

Abstract
Objective. Inflammatory back pain (IBP) is an important feature of axial spondyloarthritis (SpA) that is poorly recognized in primary care, perhaps delaying diagnosis of SpA. We aimed to develop and validate a self-report questionnaire using important domains reported by patients with IBP.
Methods. We developed a 6-item questionnaire assessing spinal/hip stiffness, nocturnal pain, diurnal variation, effects of exercise/rest, and peripheral joint pain/swelling. This was compared with the Calin questionnaire and the domains comprising the Assessment of Spondyloarthritis International Society (ASAS) criteria for IBP in 220 patients with established axial SpA and 66 patients with mechanical back pain followed in tertiary care rheumatology clinics. The classification utility of each item was evaluated using sensitivity, specificity, and likelihood ratio (LR). Multivariable logistic regression was used to analyze different combinations of items to develop candidate scoring systems.
Results. The single item “diurnal variation” had the highest combination of sensitivity (49%) and specificity (92%) for IBP (positive LR 5.95, 95% CI 2.54–13.94), outperforming the Calin and ASAS IBP criteria, which had sensitivities of 83% and 59%, specificities 42% and 66%, positive LR 1.42 and 1.72, negative LR 0.41 and 0.62, respectively. Classification utility of this item was even higher in SpA patients with disease duration < 6 years (sensitivity 48%, specificity 96%, positive LR 12, negative LR 0.54). The other 5 items did not improve classification utility in any combination.
Conclusion. Assessment of a single self-reported item, “diurnal variation,” had substantial classification utility for IBP. This domain is not addressed in existing criteria for IBP, indicating a potentially important omission.
- INFLAMMATORY BACK PAIN
- SPONDYLOARTHRITIS
- CALIN CRITERIA
- DIURNAL VARIATION
- ASAS INFLAMMATORY BACK PAIN CRITERIA
- CLASSIFICATION UTILITY
Inflammatory back pain (IBP) is one feature of ankylosing spondylitis (AS) that is incorporated into the modified New York classification criteria1 and more recently the Assessment of Spondyloarthritis International Society (ASAS) classification criteria for axial SpA2. There are no widely accepted diagnostic criteria for AS and so the classification criteria are often used for the purpose of diagnosis. However, diagnostic delay in AS is problematic because symptoms often predate diagnosis by 8 to 11 years3,4,5. Given that the symptom severity in these patients is comparable to those with established disease and that the benefit of tumor necrosis factor inhibition in these patients is well recognized6, this delay is no longer acceptable7,8,9,10.
A lack of recognition of IBP among primary care physicians likely contributes to this delay in IBP diagnosis and subsequent referral to rheumatology11. A recent postal survey of general practitioners suggested great variability in understanding the features of IBP and indicated a need for continuing education12. However, SpA is found in only 3%–5% of patients presenting with lower back pain in primary care, so few of these physicians will attain sufficient experience to diagnose IBP with confidence11. Recognition of IBP may be facilitated by the development of screening strategies that include self-report questionnaires12,13. Improved IBP screening would help both primary care physicians and rheumatologists identify patients who may have SpA and expedite their formal assessment.
Until 2009, only 2 screening criteria for IBP existed, the Calin criteria14 and the more recent Berlin criteria15. The Calin criteria were developed in 1977 and have been incorporated to some extent into the European Spondylarthropathy Study Group (ESSG)16, the modified New York criteria for AS1, and the Amor criteria for SpA17. The Calin criteria, based on nonstandardized questions administered by the interviewing clinician that were felt to be important in the clinical history for IBP, have been studied in various populations, but the same high sensitivity (95%) and specificity (76%) of the original study has not been reproduced1,18,19. The Berlin criteria were derived from an exploratory study that assessed 101 patients with AS and 112 control patients with mechanical back pain through face-to-face interviews by the same examiner15. When 3 out of 4 IBP measures were positive (“morning stiffness,” “improvement of back pain with exercise and not rest,” “nocturnal pain,” and “alternating buttock pain”), sensitivity and specificity were 33.6% and 97.3%, respectively, with a positive likelihood ratio (LR) of 12.415. Limitations of the Berlin criteria include difficulties and variation in interpretation of the wording in specific domains, such as “alternating buttock pain,” lack of standardization of the wording to the questions, and the use of an established cohort of patients with AS and mechanical back pain controls15.
