

Abstract
Objective. Etanercept, a fully human tumor necrosis factor soluble receptor, is effective in treatment of ankylosing spondylitis (AS). Current guidelines suggest sulfasalazine (SSZ) treatment as initial therapy for the management of patients with AS with peripheral arthritis versus therapy with biologics. We compared the efficacy of etanercept with SSZ in patients with AS with peripheral joint involvement.
Methods. The efficacy of etanercept 50 mg once weekly was compared with that of SSZ up to 3 g daily in subjects with ≥ 1 swollen peripheral joint at baseline, using data from a 16-week randomized double-blind study in subjects with AS. Efficacy was assessed by the Assessment in AS criteria and the Bath AS Disease Activity, Functional, and Metrology indices. The last observation carried forward method was used for imputation of missing values.
Results. Of 566 subjects included in original study, 181 (etanercept 121; SSZ 60) had ≥ 1 swollen peripheral joint and 364 (etanercept 250; SSZ 124) had none at baseline. AS patients treated with etanercept showed significantly greater improvement than those treated with SSZ in all joint assessments regardless of swollen joint involvement.
Conclusion. In this analysis, etanercept was significantly more effective than SSZ for management of patients with AS and peripheral joint involvement.
- ANKYLOSING SPONDYLITIS
- ETANERCEPT
- SULFASALAZINE
- DISEASE MANAGEMENT
- TUMOR NECROSIS FACTOR-α
- DISEASE-MODIFYING ANTIRHEUMATIC DRUGS
Ankylosing spondylitis (AS) is a chronic rheumatic disease that affects spine and peripheral joints, resulting in inflammatory back pain and often progressing to structural and functional impairment and reduced quality of life1,2,3,4. Therapies recommended for the management of AS include nonsteroidal antiinflammatory drugs, disease-modifying antirheumatic drugs such as sulfasalazine (SSZ), and anti-tumor necrosis factor (TNF) agents, such as etanercept5. Etanercept, a fully human TNF receptor, is an established therapy for AS6,7,8,9,10. SSZ, although not approved for AS in countries participating in this study, is the recommended treatment for AS with peripheral arthritis before use of anti-TNF agents5.
In the first trial to directly compare the efficacy and safety of TNF blocker versus conventional therapy, ASCEND (Ankylosing Spondylitis Study Comparing ENbrel with Sulfasalazine Dosed Weekly), etanercept was significantly more effective than SSZ in improving the signs and symptoms of AS11. We report on an analysis of the ASCEND data, in which the efficacy of etanercept and SSZ was assessed in subjects with and without peripheral joint involvement.
MATERIALS AND METHODS
Study design and subjects
The ASCEND study (NCT00247962) was a randomized, double-blind, active-comparator study conducted across 85 sites in 24 countries in Europe, Asia, Latin America, South America, and the Middle East that evaluated the efficacy and safety of etanercept compared to SSZ in subjects with active AS11. Subjects received either etanercept (50 mg once weekly) subcutaneously or SSZ (up to 3 g daily) orally. Treatment was blinded by treating all subjects with visually identical injections and tablets. For this subanalysis, each treatment group was subdivided by baseline joint involvement: subjects with 1 or more swollen joints versus subjects with no swollen joints. A detailed description of patient inclusion/exclusion criteria is provided in the previous report of clinical findings11.
Assessments and statistical analysis
Efficacy endpoints included in this subanalysis were the proportion of responders who had a 20% improvement in Assessments in Ankylosing Spondylitis (ASAS) and ASAS 5/612; improvement in Bath AS Disease Activity Index (BASDAI); partial remission (values < 2 on a 0–10 point scale in each of the 4 ASAS20 domains)13; Bath AS Metrology Index (BASMI)14; and Bath AS Functional Index (BASFI)15.
Efficacy analyses were conducted on the modified intent-to-treat population, and endpoints were analyzed by analysis of covariance, with baseline as covariate. The last observation carried forward method was used for imputation of missing values.
