

Abstract
Objective. To examine the association between magnetic resonance imaging (MRI) features of distal phalanx (DP) disease and the progression of nail pathology in psoriatic arthritis (PsA).
Methods. Clinical nail assessment and hand MRI scans were done on 34 patients with PsA. Twenty patients had repeat nail assessments after 1 year.
Results. Nails with onycholysis and hyperkeratosis at baseline were more likely to have corresponding DP bone erosion and proliferation on MRI. DP bone edema on baseline MRI was associated with development of onycholysis and hyperkeratosis in corresponding nails.
Conclusion. Our data suggest that DP inflammation is central in the development of psoriatic nail disease.
Nail disease is a common feature of psoriatic arthritis (PsA)1. Cross-sectional magnetic resonance imaging (MRI) studies have shown that nail involvement detected by MRI is present in most patients with PsA, and that MRI nail disease is strongly associated with abnormalities in the corresponding distal phalanx (DP) and associated structures2,3. Our aim was to compare the clinical subtypes of psoriatic nail disease with MRI scanning of the DP, and to determine the role of DP disease in development of psoriatic nail disease.
MATERIALS AND METHODS
With ethical approval and informed consent, 34 patients with PsA were recruited from rheumatology clinics in the Auckland, Rotorua, and Wellington regions of New Zealand. All patients met the Classification for Psoriatic Arthritis criteria for PsA4. At baseline, all patients had a comprehensive clinical assessment including the psoriatic nail severity score (PNSS), which records the presence of nail pitting, onycholysis, hyperkeratosis, and dystrophy at each nail5. Twenty patients returned for repeat nail assessment after 12 months. All nail assessments were completed by a single investigator (KP) who was blinded to the MRI results.
MRI scans of the dominant wrist and fingers were obtained in all patients at baseline using a Siemens Magnetom Avanto 1.5-Tesla (T) scanner, with dedicated wrist coil. Sequences and acquisitions have been reported6. The presence of bone marrow edema (BME), bone erosion, and proliferation at the second to fifth DP was recorded by a musculoskeletal radiologist (AD) who was blinded to the clinical nail assessment scores.
Data were analyzed using GraphPad Prism (GraphPad Software, San Diego, CA, USA). Descriptive data are presented as number (percentage) or median (range). Data comparing nail disease in the dominant hand index, middle, ring, and little fingers and MRI pathologies at the dominant hand second to fifth DP were analyzed on a site-by-site basis using chi-squared analysis.
RESULTS
In the total group, 21/34 (62%) were male, 28 (82%) were of European ancestry, and 24 (71%) were taking traditional oral disease-modifying antirheumatic drugs (DMARD). All patients had a history of psoriasis. The median age was 50 years (range 26–68), arthritis duration 10 years (range 0.5–35), psoriasis duration 18 years (range 0.5–50), Psoriasis Area and Severity Index 1.7 (range 0–12), and 28-joint Disease Activity Score with C-reactive protein 3.98 (range 1.42–6.57). There were no differences in clinical characteristics between the baseline group and those who returned for followup visits. No patient received biologic DMARD during the study period.
At baseline, 129 digits were assessed. Seven DP could not be assessed by MRI because of signal dropout, metal artefact, or severe deformity. There were 21 (16.3%) nails with pits, 24 (18.6%) nails with onycholysis, 9 (7.0%) nails with hyperkeratosis, and 2 (1.6%) with dystrophy. There were 40 nails (31.0%) with at least 1 of these 4 abnormalities. As nail dystrophy was so infrequent, this feature was not included in further analysis. On MRI at baseline, there were 18 DP (14.0%) with BME, 23 DP (17.8%) with bone erosion, and 17 DP (13.1%) with bone proliferation. At baseline, nail pitting was not associated with MRI changes in the DP. However, nails affected by onycholysis and hyperkeratosis were more likely to have corresponding DP bone erosion and proliferation on MRI (Table 1, Figure 1).