In 2009, the ASAS IBP criteria were reported and these were based on the expert judgment of the rheumatologist as the “gold standard” for diagnosing IBP in 20 patients with chronic back pain of unknown origin20. These new candidate IBP criteria administered by the interviewing clinician included the domains “improvement with exercise,” “nocturnal pain,” “age at onset < 40 years,” and “no improvement with rest.” They were then validated in a distinct cohort of 648 patients presenting to the rheumatologist with new-onset back pain, and were shown to have a sensitivity of 79.6% and specificity of 72.4%20. Limitations of the ASAS IBP criteria include the lack of standardization of the questions, so that elicitation and affirmation of IBP items is dependent on the expertise of the interviewer. As stated, this expertise is typically lacking among primary care physicians. Concerns have also been raised regarding the omission of morning stiffness due to a lack of statistical significance, even though this represents a concept considered fundamental to the recognition of IBP21. The aim of our study was to use expert consensus to develop and then pilot a standardized set of patient self-reported questions that address domains considered relevant to a diagnosis of IBP and which could be employed in primary care to identify patients who require further assessment for SpA.
MATERIALS AND METHODS
Development of survey questions
Three rheumatologists at the University of Alberta (A.S. Russell, W.P. Maksymowych, S.O. Keeling) reviewed the literature and the existing criteria for IBP in general to identify content domains considered relevant to the diagnosis of IBP. At the time of survey development and data collection, the Berlin and ASAS IBP criteria were unpublished. The 3 rheumatologists reviewed the Calin criteria independently and then as a group. At both stages, each individual Calin question item was scrutinized (Figure 1) to determine to what degree the question item addressed the domains of interest, which domains were not addressed, and the optimal formulation of the wording of questions addressing each domain in the context of the extensive clinical background of the investigators in managing patients with SpA. This resulted in a 6-item questionnaire.
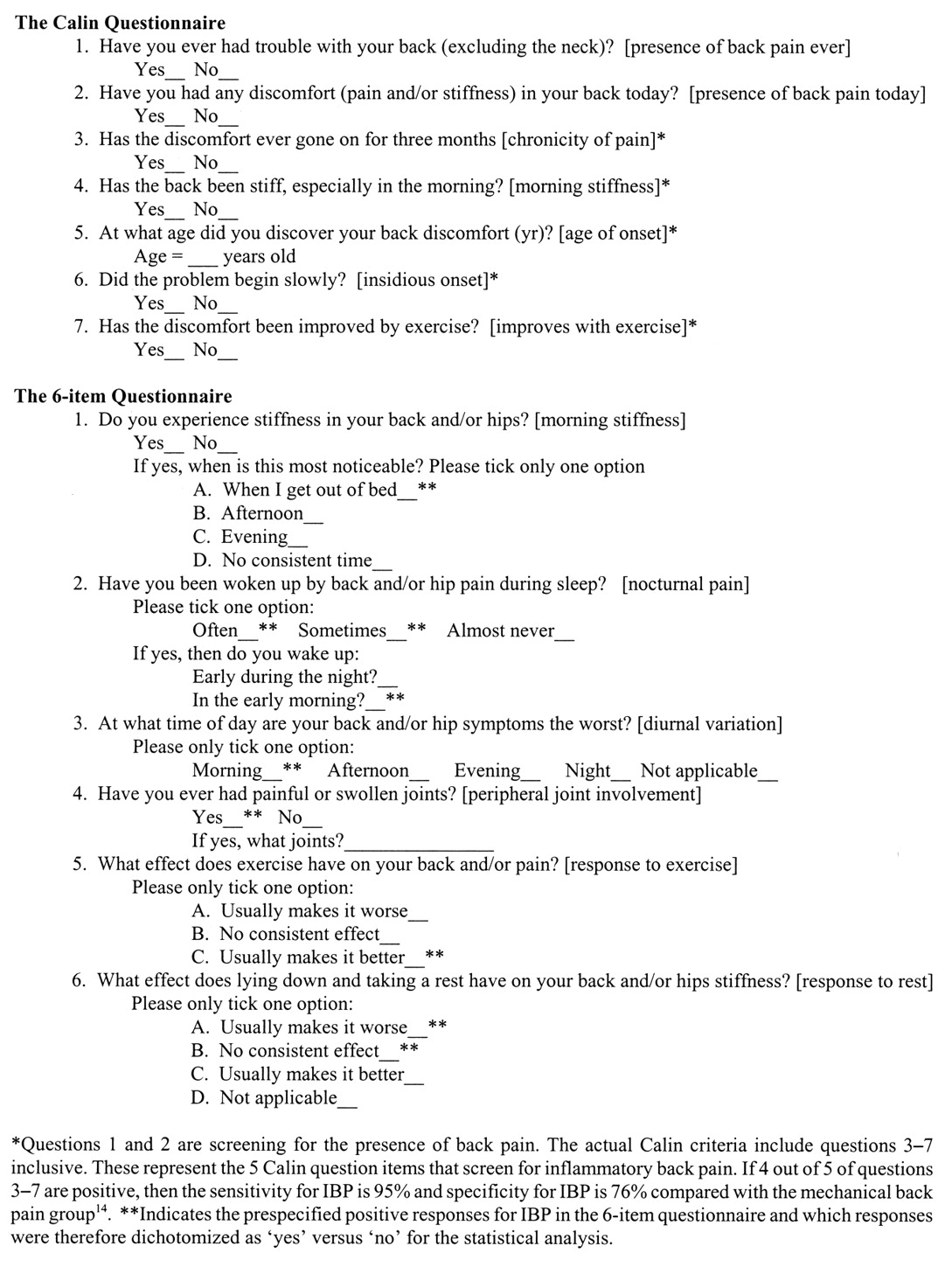
The Calin questionnaire and the 6-item questionnaire with [associated domains].