RESULTS
Of a total of 566 subjects enrolled in the ASCEND study11, 181 (etanercept 121; SSZ 60) had ≥ 1 swollen peripheral joint; 374 (etanercept 250; SSZ 124) had none at baseline (11 had no baseline assessment of swollen joints and were not included in the analysis). Baseline demographic and disease characteristics are presented in Table 1.
Baseline demographic and disease characteristics.
In each treatment group, improvements were similar in subjects with and those without baseline swollen joints (p not significant) except for proportions of ASAS20 responders (p = 0.021), with significantly greater improvement shown in those receiving etanercept than those receiving SSZ in all efficacy assessments (Figures 1 and 2).

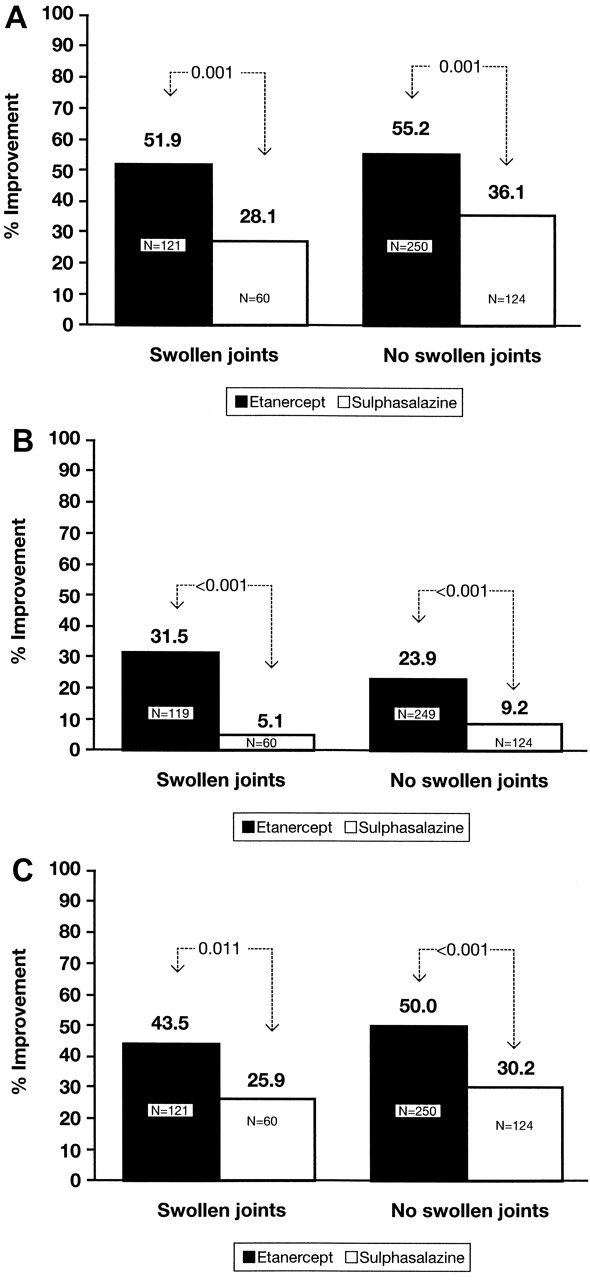
Percentage of subjects with improvement in disease activity by Assessment in Ankylosing Spondylitis (ASAS) criteria at Week 16. A. ASAS20; B. ASAS 5/6; C. partial remission.
Mean percentage improvement in disease activity by Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), spinal mobility, and physical function. A. BASDAI; B. Bath Ankylosing Spondylitis Metrology Index; C. Bath Ankylosing Spondylitis Functional Index.
In subjects with swollen joints at baseline, the number of affected joints decreased from 3.42 (95% CI 2.64, 4.20) at baseline to 1.33 (95% CI 0.82, 1.85; p < 0.001) at Week 16 with etanercept and from 3.52 (95% CI 2.73, 4.30) to 2.82 (95% CI 0.98, 4.66; p = 0.430) with SSZ. It was noted in a posthoc nonparametric test, Wilcoxon signed-rank test of change = 0, that the total number of swollen joints at baseline was significantly different from that at Week 16 for both etanercept and SSZ (p < 0.001). Nevertheless, improvement from baseline for those with swollen joints was significantly greater with etanercept (61.11%) than with SSZ (19.89%; p = 0.037).
