

To the Editor:
Mycophenolate is one of the mainstays of immunosuppressive therapy after organ transplantation and has also been increasingly used in the treatment of rheumatic diseases1. It is applied either as mycophenolate mofetil (MMF) or its enteric coated formulation (mycophenolate sodium; MPS). The immunosuppressive action of mycophenolate is mainly based on the inhibition of the de novo purine biosynthesis required for the proliferation of T and B lymphocytes2.
We describe a 72-year-old man with a 35-year history of seropositive rheumatoid arthritis (RA). During his disease course he had received multiple disease-modifying antirheumatic treatments (DMARD), which were either ineffective (chloroquine, sulfasalazine, gold) or discontinued because of adverse effects or contraindications (methotrexate, leflunomide). In 2007, the course had been complicated by an infected hip replacement with sepsis and secondary aortic valve endocarditis. A steady decline of his renal function (creatinine clearance 20 ml/min) was attributed to systemic amyloidosis. In September 2010, DMARD treatment with azathioprine was switched to MPS because of toxic bone marrow damage. Shortly thereafter, he developed severe migrating pains in rapidly altering locations together with a severe decline of general status. An increase of the daily glucocorticoid dose (from 5 to 10 mg prednisolone daily) did not alter the symptoms. He was finally admitted to our service in a severely compromised general state and complaining of severe, immobilizing pain and marked tenderness to palpation at multiple discrete periarticular points very atypical of a synovitic cause and without clinical or sonographic signs of synovitis.
Laboratory values showed an increased erythrocyte sedimentation rate (ESR) of 110 mm/h and C-reactive protein (CRP) 57 mg/l (normal < 5 mg/l). An elevated serum procalcitonin (PCT) and subfebrile temperatures to 38°C were present. Intensive investigations including blood and urine cultures, transesophageal echocardiography, endoscopy of the upper gastrointestinal tract, skeletal scintigraphy, ear-nose-throat and dentistry consult, synovial analysis of replaced joints (given the history of infected joint replacement in this patient), and positron-emission tomography combined with computed tomography of the whole body did not reveal an infectious focus or neoplastic disease. Similarly, no evidence of a viral infection (cytomegalovirus, Epstein-Barr virus, hepatitis B and C, human immunodeficiency virus) or of active rheumatic disease was found. Finally, considering the close temporal relationship of symptom onset to initiation of MPS, an MPS-induced acute inflammatory syndrome was suspected. MPS discontinuation was followed by prompt and complete disappearance of all symptoms within 1 day, accompanied by rapid normalization of ESR, CRP, and decline of the PCT level (Figure 1). The patient decidedly rejected a reexposure to mycophenolate (either to MPS or MMF). He was discharged a few days later without further intervention and since then has been seen regularly as an outpatient for as long as 7 months, reporting lasting well-being under monotherapy with low-dose prednisolone.