To confirm that the 6-item questionnaire did not reflect a particular site bias for the assessment of IBP, the questionnaire was sent to 11 members of the Spondyloarthritis Research Consortium of Canada (SPARCC), and this panel of national experts reviewed each item on a 10-point scale and ranked its importance in the diagnosis of IBP. The questionnaire was further scrutinized for feasibility and comprehension by patient members of the Canadian Spondylitis Association. All the questions/domains were considered appropriate.
Candidate items
The important domains for IBP identified by expert consensus included (1) morning stiffness, (2) age at onset of back and/or hip pain, (3) nocturnal pain, (4) diurnal variation in symptoms, (5) peripheral joint pain and swelling, (6) response to exercise, (7) response to rest, and (8) response to exercise and rest. The Calin and 6-item self-report questionnaires did not include exactly the same domains (Figure 1). Additional domains included in the 6-item questionnaire but not the Calin criteria included (1) nocturnal pain, (2) diurnal variation, (3) peripheral joint pain and swelling, and (4) response to rest.
Face validity and pilot testing in an established back pain cohort
Thirteen rheumatologists (7 at the University of Alberta, including 3 who derived the 6-item questionnaire, 6 community rheumatologists in the city of Edmonton) administered the Calin and 6-item questionnaire to consecutive patients with an established cause of back pain, using the rheumatologist’s assessment and diagnosis as the gold standard. While the 3 rheumatologists who derived the 6-item questionnaire included their own patients in the study, 48% (n = 136) of patients were contributed by other rheumatologists. The SpA diagnoses for the patients with IBP by the rheumatologists were not based formally on either the ASAS axial SpA criteria2 or ESSG criteria16 but constituted their expert opinion. The limitations of the ESSG criteria have been cited2, while the ASAS criteria were not published at the time the study was designed. Any patient with back pain of known cause was included if they were 18 years of age or older, spoke English, and agreed to participate in the study. Rheumatologists categorized the patient as “mechanical back pain (MBP)” or “inflammatory back pain (IBP)” and included the specific diagnosis (when available) and duration of back pain symptoms. The questionnaires were administered in random order to address possible order effects. All patients provided written informed consent and the study was approved by the Health Ethics Research Board of the University of Alberta (Edmonton, Alberta, Canada).
