

Abstract
Objective. The underlying mechanism(s) by which antiphospholipid antibodies (aPL) result in thrombosis remains poorly understood. A significant body of evidence has evolved to support the hypothesis that antibody-mediated disruption of an annexin A5 anticoagulant shield may play a role in the pathogenesis; this proposed mechanism has not been previously studied in children.
Methods. We investigated the association between aPL and resistance to annexin A5 anticoagulant activity in 90 children with a variety of rheumatic diseases using a novel mechanistic assay, the annexin A5 resistance assay (A5R).
Results. Patients with a diagnosis of primary aPL syndrome, systemic lupus erythematosus, and mixed connective tissue disease demonstrated lower mean A5R levels (p = 0.030), higher prevalence of positive aPL (p < 0.001), and more thrombotic events (p = 0.014) compared to those with other diagnoses. Patients with persistently positive aPL had significantly lower mean A5R compared to patients with no aPL (mean A5R = 203% ± 44% vs 247% ± 35%; p < 0.001), whereas patients with transient aPL did not. Patients with thrombosis had lower A5R levels compared to those without thrombosis (mean A5R = 207% ± 36% vs 237% ± 46%; p = 0.048).
Conclusion. Children and adolescents with rheumatic diseases and persistent aPL have reduced annexin A5 anticoagulant activity, whereas transient, nonpathogenic aPL have less effect on annexin A5 activity.
- PEDIATRIC RHEUMATIC DISEASES
- PEDIATRIC SYSTEMIC LUPUS ERYTHEMATOSUS
- ANTIPHOSPHOLIPID ANTIBODIES
- ANNEXIN A5
Antiphospholipid antibody syndrome (APS), a condition defined as the presence of antiphospholipid antibodies (aPL) in close association with vascular thrombosis and miscarriage, is the most common acquired autoimmune thrombotic state in children1. The underlying mechanism(s) by which aPL result in clinically significant thrombosis remains poorly understood. Current aPL assays were empirically derived from observations over 50 years, with immunoassays developed from biologic false-positive syphilis tests and lupus anticoagulant assays from the observation of an inhibitor to the partial thromboplastin time. These assays are difficult to interpret because they do not directly report on pathophysiologic mechanisms, and have a wide variability in laboratory methods, isotype detection, and clinically significant cutoffs.
A recent mechanism has been proposed to explain the pathophysiology of APS involving resistance to annexin A5, a potent anticoagulant protein that is localized on vascular endothelial cells, placental villi, activated platelets, and apoptotic cells. Annexin A5 proteins crystallize to form an anticoagulant shield over potentially thrombogenic cell surfaces, thereby blocking availability of anionic phospholipids from phospholipid-dependent coagulation reactions2. It has been demonstrated through atomic force microscopy that aPL interfere with the binding of annexin A5 to phospholipids, disrupting this protective shield, and potentially allowing coagulation reactions and increased clotting to occur3,4. The clinical relevance of this protein has been demonstrated by reports of marked reduction in annexin A5 on placental villi and vascular endothelial cells in patients with aPL, and by demonstration of significantly higher antiannexin A5 antibodies in patients with systemic lupus erythematosus (SLE) who have recurrent thrombosis and fetal loss5,6,7,8.
These findings have been translated into a novel mechanistic clinical assay, the annexin A5 resistance assay (A5R)9. The principle underlying this assay is that phospholipid-dependent coagulation reactions occur unimpeded in the absence of annexin A5. When present, annexin A5 rapidly binds to phospholipids, forming a protective anticoagulant shield, consequently prolonging coagulation time. The presence of aPL interferes with the formation of this shield, attenuating the anticoagulant effects of annexin A5. The A5R assay measures coagulation times in the presence and absence of annexin A5 and expresses the difference as an anticoagulant ratio2. A reduction of this ratio, as compared to healthy controls, can be seen in patients with aPL and reflects resistance to annexin A5 anticoagulant activity. This mechanistic coagulation assay reports on a proposed pathogenesis of APS, and studies have demonstrated a significant reduction in mean A5R levels in women with histories of recurrent spontaneous pregnancy losses and in adults with APS9,10.
To our knowledge, examination of A5R has not been previously investigated in children. We evaluated children and adolescents with primary rheumatologic diseases that have been associated with aPL-related manifestations [including primary APS, SLE, mixed connective tissue disease (MCTD), and Sjögren’s syndrome (SS)] and compared them with children with other autoimmune diseases less likely to be associated with aPL-related manifestations. We hypothesized that there may be an association between aPL and reduced A5R levels (i.e., increased resistance to annexin A5 anticoagulant activity) in children and adolescents with rheumatic diseases that subsequently may be associated with clinical manifestations.
MATERIALS AND METHODS
Study population
After Institutional Review Board approval, clinical and laboratory data were collected from 90 children and adolescents followed in the pediatric rheumatology clinic at Children’s Hospital at Montefiore, Bronx, NY. Pediatric patients in this clinic are seen until they are 21 years old with known primary rheumatic diseases including primary APS, SLE, MCTD, SS, juvenile idiopathic arthritis (JIA), juvenile dermatomyositis (JDM), systemic sclerosis (SSc), and systemic vasculitis. We divided our study population into 2 groups based on prior knowledge regarding the prevalence of aPL and aPL-related manifestations. The high-risk group included primary APS, SLE, and SLE-like illnesses (including SS and MCTD), and the low-risk group included JIA, JDM, SSc, and systemic vasculitis.
Clinical data were collected through chart review until the time of data entry and included demographic features (age, sex, ethnicity, and race), primary rheumatologic disorder, history of associated aPL clinical manifestations (confirmed arterial/venous thrombosis, Raynaud’s phenomenon, thrombocytopenia, livedo reticularis, neurologic manifestations, heart valve disease, and nephropathy), current medications [corticosteroids, immunosuppressive agents, hydroxychloroquine (HCQ), aspirin, anticoagulation agents, and oral contraceptive pills], and evidence of other underlying risk factors for thrombosis (inherited thrombophilias, renal disease, hormonal contraception, smoking, and family history). All thrombotic events were confirmed by objective findings on imaging studies, including magnetic resonance imaging/angiography, ultrasonography, ventilation perfusion scan, and 1 patient with skin biopsy.
We defined pediatric APS as an extension of the revised Sydney classification criteria. Based on these criteria, diagnosis of APS requires a persistent positivity of lupus anticoagulant (LAC), IgG, and/or IgM anticardiolipin (aCL) antibody, and/or anti-ß2 glycoprotein I (anti-ß2GPI) antibody of IgG, and/or IgM present on 2 or more occasions at least 12 weeks apart in association with clinical events (including vascular thrombosis or pregnancy-related morbidity)11.
Laboratory testing
Blood specimens were collected from all patients upon entry into the study. All assays were performed in the clinical laboratories of Montefiore Medical Center by technologists blinded to the clinical status of the patients. Laboratory data included a comprehensive aPL panel, including LAC and IgG/IgM/IgA isotypes of aCL and anti-ß2GPI antibodies. Testing for LAC was performed using the Staclot dRVV screen and Staclot dRVV Confirm (Stago, Parsippany, NJ, USA), a commercially available method based upon the dilute Russell viper venom time. Testing for the other components of the comprehensive aPL panel was performed by enzyme immunoassay on a PhD platform (Biorad, San Diego, CA, USA). Positive values for aPL were defined by laboratory cutoffs, regardless of titer, and were repeated at least 3 months later to confirm antibody persistence. In addition, all previously collected laboratory data regarding aPL status were included in the assessment of transient versus persistent aPL positivity.
To examine the effects of plasma samples on annexin A5 activity, we used a 2-stage method, as described4,9,10. This assay measures coagulation times in the presence and absence of annexin A5:

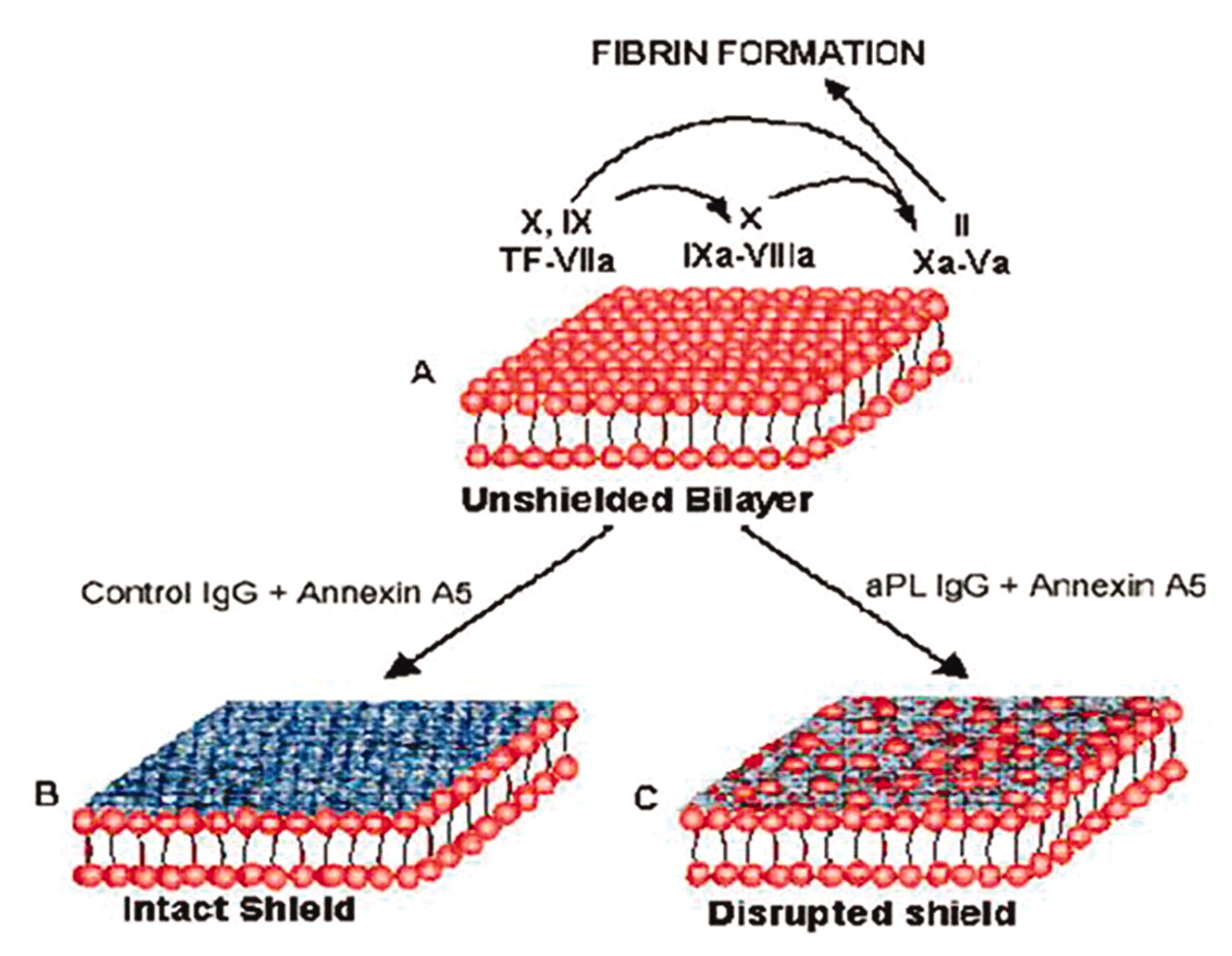
Model for antiphospholipid antibody (aPL)-mediated disruption of annexin A5 shield. (A) Phospholipid bilayers, unshielded by annexin A5, expose thrombogenic phospholipids that accelerate coagulation reactions by serving as scaffolds for the assembly of coagulation enzyme cofactor-substrate complexes. (B) In the presence of annexin A5, that protein rapidly binds to the bilayers and forms a 2-dimensional crystal that blocks the phospholipids from availability for binding coagulation proteins. (C) aPL disrupt the binding and assembly of annexin A5 crystals on the bilayers, creating defects in the crystalline array that expose phospholipids and accelerate coagulation reactions2.

Measurement of annexin A5 (AnxA5) resistance. The assay is based on activated partial thromboplastin time and prothrombin time coagulation assays. Test samples are incubated with a tissue factor-phospholipid suspension. This allowed antiphospholipid antibody antibodies, if present, to bind to phospholipids. The phospholipid sample is washed free of plasma, then added to normal plasma in the presence and absence of AnxA5, which is then recalcified with calcium. The coagulation times in the presence and absence of AnxA5 are measured, and the result is expressed as the AnxA5 anticoagulant ratio. Reduction of this ratio compared to a control population represents AnxA5 resistance2.
Statistical analysis
Statistical analysis was conducted using Stata software, version 11.1 (Stata, College Station, TX, USA). All data analyses were preceded by extensive data checking and verification to identify and resolve the reasons for missing values, inconsistencies, and out-of-range values. Descriptive statistics were computed to summarize each variable, including the mean, median, and SD for continuous variables; and frequencies and interquartile range for categorical variables. All tests were 2-sided, and p values < 0.05 were considered statistically significant. Means of continuous variables were compared using a Student t test or ANOVA and frequencies of categorical variables were compared using chi-square test or Fisher’s exact test. In cases of non-normally distributed data, Wilcoxon signed-rank test and Kruskal-Wallis test were performed. However, due to an overall normal distribution of mean A5R levels and a minimal discrepancy between statistically significant p values between parametric and nonparametric tests, we report results from the parametric tests. Mean A5R levels were compared in each of 3 subgroups: (1) persistently positive aPL serology, (2) transiently positive aPL serology, and (3) persistently negative aPL serology. Posthoc analysis between 2 groups was further conducted. Mean A5R levels were additionally analyzed in the following groups: (1) persistently positive aPL and aPL-related manifestations, (2) persistently positive aPL in the absence of clinical manifestations, (3) negative aPL and aPL-related manifestations, and (4) negative aPL with no aPL-related manifestations. Our study was performed to explore these potential associations, each of which were a priori hypotheses; therefore statistical adjustments for multiple comparisons were not performed.
RESULTS
Study population
We collected data on 90 children with primary rheumatologic disorders, including 52 with SLE (58.4%), 21 with JIA (23.3%), 8 with JDM (8.9%), 3 with primary APS (3.4%), 3 with SS (3.3%), 1 with MCTD (1.1%), 1 with SSc (1.1%), and 1 with systemic vasculitis (1.1%). Median age was 16.5 years (range 5 to 21 yrs). In the study population, 72 were female and 18 were male. Self-reported race/ethnicity data were available in 67 participants: Hispanic (46.3%), African American (41.8%), white (9.0%), and Asian (3.0%). Of the 90 participants, 66 were taking HCQ at the time of data collection (73.3%). Mean A5R level for the group as a whole was 234% ± 45% (range 121% to 361%). When we analyzed data separately in the aforementioned risk groups, those with an underlying diagnosis of primary APS, SLE, and SLE-like illnesses had significantly higher prevalence of positive aPL, thrombotic events, and lower A5R levels as compared to the remainder of the group (Table 1).
Bivariate analysis of 90 children with rheumatic diseases. Continuous variables are represented as mean ± SD. Categorical variables are represented as frequencies (percentages).
Thrombotic events
Ten of the 90 patients were found to have a history of thrombotic events. Three of these patients had 1 or more recurrent thromboses leading to a total of 14 thrombotic events. Six events were deep venous thrombosis (DVT), 1 pulmonary embolism (PE), 4 had ischemic strokes, 2 involved arterial thromboses of major organs (liver, kidney), and 1 involved the small vessels of the skin and subcutaneous tissue. One patient met criteria for catastrophic APS. One patient had recurrent miscarriages beyond the 10th week of gestation. Of these patients with thrombotic events, 6 had an underlying diagnosis of SLE, 3 had primary APS, and 1 had an underlying diagnosis of MCTD. Potential comorbid risk factors for thrombosis were found in all of the 10 patients, including use of hormonal contraception (n = 2), pregnancy (n = 1), sickle cell anemia (n = 1), nephrotic syndrome (n = 2), obesity with body mass index > 35 (n = 3), smoking (n = 1), femoral venous catheterization (n = 2), prothrombin G20210A heterozygosity (n = 1), MTHFR homozygosity with normal homocysteine levels (n = 2), and coexistent lupus cerebritis (n = 2).
Transiently positive aPL
Twenty-one patients (23.3%) were found to have transiently positive aPL. Of these patients, 19 had SLE, 1 had SS, and 1 had systemic vasculitis. The most common transiently elevated aPL was aCL, seen in 19 patients (21.1%). LAC and anti-ß2GPI antibodies were less frequently transiently elevated, seen in 8 patients (8.9%) and 6 patients (6.7%), respectively. Overall, the presence of 1 or more transiently elevated aPL was not significantly associated with thrombosis (p = 0.999).
Persistently positive aPL
Persistently positive aPL were seen in 19 patients (21.1%), with 13 patients (14.4%) having persistently positive LAC, 10 patients (11.1%) persistently positive anti-ß2GPI antibodies, and 14 patients (15.6%) persistently positive aCL. Persistent positivity was seen only in patients with an underlying diagnosis of primary APS, SLE, and MCTD. Thrombosis was significantly associated with persistently positive aPL, with 7 of 10 patients with thrombotic events having 1 or more persistently positive aPL (p = 0.001).
Annexin A5 resistance and aPL
Patients with 1 or more persistently positive aPL had greater resistance to annexin A5 anticoagulant activity, as demonstrated by lower mean A5R = 203% ± 44% compared to those with transient aPL (mean A5R = 231% ± 55%) or no aPL (mean A5R = 247% ± 35%; p < 0.001). Similarly, when we evaluated individual aPL (LAC, anti-ß2GPI, and aCL), patients with persistently positive antibodies in each group had significantly lower mean A5R levels, compared to patients with negative aPL (Table 2). Further, 6 patients (6.7%) who were persistently positive for all 3 aPL (LAC, anti-ß2GPI, and aCL) had significantly reduced mean A5R (168% ± 41% vs 242% ± 42% in those with negative aPL; p < 0.001; Figure 3). There was no significant difference in mean A5R levels among patients with transiently elevated aPL compared to those with negative aPL, with the exception of aCL, with borderline statistical significance (Table 2).

Mean annexin A5 resistance in relation to number of antiphospholipid antibodies (aPL).
Mean annexin A5 resistance assay (A5R; %) in relation to antiphospholipid antibodies (aPL).
Annexin A5 resistance and thrombosis
Patients with a history of thrombosis (n = 10) had lower mean A5R levels compared to those without thrombosis: mean A5R = 207% ± 36% versus 237% ± 46% (p = 0.048). Comparing patients with persistently positive aPL and thrombosis versus those with neither, mean A5R was 206% ± 43% versus 244% ± 42% (p = 0.029). Interestingly, patients with persistently positive aPL without thrombosis and those with thrombosis but no aPL also had lower mean A5R levels: 200% ± 46% and 209% ± 23%, respectively.
DISCUSSION
In contrast to hereditary thrombophilias, pediatric APS can produce thrombosis in arteries, veins, and/or microvasculature, leading to a wide spectrum of clinical manifestations. In general, the incidence of thrombosis in children appears to be lower than that in adults, and aPL-associated manifestations are more common, including thrombocytopenia, livedo reticularis, Raynaud’s phenomenon, migraine, chorea, and epilepsy1,11,12. Although thrombosis is relatively infrequent in childhood, the potential consequences of a thromboembolic event, when it does occur, can be devastating. In the largest international registry of 121 cases of pediatric APS, cerebrovascular involvement (including cerebral ischemic stroke and cerebral sinus vein thrombosis) was present in 32% of patients, a higher percentage than previously reported in adults with APS12,13,14. Due to limited evidence regarding the prognostic implications of positive aPL, it is difficult to measure the risk of aPL-related thrombosis in children.
A significant body of evidence has accumulated supporting the hypothesis that antibody-mediated disruption of the anticoagulant annexin A5 shield may play a role in the underlying pathogenesis of aPL-mediated thrombosis and miscarriage4,5,7,8,9,10. Our study, unique in its evaluation of annexin A5 anticoagulant activity in children and adolescents with rheumatic diseases, is also novel in examining the relationship of annexin A5 in transient versus persistent aPL. We examined resistance to the anticoagulant effects of annexin A5 using the functional A5R assay developed by Rand, et al (Figure 2) and performed by laboratory technologists blinded to the patient’s clinical status2,3,9. We found that resistance to annexin A5 anticoagulant activity, as demonstrated by reduction of the A5R ratio, was strongly associated with the presence of persistently positive aPL in our patients, a finding that was similar to those previously reported in adults with APS2,9,10.
Even more noteworthy was the further reduction in mean A5R levels seen in patients with persistent positivity of multiple aPL. Studies have shown that patients with triple positivity of LAC, anti-ß2GPI, and aCL demonstrate substantially increased risk of thrombosis, pregnancy-related morbidity, and higher recurrence rates of clinical manifestations despite the use of oral anticoagulant therapy15,16. We speculate that alterations in annexin A5 anticoagulant activity may reflect the presence of aPL with higher avidity for phospholipids (both individually and collectively) that have increased likelihood of competing with the rapid binding of annexin A5 and disrupting its crystallization (Figure 1)2. These higher avidity antibodies may therefore be more likely to be pathologically associated with clinical manifestations.
When examining each of the persistently positive aPL subtypes, we found that LAC, anti-ß2GPI, and aCL were all associated with significantly reduced mean A5R, with the greatest reduction in mean A5R levels observed in patients with anti-ß2GPI antibodies. This finding is similar to reports correlating aPL-mediated disruption of annexin A5 with ß2GPI-dependent LAC17. In that report, a multistep mechanism was proposed for aPL-related thrombosis, suggesting that aPL binding to ß2GPI occurs after the molecule undergoes a conformational change that enables the antibodies to recognize aminoterminal domains on ß2GPI and to bind 2 molecules. This dimerized ß2GPI has a higher avidity for phospholipid and therefore can compete with the binding of annexin A5 to phospholipids, decreasing its protective anticoagulant effects and potentially increasing the risk of thrombosis17.
The mechanism described here may also explain why transient aPL, which may not require the presence of ß2GPI for binding, do not have sufficient avidity to compete with annexin A5 and therefore do not result in annexin A5 resistance or pathologic thrombosis. This issue is especially pertinent to the pediatric population, as there is an increased incidence of transient, nonpathogenic aPL following various viral and bacterial infections in healthy children18,19,20. In our study, 23% of patients were found to have nonpathologic transiently elevated aPL. In general, the presence of transiently elevated aPL was not significantly associated with reduced mean A5R levels. This finding supports the hypothesis that transient aPL may differ immunologically from the pathologically relevant aPL1.
We additionally evaluated our patients by comparing those at higher risk for aPL-related manifestations with those at lower risk. Thrombosis, aPL, and lower mean A5R levels were primarily seen in patients with primary APS, SLE, and SLE-like illnesses. Interestingly, in 1 patient with catastrophic APS, the mean A5R was strikingly decreased at 140%, which was among the lowest in the group. Evaluating patients with an underlying diagnosis of SLE separately, we found that these patients accounted for the majority of patients with positive aPL and thrombosis. Among the 52 patients with SLE, the rate of thrombosis was 12%, which is equivalent to reports in the literature1,18,21,22,23,24.
The majority of our patients (73.3%) were taking HCQ at the time of data collection, including 18 of the 19 patients with persistently positive aPL, thus limiting our ability to assess the association between HCQ and A5R. Prior studies have shown that HCQ may be protective in reducing the risk of thrombosis in patients with SLE and persistently positive aPL25,26,27. In addition, Rand, et al recently demonstrated a modest but statistically significant increase in mean A5R levels in the presence of HCQ in patients with positive aPL28. Although current evidence-based guidelines do not recommend the use of HCQ in the primary or secondary prevention of thrombosis in APS, controlled studies are needed to further examine the potential role of this medication in the underlying pathogenesis of aPL-mediated thrombosis29,30.
Several limitations of our study need to be addressed. The first is our relatively small although well defined sample, with only 10 patients having a history of thrombotic events. Also, although documented by radiographic imaging, all events were collected through retrospective chart review, which has the inherent possibility that some of the factors surrounding the event and temporal association with aPL may have been limited. In addition, the absence of a pediatric-specific A5R reference range in disease-free donors limits the full interpretation of these findings. Finally, in reviewing potential thrombotic risk factors, all 10 patients with thrombosis were found to have at least 1 potential comorbid risk factor. It is unclear to what extent these potential prothrombotic risk factors may have contributed to the thrombotic events; however, it is consistent with other reports and supportive of the hypothesis that the underlying pathogenesis surrounding APS may be multifactorial31.
We have demonstrated that children and adolescents with rheumatic diseases and persistent aPL demonstrate lower annexin A5 anticoagulant activity, whereas transient, nonpathogenic aPL have less effect on annexin A5 activity. We have further shown that children with a history of thrombotic events may also demonstrate reduced A5R. In collaboration with the Atherosclerosis Prevention in Pediatric Lupus Erythematosus trial, sponsored by the Childhood Arthritis and Rheumatology Research Alliance, we plan to expand these findings into a larger, multicenter study of children with SLE to better evaluate the association between resistance to annexin A5 anticoagulant activity and aPL-related clinical manifestations.
Acknowledgment
The authors acknowledge Aileen McGinn for her assistance with the statistical analysis and editing, as well as the laboratory services provided by Dr. Xiao Xuan Wu, Mojgan Raoufi, and Julissa Pena-Medina.
Footnotes
-
Supported by a grant from the New York Chapter of the Arthritis Foundation; and by the Clinical and Translational Science Awards Grant UL1 RR025750 and KL2 RR025749 and TL1 RR025748 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Development of the annexin A5 resistance assay was made possible by NIH National Heart, Lung and Blood Institute (NHLBI) R01HL061331 and NIH NHLBI RC1HL101031. The contents are solely the responsibility of the authors and do not necessarily represent the official view of the NCRR or NIH.
- Accepted for publication August 15, 2011.








{kind=link}
{kind=link}
{kind=link}