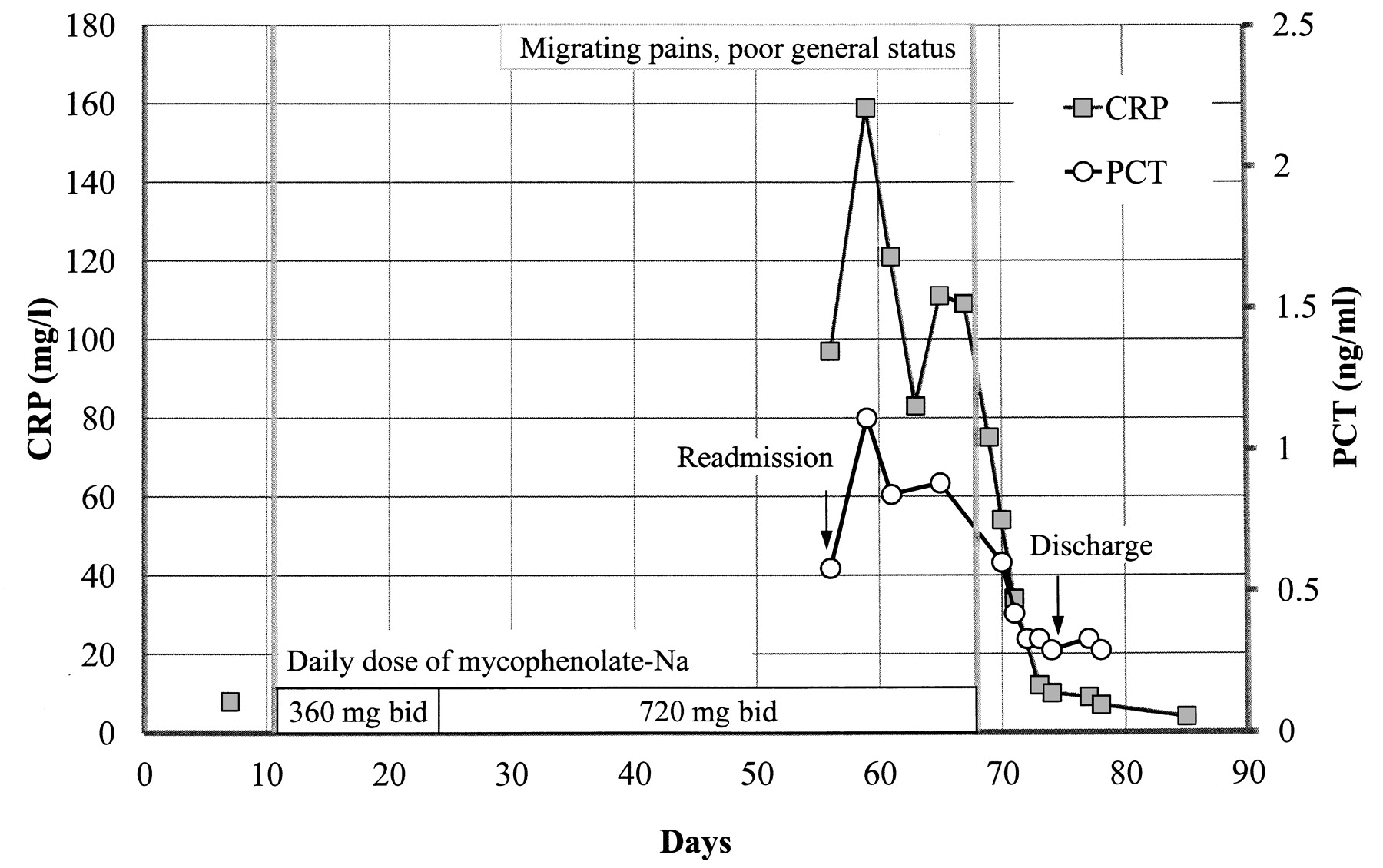
Time course of levels of serum C-reactive protein (CRP; normal < 5 mg/l) and procalcitonin (PCT; normal < 0.1 ng/ml). Vertical lines represent initiation and discontinuation of mycophenolate sodium (MPS). After 2 weeks, the MPS dose had been increased from 360 mg to 720 mg twice daily. Arrows represent times of readmission and discharge from hospital. No laboratory data were available from the time between MPS initiation and readmission.
To our knowledge, this report (being 1 of only 4 case descriptions of an acute inflammatory syndrome attributable to mycophenolate) is the first in which the reaction is due to intake of MPS. Further, it is also the first description in a patient with RA. Four other patients have been reported: 2 with granulomatosis with polyangiitis (Wegener’s), one after renal transplant, and one with systemic lupus erythemodes3,4,5. The symptoms described in those cases were very similar to those in our patient. All other patients had received MMF, and 2 of them showed identical symptoms after reexposure to the drug. The mechanism by which mycophenolate induces an acute inflammatory response in some individuals remains obscure. Ex vivo stimulation in the presence of mycophenolate induces paradoxically increased oxidative bursts in neutrophils of affected patients5. Moreover, mycophenolate acyl glucuronide metabolite concentrations correlate with serum interleukin 6 (IL-6) levels in patients with the acute inflammatory syndrome3. In our patient, a severe renal insufficiency could have contributed to the observed adverse reaction by an impaired excretion of a responsible agent.
We show for the first time that PCT levels are also elevated during MPS-associated acute inflammatory syndrome. PCT is an established marker of systemic inflammation in bacterial infection and sepsis and correlates with serum IL-6 levels6. Thus it can be speculated that mycophenolate metabolite-mediated IL-6 production induces elevated PCT serum levels in the acute inflammatory syndrome. Interestingly, increased PCT serum levels have also been described recently in patients with idiosyncratic inflammatory drug reactions to azathioprine and carbamazepine, and in the neuroleptic malignant syndrome7,8,9. Therefore, drug reactions should be considered in the differential diagnosis of inflammatory states with elevated PCT in rheumatic diseases.
The ability of mycophenolate to induce an acute inflammatory response appears to be rare and less appreciated than the similar systemic inflammatory reaction to azathioprine. However, awareness of the syndrome is important in routine clinical care, since discontinuation of the responsible agent results in prompt resolution of the symptoms.








{kind=link}