Data analysis
Baseline characteristics of the mechanical and inflammatory back pain cohort were compared with chi-square, Mann Whitney U, or Student t tests as appropriate. The responses to the Calin items are dichotomous (yes/no) whereas our 6-item questionnaire included a combination of dichotomous responses (yes or no) and multiple choice answers. We prespecified which responses for each individual item would be considered indicative of IBP in the 6-item questionnaire prior to the data analysis, due to the potential combinations of dichotomous and multiple choice answers (Figure 1). The affirmative response reflected the consensus of the expert panel of what represented IBP versus MBP for each individual item. Positive and negative LR, sensitivities, and specificities were calculated for all items, and analyses were repeated stratifying patients by age, sex, and symptom duration. For the latter, symptom duration was divided into tertiles of the cumulative distribution (< 6 years, 6–18 years, > 18 years).
Multivariate logistic regression analysis of all statistically significant items (p < 0.05) from univariate analyses of the Calin and 6-item questionnaire, respectively, was performed with the diagnosis of IBP as the dependent variable. A second analysis using stepwise forward logistic regression was performed to explore various combinations of individual items. We then undertook 2 possible analytic approaches that might form the basis for an IBP screening tool. In one approach, each question item that was significant by regression analysis received a score of 1, and scores were summed (additive tool). In a second approach, beta-coefficients for significant items by logistic regression were used to derive weights for the contribution of that item to the total score (weighted tool). With both the additive and weighted tools, all domains to which the patient answered affirmatively for IBP received a value of 1, and were entered into the formula. Therefore, when patients responded to “diurnal variation” (At what time of day are your back and/or hip symptoms the worst?) as “morning,” or to “response to exercise” (What effect does exercise have on your back and/or pain?) as “usually makes it better,” or to “response to rest” (What effect does lying down and taking a rest have on your back and/or hip stiffness?) as “usually makes it worse,” they received a value of 1 per domain. Any of the other possible responses per domain (question item) would therefore be negative for IBP and receive a score of 0. The final score reflected the sum total (additive score range = 0–3; weighted score = 0.6 × diurnal variation + 0.24 × response to exercise + 0.16 × response to rest, range 0–1). Receiver operating characteristic (ROC) analysis to calculate the area under the curve (AUC) as well as the balance between sensitivity, specificity, and likelihood ratios were used to provide optimal cutoffs for each tool in screening for IBP. These cutoffs were then used to compare sensitivity, specificity, and likelihood ratios for IBP with the Calin criteria and individual items from the 6-item questionnaire. In general, AUC ≤ 0.5 is likened to chance, 0.6–0.7 of slight clinical value, 0.7–0.8 of modest clinical value, and > 0.8 considered clinically very useful22. Subgroup analyses were performed to determine classification utility according to sex, age, and symptom duration, evaluating the performance of the questionnaires for early disease populations (age < 40 years, symptom duration < 6 years, male). Chi-square analysis was used to assess for a statistical difference between the AUC for the Calin and respective candidate tools.
We also conducted a posthoc comparison of the performance of the recently reported ASAS IBP criteria and the 6-item questionnaire by comparing sensitivity, specificity, LR, and ROC analysis when at least 4 out of the 5 domains from the ASAS IBP criteria were present as required for the diagnosis of IBP (improvement with exercise, pain at night, insidious onset, age at onset < 40 yrs, no improvement with rest). All these domains are included between the Calin criteria and the 6-item questionnaire. A posthoc analysis comparing to the Berlin criteria could not be performed because the study was designed before these were published and therefore particular domains including “alternating buttock pain” were not included15. Analyses were conducted using Stata 9.
RESULTS
Patient characteristics
The established back pain cohort consisted of 286 patients, 220 with IBP and 66 with MBP (Table 1). Overall, mean age was 44 years, 195 were men, and average symptom duration was 14 years. The mean age for patients with MBP was 49 years (range 18–82) compared to 40 years (range 14–73) for the IBP group (p ≥ 0.5). Mean disease duration for the MBP group was 13 years (range 0.3–61) and for the IBP group 15 years (range 0.2–52; p ≥ 0.5). A diagnosis of AS was made in 209 of the patients with IBP, with the definite diagnosis unavailable for 11 patients with IBP. The etiology of MBP for the 66 patients included degenerative disc disease, facet arthritis, and herniated disc. In the majority of cases, however, the specific MBP diagnosis was not recorded in the questionnaire. Eighty-one patients (28%) had symptom duration < 6 years, including 53 patients (24%) with IBP and 28 patients (42%) with MBP. There was a male predominance in the IBP group (170 men, 50 women) in contrast to a female predominance in the MBP group (41 women, 25 men). The frequency of HLA-B27 positivity was 82% (106 patients), with HLA-B27 status known for 130 patients with IBP.
