
Abstract
Objective. Autologous stem cell transplantation (aSCT) for systemic sclerosis (SSc) has been shown to be effective in recent reports. This aggressive approach and the disease itself are associated with a high mortality. We report our experiences in 26 consecutive patients.
Methods. Between 1997 and 2009, 26 patients were scheduled for aSCT. Our standard transplant regimen consists of cyclophosphamide (CYC) and granulocyte colony-stimulating factor (GCSF) for mobilization and CYC plus antithymocyte globulin for conditioning before the retransfusion of CD34 selected stem cells. The major outcome variable was the response to treatment [reduction of modified Rodnan skin score (mRSS) by 25%] at Month 6. Secondary endpoints were the transplant-related mortality and the progression-free survival.
Results. Significant skin and lung function improvement of the mRSS was achieved in 78.3% of patients at Month 6. The overall response rate was 91%, as some patients improved even after Month 6. Three patients died between mobilization and conditioning treatment, 2 due to severe disease progression and 1 whose death was considered treatment-related (i.e., GCSF or CYC toxicity). Depending on definitions, transplant-related mortality was 4% and treatment-related mortality 11%. Seven patients experienced a relapse during the 4.4 years of followup. The progression-free survival was 74%. Four patients died during followup and the most frequent causes of death were pulmonary and cardiac complications of SSc.
Conclusion. aSCT led to significant improvement in most patients with SSc. The procedure requires further optimization; hence we are modifying our screening and treatment strategy. To minimize infectious complications, CYC for mobilization and GCSF were reduced. We intensified our screening for cardiac involvement and modified our conditioning regimen in case of cardiac involvement.
- SYSTEMIC SCLEROSIS
- STEM CELL TRANSPLANT
- TREATMENT
- CYCLOPHOSPHAMIDE
- CD34 SELECTION
- GRANULOCYTE COLONY-STIMULATING FACTOR
Systemic sclerosis (SSc) is an autoimmune disease with high mortality and very few therapeutic options. In addition to the skin, the disease may affect almost every organ. Its pathogenesis remains unknown, but the ultimate endpoint is fibrosis. With respect to the expansion of skin involvement, SSc is subdivided into limited and diffuse cutaneous subsets (lcSSc/dcSSc). To date, treatment aims at ameliorating the main organ manifestations, but not at general improvement or even termination of fibrosis or the process leading to it. Hence, the treatment recommendations of the European League Against Rheumatism (EULAR)1 focus on the SSc-related individual manifestations, e.g., digital ulcers or pulmonary arterial hypertension (PAH).
Myeloablative or lymphodepleting therapies with autologous or allogeneic stem cell support are promising treatment strategies in autoimmune diseases. Since EULAR created a registry for autoimmune diseases together with the European Group for Blood and Bone Marrow Transplantation in 19962 several reports on the efficacy in different autoimmune diseases and especially in SSc have been published3,4,5,6,7. One randomized trial was published recently8 proving the superiority of autologous stem cell transplantation (aSCT) to cyclophosphamide (CYC) pulse therapy in a small cohort of patients, as the trial was terminated early due to superiority of the transplant arm. Further randomized European (ASTIS trial) and American (SCOT trial) studies are under way9. Due to its lower toxicity, aSCT is generally preferred over allogenic stem cell transplantation.
This is a retrospective analysis of our experiences with aSCT in SSc.
MATERIALS AND METHODS
All patients with SSc who were considered for aSCT between November 1997 and October 2009 were included in our analysis. Twenty-six patients were scheduled for aSCT as a rescue therapy. Indication for aSCT was either inefficacy of CYC or rapidly progressive diffuse disease with strong indicators for a bad prognosis (positivity for Scl-70 antibodies, rapid progression of skin/organ manifestations, diffuse cutaneous form, male sex, alveolitis, early PAH)8,9,10,11,12,13,14,15. Major exclusion criteria were a Karnofsky index < 70%, PAH with systolic pulmonary arterial pressure > 50 mm Hg, and DLCO < 40%. Before transplantation, all patients received pulmonary function tests, high-resolution computed tomography (HRCT) scans, and echocardiography as well as an electrocardiogram (ECG). In case of PAH on echocardiography, a right heart catheterization was added.
Medication
A nonmyeloablative protocol, an adaptation of protocols for severe aplastic anemia16, was used. A similar protocol was used for the ASTIS trial9 in Europe, as follows. Mobilization: CYC 2 g/m2 (Days 1 + 2) and granulocyte colony-stimulating factor (GCSF) with 10 μg/kg/day filgrastim starting Day 7. Leukapheresis and CD34 selection of the stem cell harvest: usually 10 days after the mobilization therapy. Conditioning: CYC 4 × 50 mg/kg body weight (Days −5 to −2) plus 4 × 10 mg/kg rabbit antithymocyte globulin (ATG; Days −4 to −1). Transplantation of CD34-positive stem cells on Day 0.
For CD34 purification, cells were positively selected using immunomagnetic beads with an anti-CD34 monoclonal antibody (CliniMACS, Miltenyi Biotec, Cologne, