

Abstract
Objective. Magnetic resonance imaging (MRI) is playing an increasingly important role in the diagnosis and followup of juvenile idiopathic arthritis (JIA). Carpal depressions are commonly observed in healthy children and in patients with JIA. The aim of our study was to further characterize these depressions in patients with JIA.
Methods. A total of 29 MRI wrist examinations were analyzed. Depressions were classified according to morphology as either tubular or focal. Features including the presence of a vessel related to the depression, evidence of synovitis, bone marrow edema, or loss of joint space on a radiograph taken on the same day were recorded for each depression.
Results. A total of 173 depressions were identified in 145 carpal bones. Forty percent were capitate depressions. A third were focal depressions and two-thirds were tubular. About 10% of tubular depressions and 30% of focal depressions were associated with features suggesting true erosions, with the remainder likely to represent vascular channels and normal variants.
Conclusion. Radiologists and clinicians should undertake caution when assessing carpal depressions on MRI because the vast majority are likely to represent normal variants.
Juvenile idiopathic arthritis (JIA) has been defined as arthritis of unknown cause occurring in children under the age of 16 years. It is the most common rheumatic disorder of childhood, with a prevalence of 0.6 to 1.9 in 1000 children1. JIA is an important chronic disease of childhood and although it is transient and self-limiting in most cases, about 10% of children remain severely disabled in adulthood2. Pathologically it involves acute synovitis, progressing to synovial hypertrophy resulting in osteocartilaginous degeneration and bony erosions, with ensuing functional disability. The recent development of more specific therapies makes accurate assessment of early disease and response to treatment imperative, enabling “fine-tuning” of patients into specific treatment algorithms3.
Although the knee is the most commonly involved joint, early JIA changes are most frequently identified in the small joints of the hands and feet1. Conventional radiographs are currently regarded as the “gold standard” for initial radiologic evaluation and assessment of disease progression in JIA4,5,6. Detection of erosions by plain radiography has been accepted as a specific and relatively sensitive diagnostic test for JIA. Although able to quantify joint damage, radiography early in the disease is nonspecific and late changes are irreversible1,7. However, magnetic resonance imaging (MRI) has played an increasingly important role in the diagnosis of JIA. A semiquantitative review of the diagnostic accuracy of MRI concluded that MRI is an accurate diagnostic method for evaluating synovium and cartilage in JIA and for assessing clinical responsiveness to treatment in peripheral joints8. Nevertheless, there has been little objective analysis of the use of MRI in assessment of bony erosions in JIA, whereas its use in rheumatoid arthritis (RA) has been more extensively studied. MRI has been demonstrated to be more sensitive than radiography in detecting erosive bone changes in RA9,10,11 and MRI assessment of bony erosions forms an important component of the widely used Outcome Measures in Rheumatology Rheumatoid Arthritis MRI Scoring System (OMERACT RAMRIS). The latter, a semiquantitative scoring system for assessing synovitis, bone erosions, and bone edema on MRI in RA hands and wrists, has been developed with data from iterative multicenter studies12,13,14,15 and a similar scoring system is being developed for MRI assessment of the wrist in JIA.
A report addressing the presence of erosions in the wrist in JIA16 adopted the OMERACT MRI definition of bony erosions in adults: sharply marginated bone lesions with correct juxtaarticular location and low signal intensity in T1-weighted images in at least 2 planes with a cortical break in at least 1 plane12. The aim of our study is to further analyze the significance of carpal depressions on MRI and in particular to determine whether these represent destructive change or normal variation. A further objective is to compare MRI and plain radiography in the assessment of carpal depressions in children with JIA.
MATERIALS AND METHODS
Patients
Children were selected from a database of 43 cases diagnosed with JIA by our center, as defined by the International League of Associations for Rheumatology revised criteria17. Inclusion criteria stipulated that patients had an MRI and plain radiograph of the same wrist no more than 2 days apart. Cases with extensive bony erosions, severe crowding, or fusion of the carpal bones were excluded. A total of 29 children met these criteria, 10 of whom were boys. The median age was 12 years and 8 months (age range 5–16 years).
Imaging protocol
For radiography, a polydoros SX80 generator (Siemens, Erlangen, Germany) and Fuji CR plates/Fuji 5000R CR reader/processing station (Fuji, Tokyo, Japan) were used. The procedure was explained and consent was obtained. The date of last menstrual period of girls over 12 years of age was determined.
For MRI, imaging was performed using a 1.5-Tesla Advanto scanner (Siemens) with up to 40 mT/m gradient strength. The procedure was explained to the patient and safety checks were performed. The patient lay head-first in the scanner and headphone or video entertainment was provided. A surface coil was applied and imaging of the wrist in the coronal and axial planes was performed. The following sequences were obtained: T1w coronal fast spin-echo (TR 556, TE 22, slice thickness 3 mm, gap 0 mm, NEX 2, matrix 512 × 250), T1w 3-D spin-echo (TR 600, TE 2, slice thickness 3 mm, gap 0 mm, NEX 2, matrix 512 × 288), T2w coronal turbo spin-echo (TR 3600, TE 95, slice thickness 3 mm, gap 0.3 mm, NEX 3, matrix 512 × 192), volumetric interpolated breath-hold examination fat saturation, precontrast and immediate postcontrast (TR 4.3, TE 2.02, slice thickness 2 mm, gap 0.4 mm, NEX 1, matrix 256 × 192), as well as a 10-min postcontrast sequence (TR 550, TE 22, slice thickness 3 mm, gap 0 mm, NEX 2, matrix 512 × 154).
Imaging analysis
Each case was allocated an individual identification number, and 2 radiologists (Reader 1 and Reader 2) with 4 years of imaging experience were blinded to clinical and other imaging data. A bony depression was defined as a focal bony concavity. Reader 1 reviewed the imaging of all 29 cases. Reader 2 randomly reviewed the imaging of 10 of the cases to enable assessment of interrater reliability. Depressions identified on MRI and plain radiographs in 5 carpal bones (scaphoid, lunate, capitate, hamate, and the trapezium/trapezoid unit) were evaluated independently by the 2 radiologists. The 3-D T1w coronal fast spin-echo sequences were analyzed for each case and depressions were recorded on a 2-D age-adjusted radiographic template of the wrist (Figure 1). Depressions identified on MRI were categorized and recorded on the template as either focal or tubular, based on their configuration (Figures 2–5 are examples).

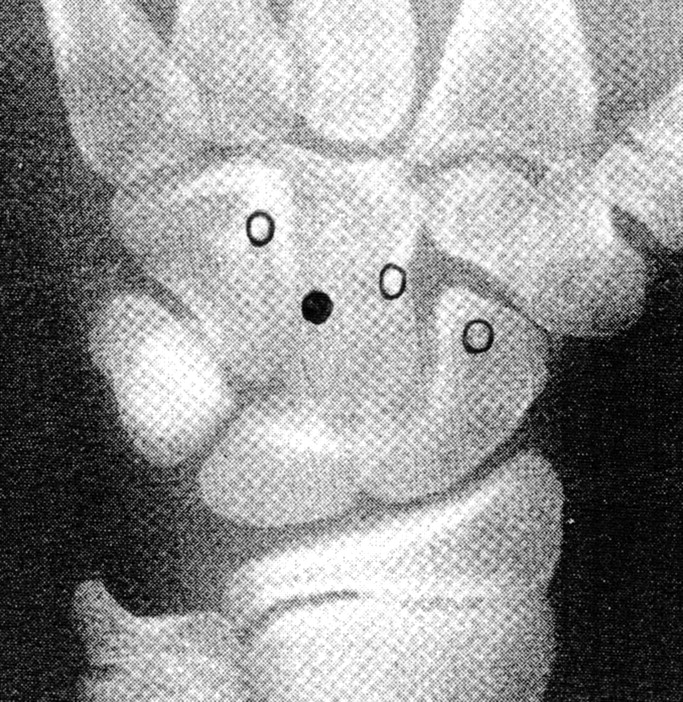
Two-dimensional age-adjusted radiographic template of the wrist used to record erosions identified on magnetic resonance imaging (MRI) and plain radiographs. On this template of an MRI of an 11-year-old, focal depressions are indicated by circles and a tubular depression by a filled-in circle.

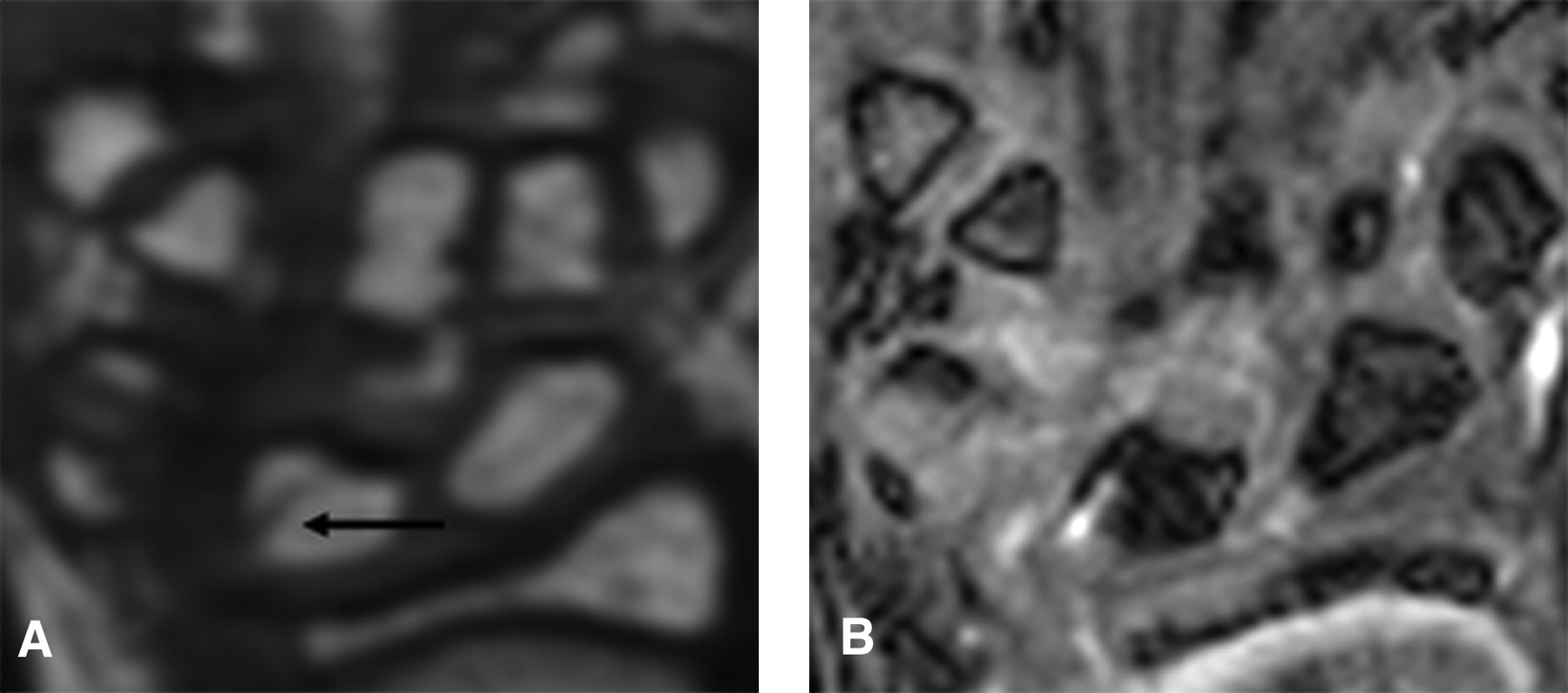
Three-dimensional coronal T1 fast spin-echo (A) and coronal volumetric interpolated breath-hold examination postcontrast (B) showing a focal depression (arrows) that is likely to represent a true erosion, in the trapezoid of a 13-year-old girl.
The plain radiograph for each case was then read and depressions were marked on a separate radiographic template.
The observers were unmasked and the templates illustrating the MRI and plain radiograph findings for each child were compared. The location of each individual depression was noted and the data tabulated for each carpal bone, to include the number and type of depressions identified on MRI and the number of depressions identified on radiography. Comparison of the findings enabled the depressions identified at the same site within a carpal bone on both MRI and radiography to be recorded, and it was then possible to extrapolate the number of depressions that were detected on MRI alone and on plain radiographs alone.
Further characterization of every depression identified on MRI was achieved by assigning individual numbers to each focal and tubular depression. The depressions illustrated on the templates (Figure 1) were labeled with their corresponding numbers. Lists of all the focal and tubular depressions were compiled and a further review of the remaining MRI sequences and inspection of the radiographs were performed, to identify and record any pathological features related to the depressions. The T1w coronal fast spin-echo was compared with the postcontrast T1w coronal fat saturation to determine whether there was evidence of pathological synovial enhancement adjacent to each depression or whether the enhancement was more in keeping with the presence of a vessel. In addition, evidence of high signal within the carpal bones adjacent to the depressions on the T2w coronal turbo spin-echo and low signal on the T1w sequence in keeping with bone edema was also noted. Finally, loss of joint space on plain radiographs in the carpus in the immediate vicinity of depressions identified on MRI was recorded. Depressions associated with the pathological features described were regarded as true erosions, whereas those where there was evidence of an intimately related adjacent vessel were labeled as vascular channels. The remaining depressions, in which neither of the latter features were present, were regarded as normal variants.
RESULTS
On MRI, 173 depressions were identified within a total of 145 carpal bones (29 patients). Capitate depressions represented almost 40% of the total. Of the 173 depressions, 112 were tubular and 61 were focal (Table 1). Fourteen of the 115 tubular depressions were identified on radiography compared with 23 out of 62 focal depressions. Interestingly, 13 depressions were seen on plain radiograph alone.
Number and type of depressions identified on radiographs and magnetic resonance imaging (MRI). Data are n (%).
Of the tubular depressions, 10.4% were associated with pathological features and were regarded as true erosions, while 76.5% were likely vascular channels. The remaining 13% may therefore represent normal variants.
Of the focal depressions, 27.4% met our criteria for true erosions, with 41.9% identified as vascular channels and 30.7% likely normal variants.
Of the depressions identified on plain radiographs, 22% represented true erosions, 40% were vascular channels, and 38% were considered normal variants.
Reader 2 randomly reviewed 10 of the cases. There was exact agreement on location and presence of 22 out of 26 focal depressions identified by Reader 1, compared with agreement on 34 out of 39 tubular depressions. Of the 22 focal depressions, there was agreement that 18 represented normal variants/vascular channels and 2 represented true erosions. There was disagreement over the nature of 2 of the depressions. There was agreement that all 34 of the tubular depressions represented either vascular channels or normal variants.
DISCUSSION
We have demonstrated that not all carpal depressions are likely to represent erosions, and this distinction is vital to enable accurate characterization of disease in JIA.
A review of the literature reveals that only 1 study has assessed the prevalence of MRI findings of bone edema, effusions, and erosion-like changes in the wrist joints of healthy children18, but none have analyzed synovial enhancement in asymptomatic children due to the inability to administer contrast. However, a number of studies have assessed the wrists of healthy adult patients, including 2 in which contrast examinations were performed, revealing changes resembling bone erosions and mild synovitis in a significant number of healthy control subjects19,20. Ejbjerg, et al describe bone erosion-like changes in 2% of 420 healthy adult volunteer carpal bones, all of which were small and in the capitate or lunate19. The majority of these did not show associated enhancement on postcontrast imaging. Many changes resembling erosions in healthy subjects are therefore likely to represent normal variants, and this distinction is vital to enable accurate disease characterization in JIA. A study by Malattia, et al16 addressing the use of MRI of the wrist in JIA adopted a simplified version of the OMERACT MRI scoring system for erosions whereby only the morphology of the bone was taken into consideration. No regard was given to features supporting the presence of erosions such as bone edema, effusions, and evidence of synovitis. The study found “erosions” on MRI in 96% of the patients, including 100% of patients with disease duration under 3 years. About half the patients were found to have “erosions” on plain radiography. This is likely to be an overestimation, particularly in view of the fact that half the patients were under the age of 10 years and had had a relatively recent onset of disease.
The OMERACT RAMRIS defines an MRI bony erosion as a sharply demarcated area of focal bone loss seen in 2 planes, with a cortical break in at least 1 plane. We believe this definition should be revised, particularly when applied to the analysis of wrist MRI in children. We propose that the following definition be adopted: a bony depression larger than that seen in a normal bone and associated with additional pathological features such as an effusion, synovial enhancement, and/or loss of joint space on plain radiography. Individual analysis of all the bony depressions identified within the 145 carpal bones examined on MRI and plain radiographs in our study revealed that the vast majority of depressions did not fit this definition and were instead likely to represent normal variation. In fact, only about one-fifth of depressions, whether focal or tubular, were likely to represent true erosions (Figures 2 and 3 are examples of depressions that are likely to represent true erosions). There were large differences in the number of MRI depressions identified in the individual bones, with capitate depressions accounting for almost 40% of the total. Scaphoid and trapezium/trapezoid unit depressions, on the other hand, accounted for only 12% and 19.6% of the total, respectively. The proportion of depressions that had features suggestive of erosions varied considerably according to the bone: 12% for the capitate, 24% for scaphoid depressions, and 30% of trapezium/trapezoid depressions. This implies that overall capitate depressions are more common and are more likely to represent normal variation when compared with trapezium/trapezoid and scaphoid depressions.

Three-dimensional coronal T1 fast spin-echo (A) and coronal volumetric interpolated breath-hold examination postcontrast (B) showing a tubular depression (arrows) that is likely to represent a true erosion, in the lunate of a 16-year-old girl.
Analysis of the morphology of the depressions revealed that in the case of tubular depressions, up to 76.5% were found to represent vascular channels, compared with 42% of focal depressions (Figures 4 and 5 are examples of tubular and vascular depressions that corresponded to vascular channels). Besides vascular channels, the identification of irregularities of the subchondral cortex caused by the normal maturation of cartilage in growing joints is a further likely explanation for some of the depressions identified. Alternatively, some that did not have associated pathological features may represent true erosions in “burned out” disease or even “arrested erosions.” Future work may be able to further clarify this.
Three-dimensional coronal T1 fast spin-echo (A) and coronal volumetric interpolated breath-hold examination postcontrast (B) showing a tubular depression (arrows) that is likely to represent a vascular channel, in the lunate of a 15-year-old girl.

Three-dimensional coronal T1 fast spin-echo (A) and coronal volumetric interpolated breath-hold examination postcontrast (B) showing a focal depression (arrows) that is likely to represent a vascular channel, in the capitate of a 7-year-old girl.
The second objective of our study was to compare MRI and plain radiography in the detection of carpal depressions. The latter are much better visualized by MRI than by conventional radiography because of 3-D image acquisition21, and the number of carpal depressions identified on MRI in our study was much greater than that identified on plain radiographs. On MRI, 173 depressions were found, and of these only 37 were visible on radiograph. This is a similar proportion to that described in an RA study comparing the sensitivity and specificity for the detection of bone erosions on MRI and radiography using computed tomography (CT) as the reference method22. This revealed a sensitivity of 61% for MRI and 24% for radiography. Clearly, given radiation concerns, CT does not have a role in the routine assessment of JIA. Nevertheless, these data illustrate the fact that a considerable proportion of carpal depressions are not identifiable on MRI or radiography. The ability of MRI to identify bone edema and effusions is key to its use in JIA. However, plain radiography will continue to have an important role because of its ability to demonstrate loss of joint space, which is a key feature that is not adequately demonstrated on MRI. Also of interest are the 13 depressions that were seen on plain radiographs alone and not detected on MRI; most of them were subtle depressions along the “edge” of the affected carpal bone. In the majority of these depressions, there was other plain radiograph evidence of destruction but no MRI signs of active inflammation, suggesting that these are “burned out” lesions.
Our study shows that many bony depressions can be falsely labeled as erosions, and a study on healthy children is warranted.
Radiographic assessment of JIA disease severity based on the presence of carpal “erosions” should be undertaken with caution because about 80% of carpal depressions may be normal variants. Radiologists and clinicians should be fully aware of these potential pitfalls. The development of an MRI atlas of normal maturation of cartilage in the wrist may allow direct assessment of the articular cartilage, allowing more reliable recognition of pathological irregularities in the subchondral cortex and therefore more accurate diagnosis of early bone erosions.
- Accepted for publication November 1, 2011.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}