Background characteristics of the patients with mechanical and inflammatory back pain. Data are mean ± SD (95% CI).
Univariate analysis and screening utility of individual items
The frequency of positive responses to the 6-item and Calin question items (domains) that achieved statistical significance in differentiating IBP and MBP patients in the univariate analysis was similar between the 2 questionnaires, except for “morning stiffness” (Table 2). The Calin question identified morning stiffness in 199 of those with IBP (90%) versus 45 MBP patients (68%). The 6-item question for morning stiffness, which was broken down into 2 parts (“Do you experience stiffness in your back and/or hips”; “If yes, when is this most noticeable”), did not identify as many IBP patients with morning stiffness [n = 95 (48%)] compared with the Calin question. While 207 IBP patients (94%) answered “yes” to the presence of stiffness in the back and/or hips, only 95 of these IBP patients (48%) answered in the affirmative when the “time of day of stiffness” was added to the question. However, specificity was considerably higher at 75%, compared to the Calin morning stiffness question (32%).
Classification utility of response to IBP domain questions in patients with inflammatory back pain (IBP) (n = 220) or mechanical back pain (MBP) (n = 66).
The domains in the 6-item questionnaire with the greatest difference in frequency between IBP and MBP included “diurnal variation” (p = 0.0001), “response to rest” (p = 0.01), and “response to exercise” (p = 0.001; Table 2). “Diurnal variation” was reported in only 5 MBP patients (8%) compared with 99 IBP patients (49%). “Response to exercise” was significantly different between IBP and MBP for both questionnaires. “Insidious onset,” a domain recorded only in the Calin criteria, was not helpful in differentiating back pain, being present in 80% of IBP and 76% of MBP patients. “Nocturnal pain” had low sensitivity and specificity for IBP and was therefore not significant in univariate analysis.
Overall, more individual domains were strongly associated with IBP in the 6-item questionnaire (Table 2) compared to the Calin criteria in the univariate analysis. While the individual Calin criteria domains strongly associated with IBP included “age of onset < 40 yrs” (not tested in the 6-item questionnaire), “response to exercise,” and “morning stiffness,” the 6-item questionnaire included 2 additional domains significantly associated with IBP, namely “diurnal variation” (not tested in the Calin criteria) and “response to rest.” The domain “diurnal variation” in the 6-item questionnaire had the highest classification utility of all the individual question items from the Calin and 6-item questionnaires, with a sensitivity of 49% and specificity of 92% and positive LR 6.0, negative LR 0.6.
Multivariate analysis and screening utility of combined items
Multivariate logistic regression analysis showed that the “diurnal variation” domain from the 6-item questionnaire was independently associated with IBP regardless of whether the domains “response to rest” and “response to exercise” were combined or separated in the analyses (adjusted OR 11.18 and 9.37, respectively, p = 0.0001 for both; Table 3). Two additional domains from the 6-item questionnaire were independently associated with IBP in multivariate analyses, including “response to rest” and “response to exercise” (Table 3). In the 6-item questionnaire, the “morning stiffness” domain was not independently associated with IBP (p > 0.5) in contrast to the Calin item for “morning stiffness” (adjusted OR 3.59, 95% CI 1.57–8.22, p = 0.002).
Multivariate logistic regression analysis of inflammatory back pain (IBP) items significant by univariate analysis to determine independent association with IBP.
We combined items from the 6-item questionnaire that were independently associated with IBP in multivariate analysis by either simple summation (additive score, range 0–3) or by application of item weighting based on the beta-coefficient from logistic regression analysis (weighted score = 0.6 × diurnal variation + 0.24 × response to exercise + 0.16 × response to rest). Optimal cutoff scores for the additive and weighted scores in ROC analysis were 2 and 0.4, respectively. The weighted score had a higher sensitivity (60%) compared to the additive score (54%) with comparable specificity (89%–90%), but neither was superior to the classification utility of the single item “diurnal variation” (sensitivity 49%, specificity 92%; Table 4). Both combined item scores and “diurnal variation” outperformed the Calin criteria (sensitivity 83%, specificity 42%). The AUC from ROC analysis for the weighted score (0.77) and single domain “diurnal variation” (0.70) were greater than that seen with the Calin criteria (0.62; p = 0.026 and p = 0.027, respectively). The AUC for the Calin criteria (0.62) was not statistically different from the additive (0.75) score (p = 0.248). The ASAS IBP criteria did not perform as well as either the single item “diurnal variation” or the additive or weighted scores in identifying IBP (Table 4).
