
Abstract
Objective. Platelet aggregation plays a major role in vascular mortality. Individuals with psoriatic arthritis (PsA) are highly predisposed to vascular mortality. We evaluated the correlation between disease activity and platelet aggregation in individuals with PsA.
Methods. Individuals with PsA receiving tumor necrosis factor-α (TNF-α) blockers (n = 114) and healthy controls (n = 114) matched for age, sex, and cardiovascular risk factors were tested for light transmission aggregometry. None was receiving antiinflammatory drugs. Platelet aggregation (max-A%) was defined as maximal light transmittance achieved within 5 min after the addition of 0.1 or 0.2 mM arachidonic acid or 0.4 μM adenosine diphosphate. A value of ≥ 50% irreversible light transmittance (LT-50%) following platelet stimulation was used to define platelet hyperreactivity. Minimal disease activity (MDA) was evaluated in subjects with PsA.
Results. Regardless of the agent used, individuals with PsA showed a higher max-A% and achieved LT-50% more often than controls. Among individuals with PsA, those achieving MDA exhibited a max-A% similar to that of controls, both being significantly lower (p < 0.001) than max-A% of subjects with active disease. Subjects with active disease showed platelet hyperreactivity (LT-50%) more often than those achieving MDA (p < 0.001). For increasing quartiles of max-A%, C-reactive protein levels increased and prevalence of MDA decreased.
Conclusion. Compared with those achieving MDA, subjects with active PsA disease had abnormally high platelet reactivity. Whether this is relevant for the cardiovascular risk profile of subjects with PsA receiving TNF-α blockers requires further evaluation.
- PSORIATIC ARTHRITIS
- PLATELET AGGREGATION
- TUMOR NECROSIS FACTOR-α BLOCKERS
- TREATMENT
Individuals with psoriatic arthritis (PsA) are predisposed to atherosclerotic vascular mortality1. Platelets link atherosclerosis with inflammation2. Little is known about disease activity and platelet aggregation in subjects with PsA receiving tumor necrosis factor-α (TNF-α) blockers.
MATERIALS AND METHODS
Among those referred to our outpatient clinic, 114 individuals with PsA (criteria of the CASPAR Study Group3) receiving TNF-α blockers for ≥ 1 year were enrolled in our study. Healthy individuals (n = 114) matched for age, sex, and cardiovascular risk factors4 served as controls. Exclusion criteria included a history of coronary artery disease, receiving active antiplatelet treatment [including nonsteroidal antiinflammatory drugs (NSAID)], serum creatinine > 140 mmol/l, platelet count < 120,000/ × 109/l, and liver enzymes more than twice the upper limit of normal5.
The clinical subset (Moll and Wright criteria6) and the achievement of a sustained (> 1 year) minimal disease activity (MDA)7 were evaluated in each PsA subject.
The maximal light transmittance (Chrono-Log; Mascia Brunelli, Milan, Italy) achieved within 5 min after the addition of 0.1 and 0.2 mM arachidonic acid (AA) or of 0.4 μM adenosine diphosphate (ADP) was defined as max-A%8. A value of ≥ 50% irreversible light transmittance (LT-50%) defined the platelet hyperreactivity9.
Continuous data were expressed as means ± SD, categorical variables as percentages. Continuous variables were compared by an independent sample T test and by ANOVA analysis. Correlations were assessed by Pearson’s linear correlation coefficients (r). The chi-square test with Fisher’s exact test was performed for categorical data.
RESULTS
Major characteristics of case and control subjects are reported in Table 1.
Demographic and clinical features of the study population. Data are mean ± SD unless otherwise specified.
No subject with PsA was receiving traditional disease-modifying antirheumatic drugs. Adalimumab therapy was employed in 44 subjects (35.6%), etanercept and infliximab in 35 each (30.7%).
PsA subjects achieved LT-50% more often than controls following exposure to ADP 0.4 μM (33.3% vs 14.0%, respectively; p = 0.001) or to AA 0.1 mM (33.3% vs 10.5%; p < 0.001) or to AA 0.2 mM (68.4% vs 19.3%; p < 0.001). Max-A% was higher in PsA subjects than in controls as well (AA 0.1 mM: 54.50% ± 16.10% vs 45.28% ± 10.93%; p < 0.001; AA 0.2 mM: 68.14% ± 18.45% vs 48.32% ± 11.79%; p < 0.001; ADP 0.4 μM: 51.15% ± 20.68% vs 36.49% ± 14.49%; p < 0.001).
Achievement of LT-50% in the 40 PsA subjects with MDA was comparable to that of controls and lower than that of subjects with active disease (Figure 1A). Similarly, max-A% values of those with MDA were comparable to controls and were lower than those of individuals with active disease (Figure 1B).

Platelet aggregation in response to different aggregating agents in PsA. A. Achievement of LT-50% in the 40 PsA subjects with MDA was comparable to that of controls and lower than that of subjects with active disease. B. Max-A% values of those with MDA were comparable to controls and were lower than those of individuals with active disease. AA: arachidonic acid; ADP: adenosine diphosphate; LT-50%: irreversible light transmittance ≥ 50%; MDA: minimal disease activity.
