutrition support team consisting of a dietitian, pharmacist, nurse, and physician. The criteria for acceptance into the HTPN program included the inability to maintain a normal nutritional status due to intestinal failure from underlying SSc. This was assessed by the physician who investigated and made the diagnosis of intestinal failure. All patients with SSc had significant GI involvement with gastroesophageal reflux disease, gastroparesis, and intestinal pseudoobstruction.
The nutritional status of all patients was assessed using the Subjective Global Assessment (SGA), which is a well validated tool for screening malnutrition based on features of history and physical examination. Patients were classified as well nourished (SGA-A), moderately malnourished (SGA-B), or severely malnourished (SGA-C)4.
Data collected from the HTPN registry and clinical monitoring include demographics, body mass index (BMI) in kg/m2, hemoglobin values, blood biochemistry, and quality of life (QOL) scores. For blood biochemistry, the following were measured using standard hospital methods: Serum albumin (normal range 38–50 g/l), plasma creatinine (normal range 50–98 μmol/l), alanine aminotransferase (normal range 7–40 U/l), aspartate aminotransferase (normal range 5–34 U/l), and alkaline phosphatase (normal range 40–150 U/l) were measured using the Architect c8000 system (Abbott Laboratories Ltd., Saint-Laurent, Quebec, Canada).
The functional status of patients with SSc taking HTPN was assessed by the Karnofsky score5 in order to measure the level of patient activity and medical care requirements. The Karnofsky performance score ranges from 0 to 100, where 0 indicates a patient is deceased and 100 indicates a patient has normal functioning with no evidence of active disease. The Karnofsky score was measured by the HTPN nurse. Survival rate while taking HTPN was also assessed.
Our study was approved by the Research Ethics Board, University Health Network, Toronto, Ontario, Canada.
Statistical analysis
Data collected from the HTPN registry were entered into a Microsoft Excel (Microsoft Corp., USA) spreadsheet, and subsequently transferred to the statistical program SPSS (Version 16.0; SPSS, Chicago, IL, USA) for analysis. Preliminary exploratory analysis examined the normality of data for the continuous variables. Descriptive statistics are reported as median (range) or percentage of population. Friedman test was done to compare the 3 timepoints for clinical and biochemical data. Where there was a significant difference, Wilcoxon signed-ranks test was done to compare baseline to 6 months and baseline to 12 months. In addition, survival analysis was performed using the Kaplan-Meier method.
RESULTS
In total, 12 patients with scleroderma were enrolled in the HTPN program at our center between 1998 and 2010. Their baseline characteristics are described in Table 1. All the patients in the study had SSc by American College of Rheumatology (ACR) criteria for classification of SSc, and GI involvement. However, patients had varying degrees of severity of SSc. The main indication for HTPN was poor nutritional status as a result of chronic intestinal pseudoobstruction and bacterial overgrowth of the small intestine that did not improve with dietary and pharmacologic interventions such as prokinetics and cyclic antibiotics. The mean age of patients with SSc requiring HTPN was 48.75 ± 3.94 years and the majority of patients were female (9/12). Eleven patients had sclerodactyly, only 1 patient had normal skin, 2 patients had renal involvement, 3 patients had cardiac involvement, and 4 patients had varying degrees of pulmonary involvement.
Baseline demographics.
Caloric intake, as assessed by the TPN dietitian, was poor in all patients despite maximum medical treatment. In some patients enteral nutrition was started, with no success because of their underlying severe intestinal pseudoobstruction (details not available for all patients). In 1 patient, a gastrojejunal tube had been placed, but was subsequently removed because of significant local discomfort related to skin tightness.
Eight patients out of the 12 were underweight with BMI < 18.5 kg/m2. Four patients had normal BMI at baseline. All patients were deemed to be moderately to severely malnourished (SGA-B in 4 patients and SGA-C in 8 patients). Therefore, all SSc patients referred for HTPN met entry criteria, and patients were admitted for HTPN.
