
Abstract
Objective. Galectin-3 is a multifunctional protein implicated in a variety of biological processes including fibrosis, angiogenesis, and immune activation, all of which are associated with the development of systemic sclerosis (SSc). We investigated the clinical significance of serum galectin-3 levels in SSc.
Methods. Serum galectin-3 levels were determined by a specific ELISA in 58 patients with SSc and 19 healthy controls.
Results. Serum galectin-3 levels were significantly lower in patients with diffuse cutaneous SSc (dcSSc) than in controls (3.29 ± 3.27 ng/ml vs 4.91 ± 2.67 ng/ml, respectively; p < 0.05), while being comparable between limited cutaneous SSc (3.70 ± 2.39 ng/ml) and healthy controls. In dcSSc, serum galectin-3 levels significantly correlated with total skin score (r = 0.45, p < 0.05). Serum galectin-3 levels were significantly decreased in early dcSSc (disease duration < 1 year; 1.64 ± 1.74 ng/ml; p < 0.05), but not in mid-stage dcSSc (1 to 6 years; 3.22 ± 3.16 ng/ml) or late-stage dcSSc (> 6 years; 4.86 ± 4.10 ng/ml), compared with controls. Serum galectin-3 levels were higher in SSc patients with both digital ulcers (DU) and elevated right ventricular systolic pressure (RVSP) than in those without each symptom (DU: 5.44 ± 3.74 ng/ml vs 2.99 ± 2.36 ng/ml, p < 0.05; elevated RVSP: 4.44 ± 3.14 ng/ml vs 2.82 ± 2.64 ng/ml, p < 0.05).
Conclusion. Galectin-3 may be related to the developmental process of skin sclerosis in dcSSc and of DU and pulmonary vascular involvements in total SSc.
- SYSTEMIC SCLEROSIS
- GALECTIN-3
- SKIN FIBROSIS
- PULMONARY ARTERIAL HYPERTENSION
- DIGITAL ULCER
Systemic sclerosis (SSc) is a multisystem autoimmune disease characterized by initial vascular injuries and resultant fibrosis of skin and certain internal organs1. Although the pathogenesis of SSc remains unknown, an increasing number of growth factors, cytokines, and other molecules have been shown to be involved in the complex network of signaling pathways driving aberrant immune activation, dysregulated angiogenesis, and deposition of extracellular matrix throughout the course of this complex disorder.
Lectins are carbohydrate-binding proteins with a selective affinity for specific oligosaccharides2. Galectins are a growing family of ß-galactoside-binding animal lectins, 15 members of which have been identified to date3. Among them, galectin-3 has a unique structure whereby its single polypeptide chain forms 2 structurally distinct domains, such as the C-terminal carbohydrate recognition domain and the atypical N-terminal domain2. While the C-terminal domain is responsible for lectin activity of galectin-3, the N-terminal participates in multimer formation and secretion of galectin-3 and in oligosaccharide binding4,5,6. In normal adults, galectin-3 has been detected mainly in epithelial cells and myeloid cells, including the epithelium of gastrointestinal and respiratory tracts, renal distal tubules, activated macrophages, eosinophils, neutrophils, and mast cells3. In addition, galectin-3 displays pathological expression in many tumors, such as thyroid, pancreatic, and colon cancers7. Although galectin-3 is predominantly located in the cytoplasm, it has also been found on the cell surface, within the extracellular matrix, and in the nucleus, suggesting the pleiotropic roles of galectin-3 depending on its localization3. Intracellular galectin-3 inhibits apoptosis, regulates the cell cycle, and participates in the nuclear splicing of pre-messenger RNA8,9,10,11. Its extracellular functions encompass cell to cell and cell to matrix adhesions12,13,14, angiogenesis15, fibrosis16,17,18,19, and the activation of various immune cells, such as macrophages, neutrophils, mast cells and lymphocytes20,21,22,23,24. Consistent with its various roles, the levels of soluble and/or cellular galectin-3 are increased in autoimmune diseases such as systemic lupus erythematosus, rheumatoid arthritis, and Behçet’s disease, and correlate with their disease activities25,26,27.
This situation led us to focus on the role of galectin-3 in the mechanism responsible for the development of SSc. As an initial step, we measured the serum levels of galectin-3 in patients with SSc and evaluated their association with clinical features.
MATERIALS AND METHODS
Patients
Serum samples, frozen at −80°C until assayed, were obtained from 58 consecutive patients with SSc (56 women, 2 men; mean age 57.0 ± 14.2 yrs; mean disease duration 7.9 ± 10.2 yrs) who presented to the dermatology department of Tokyo University Hospital, a tertiary academic center in Japan, and 19 healthy individuals (18 women, 1 man; mean age 56.0 ± 10.0 yrs) without history or family history of SSc. All subjects gave informed consent, and institutional approval was obtained (University of Tokyo Graduate School of Medicine). Patients were excluded if they had been treated with corticosteroids or other immunosuppressants against clinical symptoms associated with SSc prior to their first visits. Patients were grouped by LeRoy’s classification system1: 29 with limited cutaneous SSc (lcSSc) and 29 with diffuse cutaneous SSc (dcSSc). All patients with dcSSc and 26 of the patients with lcSSc fulfilled the criteria proposed by the American College of Rheumatology28. Three patients with lcSSc not meeting these criteria had sclerodactyly and at least 2 other features of SSc, such as calcinosis, Raynaud’s phenomenon, esophageal dysfunction, and telangiectasia. All patients but those with skin sclerosis clinically limited to distal to hands underwent skin biopsy and were histologically diagnosed as having SSc.
Measurement of serum galectin-3 levels
Specific ELISA kits were used to measure serum galectin-3 levels (R&D Systems, Minneapolis, MN, USA). Briefly, polystyrene 96-well plates coated with antigalectin-3 antibodies were incubated with 100 μl of serum at room temperature for 2 h. Then the wells were washed and incubated at room temperature for 2 h with horseradish peroxidase-conjugated antigalectin-3 antibodies. Next, the wells were washed again, added to tetramethylbenzidine, and incubated at room temperature for 30 min. Finally, H2SO4 was added to terminate the reaction and the absorbance at 450 nm was measured. Serum galectin-3 levels were calculated using the standard curve.
Clinical assessments
The clinical and laboratory data were obtained when the blood samples were drawn. Patients were evaluated for the presence of esophageal, cardiac, renal, joint, and muscle involvements as described29,30. Skin score was measured using modified Rodnan total skin thickness score (mRSS)31. The degree of interstitial lung disease (ILD) was evaluated by the percentage of predicted vital capacity (%VC) and the percentage of predicted %DLCO on pulmonary function test. Elevated right ventricular systolic pressure (RVSP) was defined as ≥ 35 mm Hg on echocardiogram. Disease onset was defined as the first clinical event of SSc other than Raynaud’s phenomenon. Disease duration was defined as the interval between disease onset and the time the blood samples were drawn.
Statistical analysis
Statistical analysis was carried out with the Mann-Whitney U test for 2-group comparisons, with a Kruskal-Wallis test and a Steel-Dwass test for multiple comparisons, and with Fisher’s exact probability test for the analysis of frequency. Correlations with clinical data were assessed by Spearman’s rank correlation coefficient. Statistical significance was defined as a p value < 0.05.
RESULTS
Serum galectin-3 levels in SSc
Serum galectin-3 levels in patients with SSc were significantly lower than those in healthy individuals (3.50 ± 2.85 vs 4.91 ± 2.67 ng/ml, respectively; p = 0.035, Mann-Whitney U test). Since the expression profiles of certain growth factors and cytokines can be quite different between dcSSc and lcSSc, we also evaluated serum galectin-3 levels in these subgroups. As shown in Figure 1, serum galectin-3 levels were significantly lower in patients with dcSSc (3.29 ± 3.27 ng/ml) than in healthy controls (p < 0.05, Kruskal-Wallis test and Steel-Dwass test), while there was no significant difference in serum galectin-3 levels between patients with lcSSc (3.70 ± 2.39 ng/ml) and controls (p > 0.05, Kruskal-Wallis test and Steel-Dwass test). Collectively, the decrease in serum galectin-3 levels may be associated with some aspects of the disease process in dcSSc.

Serum galectin-3 levels in patients with diffuse cutaneous systemic sclerosis (dcSSc), limited cutaneous SSc (lcSSc), and healthy individuals. Serum galectin-3 levels were determined by a specific ELISA. Bars indicate the mean value in each group. Statistical analysis by Kruskal-Wallis test and Steel-Dwass test for multiple comparisons.
Serum galectin-3 levels correlate with the severity of skin sclerosis, but not ILD, in dcSSc
Since dcSSc is characterized by progressive skin sclerosis and ILD, we next focused on this patient group and evaluated the association of serum galectin-3 levels with fibrotic response in skin and lung. To this end, we looked at the correlation of serum galectin-3 levels with mRSS, %VC, and %DLCO in dcSSc.
A significant positive correlation was found between serum galectin-3 levels and mRSS in patients with dcSSc (r = 0.45, p < 0.05; Figure 2). In contrast, neither %VC nor %DLCO showed a significant correlation with serum galectin-3 levels in dcSSc (data not shown). Given a profibrotic effect of galectin-3 in various pathological fibrotic conditions16,17,18,19, these results suggest that galectin-3 is associated with the development of dermal fibrosis, but not ILD, in dcSSc.
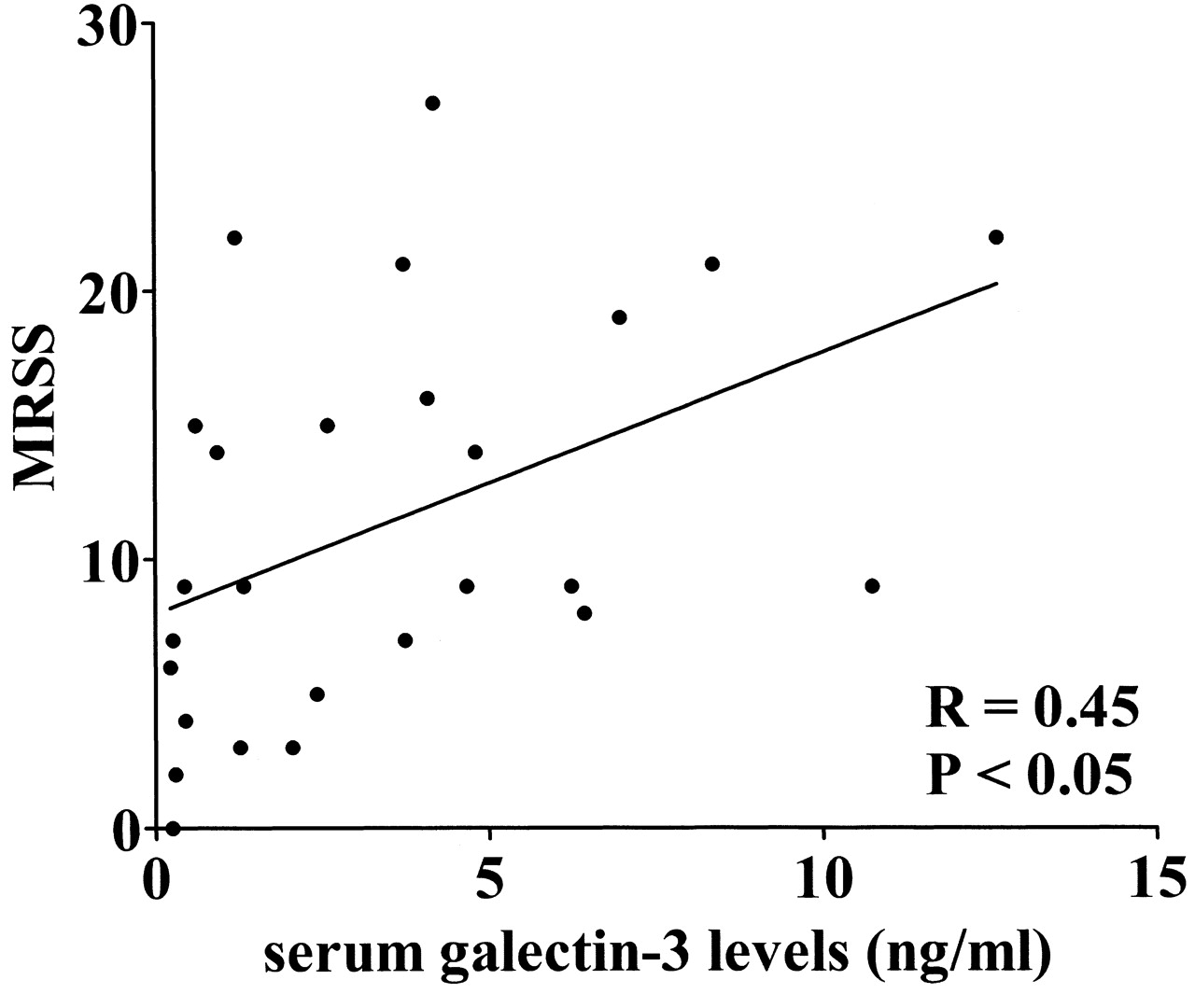
Correlation of serum galectin-3 levels with modified Rodnan total skin thickness score (MRSS) in patients with diffuse cutaneous systemic sclerosis (dcSSc). A significant positive correlation was found between serum galectin-3 levels and MRSS in patients with dcSSc (r = 0.45, p < 0.05, Spearman’s rank correlation test). Solid line represents the regression line.
Decrease in serum galectin-3 levels and initiation of dermal fibrotic responses in dcSSc
As described, serum galectin-3 levels correlated positively with mRSS in dcSSc. However, this result appears to be contradictory to the finding that serum galectin-3 levels are relatively decreased in patients with dcSSc compared with patients with lcSSc. One of the plausible explanations for this observation is that reduction of galectin-3 levels may largely contribute to the initiation of fibrosis in the early stage of dcSSc, but not afterward. To assess this hypothesis, we classified patients with dcSSc into 3 subgroups according to their disease duration, that is, early dcSSc (disease duration < 1 year), mid-stage dcSSc (disease duration 1 to 6 years), and late-stage dcSSc (disease duration > 6 years), and evaluated the correlation of serum galectin-3 levels with disease duration (Figure 3). Supporting our hypothesis, serum galectin-3 levels were decreased in patients with early dcSSc (1.64 ± 1.74 ng/ml) compared with healthy controls (p < 0.05, Kruskal-Wallis test and Steel-Dwass test), while there was no significant difference between patients with mid-stage dcSSc (3.22 ± 3.16 ng/ml) or late-stage dcSSc (4.86 ± 4.10 ng/ml) and controls (p > 0.05, Kruskal-Wallis test and Steel-Dwass test). Therefore, the reduction of galectin-3 may contribute to the initiation of dermal fibrosis in early dcSSc, probably modulating immune responses.

{kind=link}
{kind=link}
{kind=link}
Serum galectin-3 levels in patients with diffuse cutaneous systemic sclerosis (dcSSc) classified into 3 subgroups based on disease duration < 1 year, disease duration 1 to 6 years, and disease duration > 6 years. Serum galectin-3 levels were determined by a specific ELISA. Horizontal bars indicate the mean value in each group. Statistical analysis by Kruskal-Wallis test and Steel-Dwass test for multiple comparisons.
