
Abstract
Objective. To assess the utility of interferon-α (IFN-α) in serum and cerebrospinal fluid (CSF) as a biomarker of disease activity in central neuropsychiatric systemic lupus erythematosus (cNPSLE).
Methods. Serum and CSF samples were drawn at hospitalization in 34 patients with cNPSLE, 16 surgical SLE, 4 primary neuropsychiatric conditions, and 25 with nonautoimmune conditions, except in 44 non-NPSLE patients in whom only serum was studied. Six months later, serum/CSF and serum samples were taken in 20 cNPSLE and 35 non-NPSLE patients, respectively. SLE activity was assessed at hospitalization, and 6 months later in cNPSLE and non-NPSLE patients. IFN-α was detected by Luminex technology.
Results. The mean ± SD age of patients with cNPSLE was 31.4 ± 12.2 years, which was similar across the study groups (p = 0.46). Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) scores among cNPSLE, non-NPSLE, and SLE-surgical patients were 15.3 ± 8.2, 12.4 ± 8.2, and 3.8 ± 1.5, respectively. IFN-α levels in serum were higher in cNPSLE than in nonautoimmune patients (p = 0.02), but were similar to non-NPSLE and SLE-surgical groups. In CSF samples, IFN-α levels were higher in cNPSLE than in nonautoimmune patients (p = 0.03), and were nonsignificantly higher than in SLE-surgical and primary neuropsychiatric patients. Six months later, serum levels of IFN-α did not vary from baseline values despite a significant decrease in SLEDAI-2K score in cNPSLE and non-NPSLE patients. IFN-α levels in the CSF of patients with cNPSLE also remained stable. Among specific cNPSLE syndromes, CSF IFN-α levels were significantly higher among patients with acute confusional syndrome.
Conclusion. IFN-α does not seem to represent a useful biomarker of cNPSLE syndromes; its utility in specific cNPSLE manifestations merits further investigation.
- SYSTEMIC LUPUS ERYTHEMATOSUS
- INTERFERON-α
- BIOMARKER
- NEUROPSYCHIATRIC
Systemic lupus erythematosus (SLE) is a chronic multisystemic autoimmune disease that may involve the nervous system, resulting in a variety of neurologic and psychiatric manifestations1. The American College of Rheumatology (ACR) classifies neuropsychiatric manifestations of SLE into 19 syndromes, which include psychiatric, central, and peripheral manifestations2. At present, an accurate indicator of central nervous system (CNS) involvement in SLE has not been identified.
Several studies have identified type I interferons (IFN-I) as agents in the pathogenesis of SLE3. Thus, patients with SLE can have increased serum levels of IFN-α, especially those with cutaneous and renal disease4,5,6,7. Gene expression microarray studies have revealed a strikingly homogeneous pattern of upregulated IFN-inducible genes in almost all patients with SLE compared to normal blood donors or patients with rheumatoid arthritis8,9,10. The sum of these genes induced by IFN-I, known as the IFN signature, includes several chemokines and cytokines plus additional molecules such as transcription factors and antiviral proteins11,12.
Because studies of IFN-α levels in both cerebrospinal fluid (CSF) and serum in neuropsychiatric SLE (NPSLE) are scarce and outdated13,14,15, we assessed the utility of IFN-α levels in serum and CSF as a biomarker of disease activity in patients with central NPSLE (cNPSLE), and investigated the correlation between serum and CSF levels of IFN-α.
MATERIALS AND METHODS
Patients
Thirty-four patients with SLE according to the ACR criteria16, hospitalized between February 2003 and June 2005 because of central NP manifestations, were studied (cNPSLE group). All patients were evaluated by the study rheumatologists and neurologists, at hospitalization and 6 months later, using a standardized protocol. At hospitalization, sociodemographic data and information on SLE characteristics including disease activity assessment by the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K)17 were collected. Serum and CSF samples were obtained from all patients at hospitalization when the NP manifestations were active and in 20 patients 6 months later, when the NP manifestations were clinically quiescent. NP manifestations were classified using the ACR nomenclature for NP lupus syndromes2. Central NP manifestations included seizure disorders (n = 13), severe refractory headache (n = 7), acute confusional state (n = 8), cerebrovascular disease (n = 4), psychosis (n = 1), and transverse myelitis (n = 1). NP manifestations were attributed to SLE given that there were no exclusion factors for it2, and no patient had any of the minor NP events that have been reported with a comparable frequency in the general population18.
As controls we studied 4 groups of patients as follows. (1) Non-NPSLE group: 44 consecutive patients with SLE with no history of NP manifestations, malignancies, or severe infection, who were hospitalized. These were also evaluated by the study rheumatologist at hospitalization and 6 months later, and serum samples were obtained from all patients at hospitalization and in 35 patients 6 months later. The main reasons for hospitalization were SLE activity (n = 40; disease diagnosis, renal, hematological, pneumonitis, serositis, hepatitis, fever), pulmonary thromboembolism (n = 2), and miscellaneous (n = 2). (2) SLE-surgical group: serum and CSF samples were obtained from 16 SLE patients without history of NP manifestations who underwent an elective surgery. (3) Primary neurological group: 4 patients with primary NP disorders, optic neuritis (n = 2), Devic’s syndrome (n = 2). Serum and CSF samples were obtained during clinical assessment upon hospitalization. (4) Nonautoimmune group: 25 patients with neither autoimmune disease nor NP manifestations who underwent elective surgery for the following conditions: bone marrow donors (n = 7), hysterectomy (n = 7), Tenckhoff catheter collocation (n = 3), hydrocele (n = 2), lower limb amputation due to diabetes mellitus type II (n = 2), saphenectomy (n = 2), circumcision (n = 1), and inguinal hernioplasty (n = 1). Serum and CSF samples were obtained during clinical assessment upon hospitalization.
Serum was collected, and CSF was centrifuged at 12,000 g. Serum and the CSF supernatant were immediately frozen (< 30 min) at −86°C until assayed for the determination of IFN-α.
IFN-α was measured using Luminex bead-based technology according to the manufacturer’s recommendation (Milliplex Map; Millipore Corp., Billerica, MA, USA). The detection limit of the experimental system was 3.2 pg/ml.
The study was approved by the Institutional Committee of Biomedical Research and all patients provided signed informed consent.
Statistical analysis
Categorical variables were compared using chi-square or Fisher’s exact test. Continuous variables were analyzed using Student’s t test, Mann-Whitney U test, Wilcoxon signed-rank test, paired t test, or 1-way ANOVA. IFN-α values are presented as median (range). The correlation coefficients were estimated using Spearman’s rho. P value was set at < 0.05, 2-tailed.
RESULTS
Characteristics of the study population
At entry, the mean ± SD age of patients in the cNPSLE group was 31.4 ± 12.2 years, and no difference was observed across the study groups (p = 0.46). Disease duration in patients with cNPSLE was shorter than in the non-NPSLE group, 3.6 ± 4.5 and 8.8 ± 7.2 years (p = 0.05), respectively, but similar to that of patients in the SLE-surgical group. Disease activity was severe in patients in the cNPSLE and non-NPSLE groups, with SLEDAI-2K scores 15.3 ± 8.2 and 12.4 ± 8.2, respectively; and mild in the SLE-surgical group (Table 1).
Demographic characteristics and interferon-α (IFN-α) levels in serum and cerebrospinal fluid (CSF) from patients with central neuropsychiatric systemic lupus erythematosus (cNPSLE) and controls at the time of hospitalization. Except where indicated otherwise, values are the mean ± SD.
IFN-α levels in serum and CSF in study groups
In serum, IFN-α levels in patients with cNPSLE were higher than those in patients with nonautoimmune diseases (p = 0.02), but no difference was observed compared with the other SLE groups, including the SLE-surgical group, which had mild disease activity, and patients with primary autoimmune disorders.
In CSF, IFN-α levels were higher in the cNPSLE group in comparison with patients with nonautoimmune disorders (p = 0.03). Also, nonsignificant higher values were observed in comparison to patients in the SLE-surgical and primary autoimmune groups (Table 1).