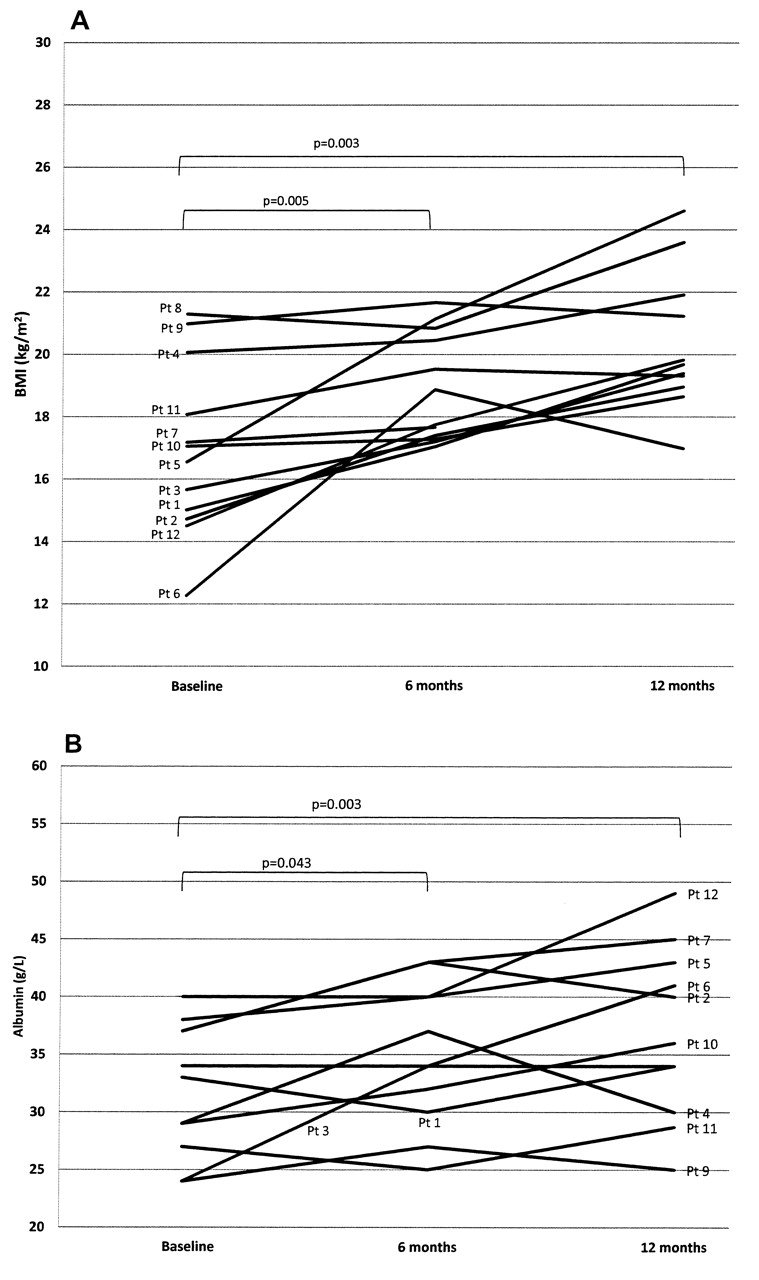
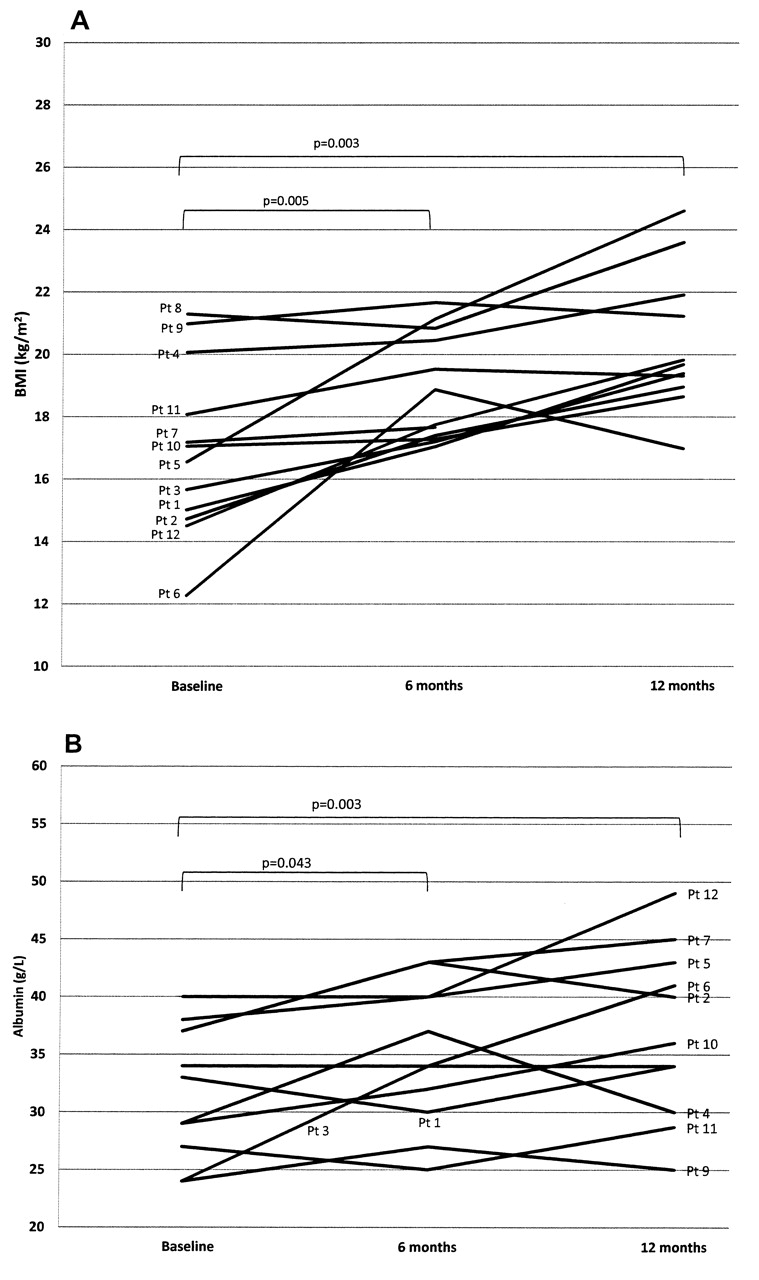
In patients receiving HTPN, weight increased significantly over the period of 12 months (Table 2). Median BMI increased in 6 months on HTPN from 16.8 kg/m2 (range 12.3–21.3) to 18.3 kg/m2 (17.0–21.7) (p < 0.001) and further increased to 19.7 kg/m2 (17.0–24.6) at 12 months (Table 2). At baseline 7/12 (58%) patients had albumin level < 35 g/l. At 6 months, albumin increased from 31 g/l (range 22–40) to 34 g/l (25–43), and further increased to 36 g/l (25–49) at 12 months. Individual BMI and albumin measurements are shown in Figure 1. There was no significant change in liver enzymes and bilirubin. The mean hemoglobin at HTPN initiation was 99.1 g/l (range 80–135).
{kind=link}
Individual measurements in patients with systemic sclerosis receiving home parenteral nutrition. A. Body mass index (BMI); B. albumin.
Nutritional and biochemical values. Values are median (range) unless otherwise indicated.
Mean Karnofsky score at baseline was 58.00 ± 3.27; although there was a decrease in score at 12 months to 39.00 ± 13.29, this did not reach significance (p = 0.222).
Within the first year of HTPN initiation, 1 of 12 patients died from complications related to SSc, 10 patients continued receiving HTPN, and in 1 patient HTPN was tapered and switched to enteral feeding. Within 2 years from HTPN initiation, a total of 5 patients died, all from causes related to SSc and not related to TPN. Therefore, the 2-year survival was 58%. Overall, looking at the entire HTPN duration, including the first 12 months after initiation, HTPN duration ranged between 5 and 270 months. The mean survival while receiving HTPN was 228.8 ± 29.2 months. If we exclude a patient with mild SSc who had pseudoobstruction and survived 270 months on HTPN, the mean survival was 72.6 ± 9.9 months. As fewer than half the subjects had died at the end of 2 years, median survival could not be determined.
DISCUSSION
Results from our study indicate that HTPN improved nutritional status of patients with SSc but did not improve functional status, and observed survival at 2 years was only 58%.
Very few studies have investigated the effects of HTPN on patients with SSc. Ng, et al reported successful HTPN therapy in 15 patients with severe bowel disease related to SSc, including intestinal pseudoobstruction, malabsorption, and malnutrition6. In that study, line complications and survival were reported. With 15,700 catheter-use days there were only 2 episodes of septicemia and 2 episodes of superior vena cava obstruction. The authors reported improved QOL, but a specific QOL assessment tool was not described. Seven patients died, likely from SSc complications unrelated to GI disease or parenteral nutrition. Brown, et al confirmed the longterm safety of HTPN for SSc-related intestinal failure; however, in that study, the effect on nutritional characteristics and QOL was not examined7. In our study, we did not record HTPN-related complications such as line infection as this was not well recorded in patients’ charts.