Elevated serum galectin-3 levels and development of digital ulcer and pulmonary vascular involvement in SSc
To further investigate the association of serum galectin-3 levels with clinical manifestations of SSc other than skin fibrosis and ILD, we classified patients with SSc into 2 groups according to the presence or absence of each organ involvement and compared serum galectin-3 levels between these 2 groups (Table 1). Among various organ involvements, digital ulcer (DU) and elevated RVSP were associated with elevated serum galectin-3 levels in SSc. Serum galectin-3 levels were higher in SSc patients with DU than in those without (5.44 ± 3.74 vs 2.99 ± 2.36 ng/ml; p = 0.033). Further, patients with elevated RVSP showed higher galectin-3 levels than those without (4.44 ± 3.14 vs 2.82 ± 2.64 ng/ml; p = 0.033). These results indicate that the increase of galectin-3 may be involved in the mechanism responsible for the development of DU and pulmonary vascular involvement leading to pulmonary arterial hypertension in SSc.
Associations of serum galectin-3 levels with organ involvement.
DISCUSSION
Although the pathogenesis of SSc is still unknown, experimental data from patient cells and sera continue to provide us with clues to the mechanism responsible for the development of fibrosis, vasculopathy, and autoimmunity in this complicated disorder. Recent studies demonstrating pleiotropic effects of galectin-3 on fibrosis, angiogenesis, and immune activation led us to investigate if this cytokine is involved in the pathological events in SSc. As an initial step to address this issue, we investigated serum galectin-3 levels and their associations with clinical features in SSc. Serum galectin-3 levels were significantly lower in patients with dcSSc than in controls, while there was no significant difference in serum galectin-3 levels between patients with lcSSc and controls. Serum galectin-3 levels were decreased in patients with early-stage dcSSc compared with controls, while mid-stage and late-stage patients had serum galectin-3 levels similar to those in controls. Together with the finding that serum galectin-3 levels did not correlate with %VC or %DLCO, but with mRSS in dcSSc, galectin-3 may be involved in the development of dermal, but not pulmonary, fibrotic response in dcSSc, probably through its profibrotic and immunomodulating effects. On the other hand, elevated serum galectin-3 levels were linked to the development of DU and pulmonary vascular involvement in total SSc. Therefore, galectin-3 appears to play some roles in the pathological events relevant to vasculopathy as well as dermal fibrosis in SSc.
A series of in vivo and in vitro studies demonstrated that galectin-3 plays a pivotal role in the developmental process of certain pathological fibrotic conditions. A study by Henderson, et al16 demonstrated that galectin-3 is upregulated in established human fibrotic liver disease and is temporally and spatially related to the induction and resolution of experimental hepatic fibrosis. Further, RNA interference-mediated silencing of the galectin-3 gene inhibits myofibroblastic differentiation of hepatic stellate cells, and galectin-3-null mice are resistant to the development of CCL4-induced hepatic fibrosis largely due to the lack of transforming growth factor-ß (TGF-ß)-induced transactivation of hepatic stellate cells. Similarly, Henderson, et al16 also revealed that galectin-3 expression and secretion by macrophages promotes renal myofibroblast accumulation/activation and fibrosis in a mouse model of progressive renal fibrosis. These data suggest that galectin-3 is required for TGF-ß-mediated myofibroblast activation and matrix production in certain types of pathological fibrosis. Supporting this idea, serum levels of galectin-3 reflect the severity of fibrotic conditions in liver and heart diseases32,33,34,35,36, and bronchoalveolar lavage fluid levels of galectin-3 correlate with the severity of pulmonary fibrosis37 in humans. As for the association of galectin-3 with dermal fibrosis, a recent study by Dvoránková, et al19 demonstrated that galectin-3 induces the expression of α-smooth muscle actin, a marker of myofibroblasts, suggesting that galectin-3 exerts a profibrotic effect by promoting the activation of dermal fibroblasts into matrix-secreting myofibroblasts. With our current data that serum galectin-3 levels positively and significantly correlate with mRSS but with neither %VC nor %DLCO in dcSSc, galectin-3 may be associated with the development of dermal fibrosis, but not ILD. To confirm this, we are currently investigating the significance of galectin-3 for the establishment of myofibroblastic phenotype in SSc dermal fibroblasts.
A growing body of evidence demonstrated that galectin-3 is one of the important factors skewing Th1/Th2 polarization of the Th cell response in various pathological conditions. For instance, galectin-3 induces selective downregulation of interleukin 5 (IL-5) gene expression in several cell types, including eosinophils, T cell lines, and antigen-specific T cells38. Consistently, treatment of chronic asthmatic mice with gene therapy using plasmid encoding galectin-3 leads to an improvement in Th2 allergic inflammation39. On the other hand, galectin-3 deficiency reduces the development of experimental autoimmune encephalomyelitis40, where Th1 and Th17 cells are thought to be responsible for the inflammatory demyelination, by decreasing interferon-γ and IL-17 production but expanding populations of Th2 cells and inducible regulatory T cells. Thus, galectin-3 promotes the pathological Th1/Th2 polarization in a context-dependent manner.
In the case of SSc, serum galectin-3 levels were decreased in its early stage, but reversed up to normal levels afterward. The dynamics of galectin-3 along with disease course implies that galectin-3 acts as a factor promoting the Th1 polarization in SSc according to the canonical Th1/Th2 paradigm in this disorder. In the early stage of dcSSc with progressive skin sclerosis, serum levels of IL-6 and IL-10 are significantly elevated, while levels decreased to normal in the late stage of dcSSc with the improvement of skin sclerosis41. Another Th2 cytokine, IL-4, has normal levels in the early stage of dcSSc, but is decreased as well in the late stage of dcSSc. In contrast, serum levels of IL-12, a key Th1 cytokine, are decreased in the early stage of dcSSc, then gradually increase in parallel with disease duration and finally reach significantly higher levels than normal controls in the late stage of dcSSc with the resolution of skin sclerosis42.
Of note, the maximal levels of serum IL-12 throughout the disease course correlate inversely with mortality in early dcSSc with diffuse cutaneous involvement. Thus, immune polarization in SSc generally shifts from Th2 to Th1 in parallel with disease duration, while the sustained Th2 immune polarization closely associates with exacerbation of the disease. Therefore, the decrease in galectin-3 levels may contribute to the initiation of the disease by decelerating the Th1 polarization of the Th cell response in concert with various cytokines in early stage SSc.
Another important pathological aspect of galectin-3 is to exert a potent proangiogenic effect in concert with various proangiogenic factors, including vascular endothelial growth factor and basic fibroblast growth factor15,43. In our study, serum galectin-3 levels were significantly elevated in patients with DU or elevated RVSP compared to those without, in total SSc. Given that macrovascular involvement, which is characterized by intimal thickening, is closely associated with severe skin ulcers, galectin-3 may be linked to the development of proliferative vasculopathy, such as pulmonary vascular involvement leading to pulmonary arterial hypertension and macrovascular involvement, in total SSc. Although the detailed mechanism of proliferative vasculopathy remains unknown, proliferation of endothelial cells and vascular smooth muscle cells due to aberrant activation of angiogenesis may play a pivotal role in this pathological process44. Increasing evidence revealed that angiogenic factors can be placed in 2 categories: the factors inducing proliferation and differentiation of endothelial cells (e.g., basic and acid fibroblast growth factor, vascular endothelial growth factor, and TGF-α), and the factors inducing differentiation but not proliferation of endothelial cells (e.g., angiogenin, TGF-ß, and tumor necrosis factor-α)45. Although it appears to belong to the latter category15, galectin-3 may accelerate the activation of pathological angiogenesis leading to proliferative vasculopathy in concert with various proangiogenic factors promoting endothelial proliferation.
We have reported the first study, to our knowledge, regarding the clinical significance of serum galectin-3 levels in SSc. A series of analyses indicate that galectin-3 may be associated with the pathological events relevant to the development of skin fibrosis and proliferative vasculopathy in SSc. Our study supports previous findings that galectin-3 may be involved in the mechanism responsible for the development of autoimmune diseases.
Footnotes
-
Supported by a grant for Research on Intractable Diseases from the Ministry of Health, Labor, and Welfare of Japan.
- Accepted for publication October 28, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.