At Week 16, etanercept resulted in a significantly higher proportion of ASAS20 responders than SSZ in those with swollen joints at baseline (68.6% vs 50.0%; p = 0.020). Similar results were seen in those without swollen joints at baseline (79.1% vs 54.8%; p < 0.001; Figure 1A). Twice as many subjects receiving etanercept achieved an ASAS 5/6 response compared to those receiving SSZ at Week 16 (Figure 1B).
The proportion of subjects receiving etanercept who were in partial remission was significantly greater than the portion of those receiving SSZ (p < 0.01; Figure 1C) at Week 16: 34.7% versus 15.0% (p = 0.006) for subjects with swollen joints at baseline and 32.8% and 15.3% (p < 0.001) for subjects with no swollen joints at baseline. The number needed to treat calculated from these results was 5.1 and 5.7 for patients with and without swollen joints, respectively, indicating that for every 5 subjects with swollen joints and for every 6 subjects without swollen joints treated with etanercept, 1 additional subject would be in partial remission.
As with the disease activity assessments, subjects receiving etanercept showed significantly greater improvement in spinal mobility (BASMI) and physical function (BASFI) than those receiving SSZ at Week 16 (Figures 2B, 2C). At 16 weeks, the effect of treatment with etanercept versus SSZ on BASDAI, BASFI, and BASMI was significant in subjects both with and without swollen joints at baseline (Figure 2A, 2B, 2C). For subjects with no swollen joints at baseline, the treatment effects were 11.20 (95% CI 7.04, 15.35; p < 0.001), 11.10 (95% CI 6.84, 15.37; p < 0.001), and 0.55 (95% CI 0.28, 0.82; p < 0.001), respectively. For subjects with swollen joints at baseline, the effects were 13.99 (95% CI 5.97, 22.01; p < 0.001), 9.80 (95% CI 2.27, 17.33; p = 0.011), and 0.84 (95% CI 0.35, 1.32; p < 0.001), respectively.
DISCUSSION
In our analysis, etanercept was significantly more effective than SSZ in improving both the signs and symptoms of AS in subjects regardless of baseline swollen joints. Although the total number of affected joints decreased over 16 weeks in both treatment groups, the number of swollen joints improved from baseline by 20% with SSZ treatment versus 61% with etanercept (p = 0.037). Twice as many subjects receiving etanercept (regardless of swollen joints) were considered ASAS 5/6 responders compared to those receiving SSZ. More than 30% of subjects receiving etanercept achieved partial remission by Week 16 versus 15% of subjects receiving SSZ.
Etanercept was significantly more effective than SSZ in improving the clinical symptoms of AS in subjects without and more notably with swollen joints at baseline. These findings support the role of etanercept as a key therapy for the management of subjects with AS regardless of peripheral joint involvement.
Acknowledgment
Medical writing support for this report was provided by Ruth Pereira, PhD, of the External Medical Communications Department of Pfizer Inc. and Stephanie Eide of UBC Scientific Solutions. Conduct and monitoring of the study was provided by Carole L. Wishneski, RN, MS, MBA, of Pfizer Inc.
Footnotes
-
Supported by Wyeth, which was acquired by Pfizer Inc. in October 2009. J. Braun has received honoraria for talks and advisory boards and grants for studies from Centocor, Amgen, Abbott, Roche, BMS, Novartis, Pfizer, and MSD. C. Ramos-Remus has received advisory fees from Abbott, Pfizer, and Roche and compensation to conduct clinical trials from Pfizer, Roche, and Merck-Serono. K. Pavelka has received honoraria for lectures from Pfizer, MSD, Roche, and Abbott. B. Freundlich is a former employee of Wyeth.
- Accepted for publication October 5, 2011.








{kind=link}
{kind=link}