Paired assessments of IFN-α levels in cNPSLE and non-NPSLE patients
In patients with cNPSLE, serum IFN-α levels remained stable after 6 months from the onset of NP manifestations, when they were clinically quiescent, median 52.4 pg/ml (range 3.2–1074.4) and 77.6 pg/ml (range 3.2–2321.4; p = 0.20) correspond to serum IFN-α levels of the cNPSLE group at baseline and 6 months later, respectively. The median (min–max) 24.1 (3.2–193.3) and 35.1 (3.2–64.1), respectively (p = 0.40), correspond to CSF IFN-α levels of cNPSLE group at baseline and 6 months later, respectively.
The median (min–max) 101.2 (11.7–3641.5) and 77.3 (2.3–6350.6) (p = 0.41) correspond to IFN-α serum levels of non-NPSLE group at baseline and 6 months later, respectively.
Stability of IFN-α levels was observed at 6 months, despite a significant decrease in SLEDAI-2K score in the patients with cNPSLE and the non-NPSLE patients, minus 11.05 and 7.5 points (p < 0.001), respectively (Table 2).
Serum/CSF IFN-α levels and SLEDAI-2K score from cNPSLE and non-NPSLE patients determined at baseline and 6 months.
Correlation of IFN-α levels in patients with cNPSLE
The correlation coefficient of serum and CSF levels of IFN-α in the 54 samples drawn from the 34 patients with cNPSLE was rs = 0.25 (p = 0.07).
Correlation of IFN-α levels with disease activity in cNPSLE patients
At the onset of NP manifestations, the correlation coefficients between IFN-α levels and SLEDAI-2K scores were rs = 0.33 (p = 0.05) in serum and rs = 0.32 (p = 0.06) in CSF. However, among the 20 patients with paired serum and CSF samples, the correlation coefficients using all the samples were rs = 0.09 (p = 0.60) in serum and rs = 0.21 (p = 0.19) in CSF.
Posthoc analysis of IFN-α levels in specific NPSLE manifestations
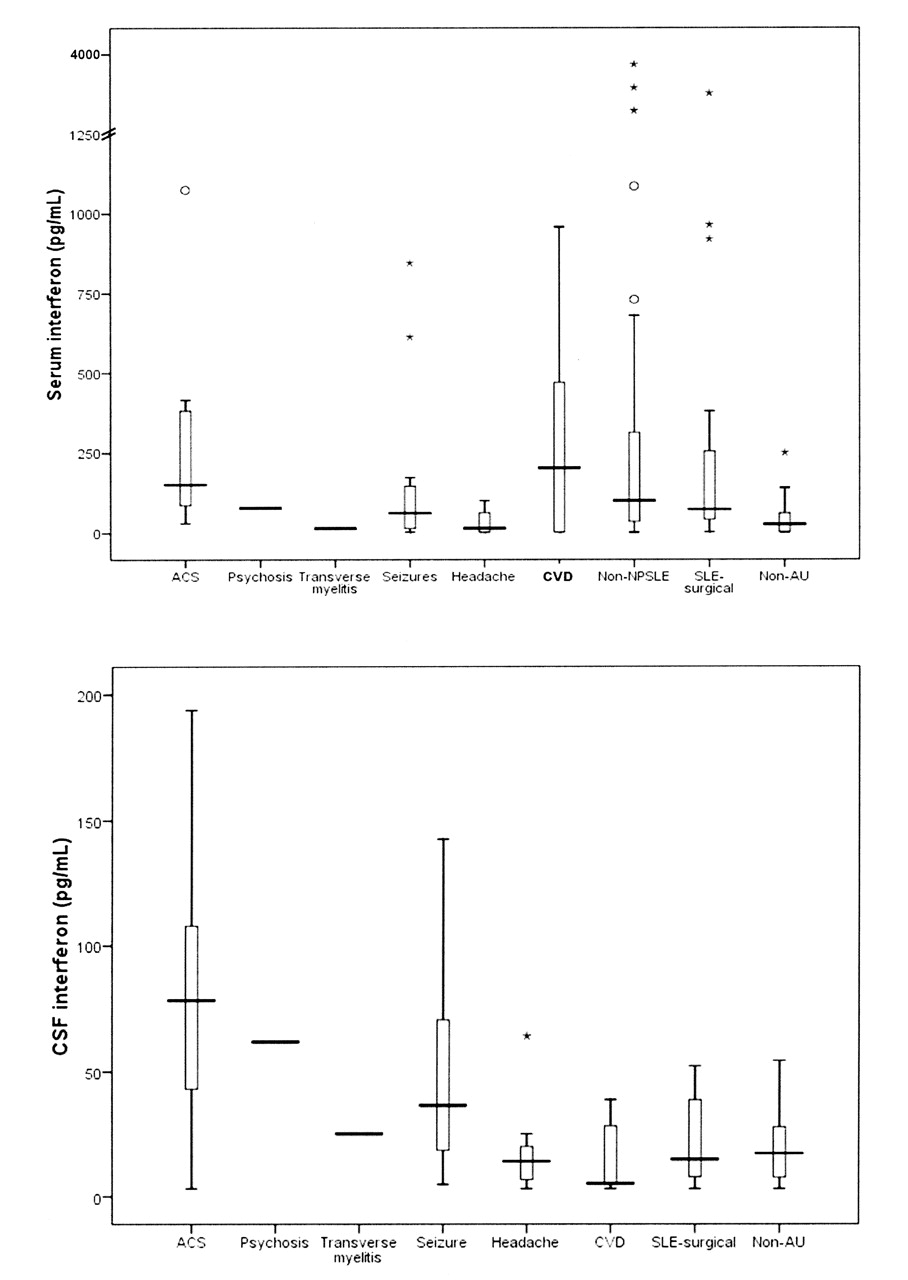
No difference was found in serum IFN-α levels among patients with NPSLE, SLE controls, and nonautoimmune groups (Figure 1). In CSF samples, however, patients with acute confusional state showed significantly higher IFN-α levels compared to those with severe refractory headache (p < 0.02) and the SLE-surgical (p < 0.009) and nonautoimmune (p < 0.001) groups (Figure 1). Unfortunately, the sample size did not allow analysis in paired assessments during the acute and quiescent periods.

{kind=link}
Levels of interferon-α (IFN-α) in serum (upper panel) and cerebrospinal fluid (CSF; lower panel) in patients with specific central neuropsychiatric systemic lupus erythematosus (cNPSLE) manifestations, non-NPSLE, surgical SLE, and nonautoimmune patients. ACS: acute confusional syndrome; CVD: cerebrovascular disease; non-AU: nonautoimmune.