Measurements of nutritional status in patients with SSc can be challenging due to the effect of the underlying disease on anthropometric characteristics based on skin elasticity (skin-fold measurements), or plasma proteins that can be affected by renal function. In our patients, we found significant gain in BMI despite the small sample size. Although SGA was performed at baseline, repeated assessments were not recorded in patients’ charts.
Regarding albumin, a significant increase was seen on HTPN, suggesting improvement in nutritional status. Although this was small and did not normalize, this increase was likely a reflection of improved nutrition, since these patients were clinically stable and also presented concomitant weight gain while receiving HTPN. Albumin has its limitation as a nutritional marker because it may be affected by factors such as infection, liver synthetic dysfunction, and renal losses of protein. Recently, research from the Canadian Scleroderma Research Group stated that albumin was not a useful marker for malnutrition in SSc patients8.
In our study, we did not see a significant effect of HTPN on functional status of SSc patients as assessed by the Karnofsky scoring system. We should note that this score has never been validated in SSc. Also, it is possible that HTPN in these patients may have improved other QOL aspects not assessed by the Karnofsky score.
Our observed 2-year survival rate was 58%. For those who died, the primary cause of death was not TPN-related but reported to be SSc-related by their primary physicians. Since these patients died at different hospital centers scattered throughout the Province of Ontario, it was not possible to get specific information related to their deaths. In some of our patients, the disease progressed rapidly and involved multiple organs, resulting in death secondary to pulmonary, cardiac, or renal failure. In other patients, although SSc disease may have involved various organs, it remained relatively stable for long periods of time. One patient with SSc had cardiac involvement and pulmonary hypertension and died within 1 year of HTPN initiation, with the other 4 dying in the second year of HTPN. On the other hand, another patient with SSc with the longest survival on HTPN (270 months) had no significant organ involvement except for GI involvement.
In patients with SSc, there is a disparity in the number of years lived. Our results are close to those of Amiot, et al, who reported a 2-year survival rate of 37% in adults with SSc and chronic intestinal pseudoobstruction receiving HTPN9. A study conducted in 264 patients with diffuse cutaneous SSc from the Scleroderma Criteria Cooperative Study from 1973 to 1977 showed that renal, cardiac, pulmonary, and GI involvement in SSc predicted reduced survival10. The poorest prospects for survival were patients < 64 years of age with a hemoglobin level < 11 g/dl, and in those > 64 years old with a blood urea nitrogen level > 16 mg/dl. In a more recent study in 309 French Canadians, Cox regression revealed that independent predictors of mortality were skin involvement of the trunk, age, carbon monoxide diffusion capacity of the lungs ≤ 70% of normal value, erythrocyte sedimentation rate ≥ 25 mm/h, and hemoglobin level ≤ 125 g/dl11. All but 1 patient in our population had hemoglobin values ≤ 125 g/dl at HTPN initiation (mean 99.1 g/l).
Although we did not compare SSc patients receiving to those not receiving HTPN, our study may support findings by Grabowski and Grant that adequate nutritional support does not alter the natural history of systemic scleroderma12. However, HTPN may help avoid progressive debilitation due to nutritional depletion.
There are limitations to our study. Although the data from the HTPN registry were collected prospectively, these results are based on a retrospective review of the HTPN registry along with patients’ charts. In addition, the number of patients was small because very few patients with SSc are referred to the HTPN program. It is not clear whether this is due to the rarity of significant malnutrition or to the fact that malnutrition is underrecognized. Considering that 18% of SSc patients are reported to be at high risk of malnutrition, it is possible that nutrition support (enteral or parenteral) is underprescribed. Longterm complications from HTPN such as cholestasis, osteoporosis, and frequency of line infections were not assessed. Also, not all independent predictors of mortality were examined because of the retrospective design of this study and the small number of patients.
The use of HTPN was beneficial in improving the nutritional status of patients with SSc but did not improve performance status, and patients’ survival remained low.
Acknowledgment
The authors gratefully acknowledge Lydia Fairholm, RD; Millie Yeung, MScPhm; Mary Baun, BScPhm, from the Home Total Parenteral Nutrition Team, Toronto General Hospital, Toronto, Canada.
- Accepted for publication December 20, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.