Classification utility of candidate tools for inflammatory back pain (IBP): (1) additive score, (2) weighted score, (3) “diurnal variation” single item, (4) Calin criteria, and (5) ASAS IBP according to expert criteria.
Subgroup analysis according to sex and symptom duration
The classification utility of the additive and weighted scores and “diurnal variation” was further assessed in those patients in the lowest tertile of symptom duration, which was < 6 years (Table 5). Both the additive and weighted scores and “diurnal variation” performed even better, with high specificities (> 95%) and increased positive LR (12 to 15) in these patients. Classification utility was also somewhat higher in women, although sample size was small and 95% CI were wide.
Classification utility of candidate tools for inflammatory back pain stratified by sex and symptom duration.
DISCUSSION
We developed a 6-item questionnaire to classify IBP in the clinical setting with future intention to validate the final product in target populations and primary care to ultimately screen for early SpA. We found that our 6-item self-report questionnaire more effectively identified IBP than either the Calin or the ASAS IBP criteria in a population with established back pain. In particular, the single domain “diurnal variation” had the strongest association with IBP in our study. This has not been evaluated previously in any screening tools for IBP. In contrast, the similar domain “morning stiffness” had limited classification utility in both the 6-item self-report and Calin questionnaires and combinations of items did not reveal performance that was superior to the single item diurnal variation domain. Diurnal variation also outperformed the Calin and ASAS IBP criteria.
The Calin criteria were developed from the clinical history of IBP in established AS, whereas the 6-item questionnaire was derived by expert consensus followed by development of standardized questions. The Calin questionnaire is not completed by the patient but rather the rheumatologist, and lacks precise wording for each domain. The questionnaire is only completed if the patient has ever had back pain, whereas the 6-item questionnaire is completed if one has had back and/or hip pain, thereby acknowledging that many patients refer to the buttock region as the “hip”23. “Insidious onset” was omitted from the 6-item questionnaire because investigators felt the term “insidious” is vague and not well defined. Nocturnal pain has been suggested as a characteristic feature of IBP, but it did not attain statistical significance as set out in the 6-item questionnaire. This may relate to patient difficulty in interpreting the wording of this question. The expected answer for IBP would be for pain in the early morning or “second half of the night,” but interpretation of this question and its answer for the IBP compared to the MBP patient was evidently varied and did not achieve statistical significance15. A patient’s understanding of “second half of the night” may be mixed, leading to heterogeneity in responses between MBP and IBP patients (e.g., second half of the night might be midnight onward versus after 3 AM). It is difficult to develop a standardized question that adequately conveys the meaning of this complex domain and our data should not necessarily be interpreted as diminishing the importance of this feature in the evaluation of IBP.
Diurnal variation may have performed so well in our study because the question wording does not address specific symptoms, but rather the time of day when they are most noticeable. While specificity was high (92%), sensitivity was low, at 49%, in the overall group of patients with AS, although higher (58%) in those with symptom duration < 6 years. It is possible that this might reflect disease activity, with more active patients having more obvious diurnal variation in symptomatology. Our data support the conclusions of the ASAS IBP study, which indicated that morning stiffness does not independently discriminate between IBP and nonspecific causes of back pain20.