DISCUSSION
SLE is a heterogeneous disease with variable combinations of several gene polymorphisms that contribute to susceptibility19,20. Most patients with SLE share an increased expression of IFN-I-induced genes that is more pronounced during disease activity4,5,6,7. This indicates that the different genetic backgrounds leading to SLE converge on the IFN-I signaling pathway. Although most patients with SLE have increased expression of IFN-I-induced genes, not all of them have high levels of serum IFN-I4,5,6,7,8,9.
We found that IFN-α levels in serum and CSF were significantly higher in patients with SLE than nonautoimmune patients. However, IFN-α levels in serum did not discriminate patients with active cNPSLE manifestations, active non-NPSLE manifestations, and SLE patients with mild disease. Although higher IFN-α levels in CSF were observed among patients with cNPSLE, no clear difference could be established with the other groups studied, except patients with nonautoimmune disease. Paired analyses of IFN-α levels in serum and CSF during the active and quiescent phases of cNPSLE manifestations did not differ, and a similar situation was observed in patients with non-NPSLE. Finally, IFN-α levels in serum and CSF correlated poorly.
Most cross-sectional studies of patients with SLE have demonstrated an association between activation of IFN-I pathway and disease activity. Recently, however, 2 studies evaluating the longitudinal expression of IFN-induced genes have shown that, although higher IFN response scores were associated with increased disease activity, the IFN scores of individual patients did not correlate with changes in disease severity or the risk for disease flare, indicating that IFN-induced gene expression has limited clinical utility as a biomarker of acute changes in disease activity21,22. A more recent study that included a multiethnic cohort of 1089 patients with SLE analyzed the presence or absence of the ACR clinical criteria for SLE, autoantibodies, and serum IFN-α activity by univariate and multivariate models23. It was found that IFN-α activity was strongly associated with autoantibodies, regardless of the known differences among patients of different ethnic background, but not with clinical manifestations. The authors concluded that IFN-α may be more relevant to humoral tolerance and initial pathogenesis, rather than in later clinical disease manifestations. Another possible explanation that has not been explored in depth is that, rather than an increased IFN-I production, SLE could be associated with an increased responsiveness to IFN-I.