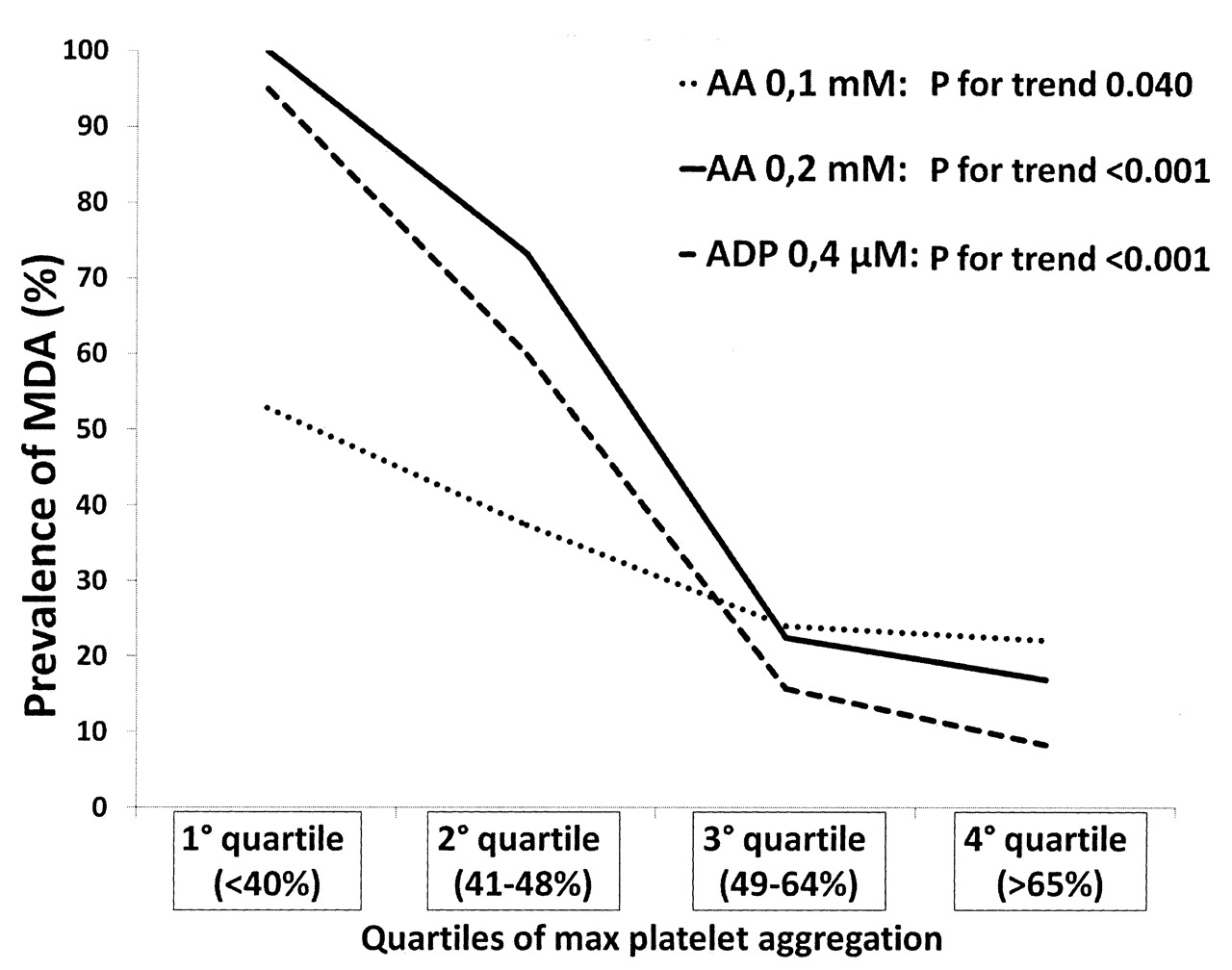
C-reactive protein (CRP) values were lower in subjects with MDA than in those with active disease (1.98 ± 1.8 vs 3.6 ± 3.9; p = 0.007). CRP values showed a direct correlation with max-A% (AA 0.1 mM: r = 0.360, p < 0.001; AA 0.2 mM: r = 0.278, p = 0.003; ADP 0.4 μM: r = 0.224, p = 0.018) and with max-A% quartiles (AA 0.1 mM: r = 0.446, p < 0.001; AA 0.2 mM: r = 0.216, p = 0.022; ADP 0.4 μM: r = 0.209, p = 0.027). The prevalence of MDA decreased for increasing quartiles of max-A% (Figure 2).
{kind=link}
{kind=link}
Prevalence of MDA according to quartile of maximum aggregation in response to different agonists (AA 0.1 mM, AA 0.2 mM, ADP 0.4 μM). AA: arachidonic acid; ADP: adenosine diphosphate; MDA: minimal disease activity.
DISCUSSION
Our study shows that platelet function is increased in patients with PsA, especially in those with poorly controlled disease. The correlation of CRP with max-A% and the decreasing prevalence of MDA for increasing quartiles of max-A% argue for a link between inflammation and platelet reactivity. By interacting with specific platelet receptors, cytokines/chemokines involved in PsA10 cause intracellular calcium mobilization, nucleotide secretion, and platelet activation11. Hyperreactivity to ADP has been reported in rheumatic diseases5. However, almost 50% of patients in that sample were receiving NSAID12 and only 17% had PsA.
Platelet hyperreactivity was correlated with an elevated incidence of arterial thrombosis13,14, and the effect of antiplatelet agents in the vascular risk profile of subjects with PsA requires investigation5. Our data show that inflammation influences platelet reactivity and that achievement of minimal disease activity may normalize platelet hyperreactivity.
Acknowledgment
The authors thank all members of the CaRRDs Study Group for collaboration and support in the literature search and the organization of the study; and Dr. Anna Lilia Ruocco and Dr. Fabrizio Giello, Department of Clinical and Experimental Medicine, Federico II University, for performing platelet aggregation tests.
- Accepted for publication September 15, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.