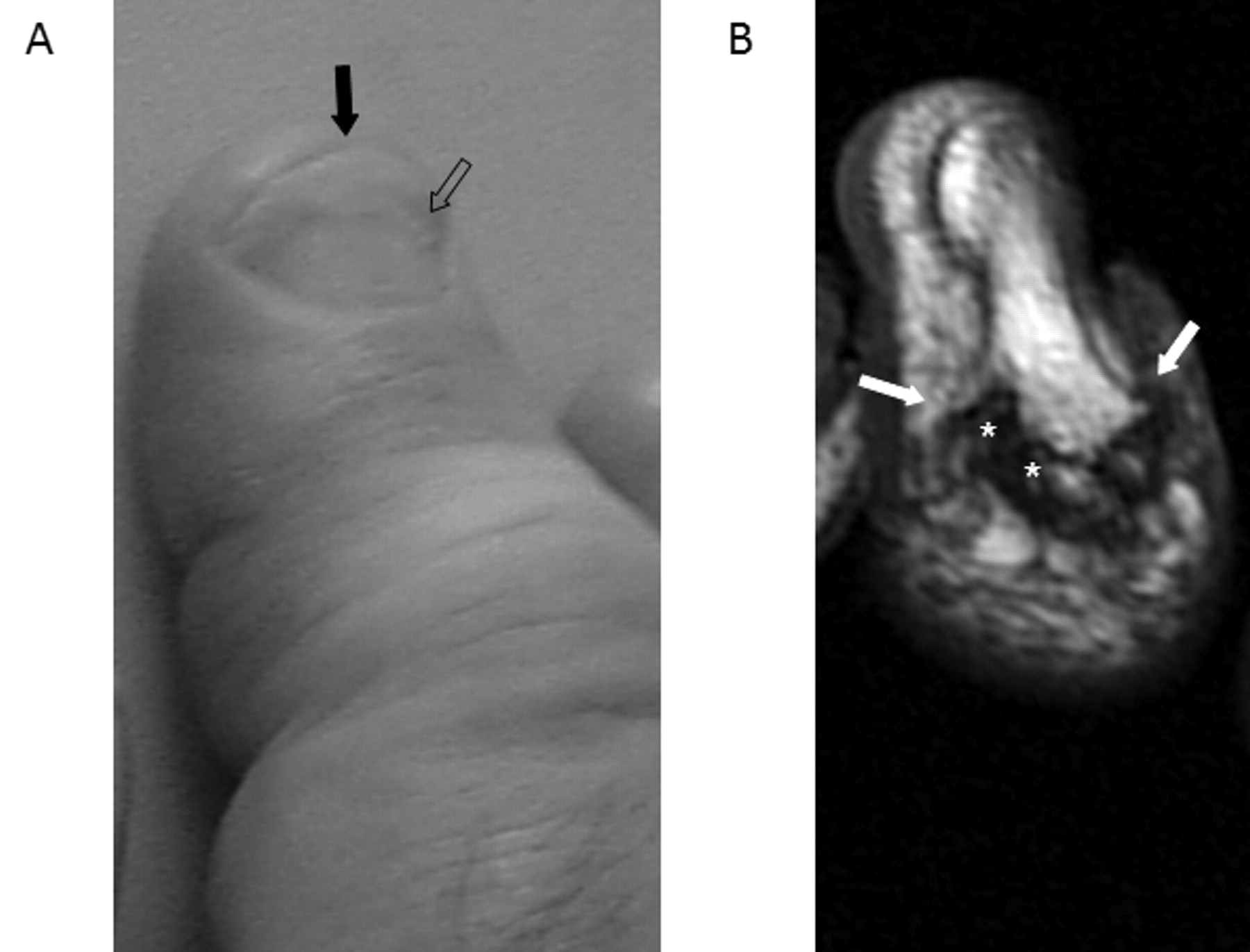
A. The nail of the right middle finger in a patient with psoriatic arthritis showing onycholysis (solid arrow) and hyperkeratosis (open arrow). B. Corresponding right middle finger distal phalanx from the same patient on T1-weighted coronal magnetic resonance imaging scan showing bone erosion (asterisks) and proliferation (arrow).
Site-by-site analysis of psoriatic nail lesions and distal phalanx disease detected by magnetic resonance imaging (MRI) at baseline (n = 129 nails).
Followup assessment of 80 fingernails at 1 year showed 13 (16%) with pits, 20 (25%) with onycholysis, 8 (10%) with hyperkeratosis, and 2 (3%) with dystrophy. There were 29 nails (36%) with at least 1 abnormality. Of the 67 nails without pits at baseline, 10 (15%) developed pits; of the 61 nails without onycholysis at baseline, 4 (7%) developed onycholysis; and of the 72 nails without hyperkeratosis at baseline, 4 (6%) developed hyperkeratosis. There was no relationship between development of nail pitting and corresponding DP disease on baseline MRI. However, nails that developed onycholysis were more likely to have corresponding DP BME on baseline MRI, compared with nails that did not develop onycholysis (50% vs 11%; p = 0.03). Similarly, nails that developed hyperkeratosis were more likely to have corresponding DP BME and erosion on baseline MRI compared with nails that did not develop hyperkeratosis (for BME 75% vs 10%; p = 0.0003; and for erosion 75% vs 18%; p = 0.006).
DISCUSSION
Consistent with previous cross-sectional studies2,3, our study demonstrated a relationship between DP bone disease and psoriatic nail disease in patients with PsA. Further, certain features of psoriatic nail disease, onycholysis and hyperkeratosis, were strongly associated with DP disease in both cross-sectional and longitudinal analysis. The contrasting lack of relationship between nail pitting and DP disease may reflect the pathogenesis of nail pitting, which arises due to defects in the uppermost part of the nail plate7. Although DP BME was not associated with nail disease in the baseline cross-sectional analysis, this feature was associated with development of hyperkeratosis and onycholysis in the corresponding nail. BME is strongly associated with bone erosion in patients with erosive PsA6, and biologic therapies that target BME and prevent erosion in PsA also prevent nail disease8,9,10. Intervention studies specifically addressing the relationship between response to these therapies at the DP and corresponding nail may provide further evidence supporting this relationship.
We acknowledge the limitations of our study. Despite the lack of clinical differences, it is possible that the changes observed over time in the followup group may have been different than those in the group who did not return. Patients had longstanding disease, and findings may have been different in an early disease cohort. The frequency of nail disease was low compared to other studies1,11; it is likely that not all nail disease was identified as only certain features are assessed using the PNSS. Common features such as discoloration and ridging are not recorded using this scoring system. However, this system allowed us to standardize the measurement using a single observer, who was blinded to the MRI scores.
Our data provide further evidence of the close relationship between adjacent bone and nail disease in PsA, and support the hypothesis that inflammation at the DP is central in the development of psoriatic nail disease.
Footnotes
-
Supported by the Auckland Medical Research Foundation, the Auckland Regional Rheumatology Research Trust, and the QE Hospital Community Trust; and by an investigator-initiated grant from Novartis.
- Accepted for publication November 29, 2011.








{kind=link}