Our 6-item questionnaire did not consider the Berlin criteria or ASAS expert IBP criteria because they were not published when we developed our questionnaire. However, the Berlin criteria do not detail how the questions can be standardized, leaving specific domains such as “alternating buttock pain” open to interpretation15. Moreover, a posthoc analysis in our study incorporating the 5 domains comprising the ASAS IBP criteria did not perform as well as 1 domain, “diurnal variation,” or the additive and weighted scores. The Berlin criteria comprise 4 domains, “morning stiffness,” “improvement of back pain with exercise and not rest,” “nocturnal pain,” and “alternating buttock pain,” while the ASAS IBP criteria do not include “morning stiffness” or “alternating buttock pain” but add “age less than 40” and “insidious onset” to the other 3 domains, including “improvement with exercise,” “nocturnal pain,” and “no improvement with rest.” The Berlin and ASAS criteria may perform better when administered and critically assessed by clinicians with special expertise in musculoskeletal disorders, but our data suggest that they are unlikely to be useful in primary care practice, where physicians may lack sufficient experience with different presentations of IBP12. The utility to the primary care physician of a single question, “diurnal variation,” or even the self-administered 6-item questionnaire improves the screening of patients with chronic back pain in the general population for SpA.
The utility of self-report questionnaires with standardized questions was recently demonstrated in a case-ascertainment tool for AS, where patient self-report for IBP screening was used13. Weisman, et al identified candidate question items with input from an advisory board, and then drafted and revised a case-ascertainment tool that was validated in a case-control study of 145 cases of AS and 308 cases of chronic back pain with mechanical back pain13. The resulting patient-reported 12-question items had a sensitivity of 67.4% and specificity of 94.6% and included several features of IBP including “neck and/or hip pain/stiffness” and “improvement with daily physical activity.” Ultimately, both the case-ascertainment tool and single item “diurnal variation” strive to identify patients with higher probabilities of having SpA who warrant further evaluation. The case-ascertainment tool did have a greater sensitivity and specificity than “diurnal variation.” However, if the ultimate goal is to identify more patients with potential SpA by creating a tool useful in the primary care office or even a Web-based format, the feasibility of a 12-item instrument compared to a single question raises concern. If there is a slight tradeoff in sensitivity and/or specificity but a greater likelihood for regular use of this question in primary care and specialist offices alike, there is a greater likelihood of identifying patients with IBP requiring further investigation for SpA. A recent study evaluating referral recommendations for patients with chronic back pain by primary care physicians and orthopedists demonstrated the utility of educating primary doctors on SpA features such as IBP24. However, even that study included more than one IBP domain among other recommendations for screening (e.g., HLA-B27).
The primary limitation of our study is that patients had established disease, and the utility of the “diurnal variation” domain requires further testing in a primary care population. The gold standard for diagnosing SpA was the rheumatologist’s diagnosis rather than formal criteria such as the modified New York criteria, although it is likely that most practicing rheumatologists would have used these criteria, as the study was conducted before the appearance of the ASAS criteria for SpA diagnosis. There is a possibility that screening utility of our questionnaire will be lower in unselected patient populations. Nevertheless, our data suggest that primary care physicians should be made aware of diurnal variation as a potentially important characteristic of IBP, and consider referral to a rheumatologist if the patient is young and especially if HLA-B27-positive25. In addition, further studies aimed at developing screening strategies for IBP should incorporate diurnal variation into the study design. Comparing sensitivity/specificity of the 6-item questionnaire to either the Calin or ASAS IBP criteria, respectively, may also be problematic because the Calin and ASAS questionnaires were designed for administration by the interviewing clinician, compared to the 6-item questionnaire that was designed for patient self-report. Therefore, the inferior performance of the Calin or ASAS IBP criteria may reflect this methodological difference in how these questionnaires were designed.
To our knowledge, this is the first report that formally identifies the importance of “diurnal variation” in the diagnosis of IBP. While there are many criteria for IBP based on expert consensus and overlapping domains, none has demonstrated the same initial classification utility as shown with the single domain of diurnal variation. We also suggest that self-report standardized questions can be helpful in screening for a complex disorder such as IBP, and that this may be a more feasible and pragmatic approach than the administration of multiitem tools assessing overlapping domains that are unfamiliar to most primary care physicians. Our proposed approach to screening for IBP, using the single item of diurnal variation completed by the patient, deserves further testing in larger, unselected cohorts of patients and those at higher risk for SpA.
Acknowledgment
The authors thank Dr. Anthony S. Russell for his contribution to the initial development of the 6-item questionnaire.
Footnotes
-
Prof. Majumdar is a Health Scholar supported by Alberta Innovates — Health Solutions.
- Accepted for publication December 7, 2011.








{kind=link}