Our data complement these studies. As described among SLE patients without NP manifestations, in our patients with NPSLE, IFN-α levels in serum and CSF seemed to have fair correlation with disease activity during the outbreak of NP manifestations, but in the followup samples the correlation waned. Our results differ from those reported in patients with lupus psychosis, where principally the CSF levels of IFN-α were correlated with disease activity13. In our study, IFN-α levels in SLE patients with cerebrovascular disease, seizures, severe refractory headache, and non-NPSLE were not elevated and did not differ from levels in nonautoimmune patients. Since we included only 1 patient with psychosis and 1 with transverse myelitis, we are unable to argue about the utility of serum and CSF measures of IFN-α in these manifestations; nevertheless, it is notable that patients with acute confusional state were the ones that showed significantly higher levels of IFN-α in CSF, compared with the other NPSLE syndromes.
Whether IFN-α plays a critical role in specific NP manifestations is difficult to ascertain because of the heterogeneous expression of SLE, and particularly for the 19 syndromes that comprise NPSLE, where necessarily each one of them must have different pathogenic mechanisms, as we observed, at least in CSF from patients with acute confusional state.
Previously, it was shown that instead of evaluating IFN-α levels, monitoring chemokines induced by IFN-α (CXCL10, CCL-2, and CCL19) in SLE may improve the assessment of current disease activity and the prediction of future disease flares24. In this regard, we recently showed that NPSLE patients have significantly higher CSF levels of CXCL10 at the onset of NP manifestations, and the levels of this chemokine showed a statistically significant decrease after 6 months, when the disease was clinically quiescent25. We concluded that CXCL10 may be considered as a preponderant chemokine in the development of NPSLE. Interestingly, it was also shown24 that CXCL10 was the chemokine that was consistently the most strongly associated with current and future disease activity, raising the possibility that serum CXCL10 levels may represent a stand-alone biomarker of SLE activity.
We must highlight some potential limitations of our study. (1) Although a relatively large number of patients with NP manifestations were included and we did detect a correlation between IFN-α and cNPSLE, the study was not adequately powered to determine a correlation with specific manifestations. Therefore, our results should be interpreted with caution since NPSLE manifestations are likely to be due to heterogeneous mechanisms. (2) Our results apply to patients with acute NP manifestations who needed to be hospitalized for diagnosis or treatment. We did not study non-hospitalized patients or patients with chronic serious manifestations, e.g., depression, seizures, or cognitive dysfunction. (3) We did not carry out screening for NP manifestations among the patients with no history for them, thus although none had any of the acute and severe manifestations of patients with cNPSLE, we cannot exclude that they had mild or subclinical NP manifestations. (4) Although at 6 months the NPSLE patients were clinically in remission, we cannot exclude ongoing, subclinical NP activity that might have been associated with the presence and levels of IFN-α.
Our study also has strengths that need to be emphasized. (1) This is the first study to assess levels of IFN-α in serum and CSF, in various groups of patients with SLE and in subjects without autoimmune disease. Thus, several groups of negative controls were assembled. (2) The paired assessment in serum and CSF of IFN-α during the acute episode and 6 months later provides unique information about the sensitivity of levels of IFN-α to change in the status of NP manifestations. (3) All patients were assessed prospectively following a standardized evaluation, and determination of IFN-α was blinded to the diagnosis and the study group. Further, all patient sera and CSF samples were evaluated simultaneously to avoid intraassay variability.
Levels of IFN-α in serum and CSF in cNPSLE were not higher than those in patients with non-NPSLE. No correlation with disease activity was observed; therefore, IFN-α levels do not seem to represent a useful biomarker of CNS involvement in patients with SLE.
- Accepted for publication October 18, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.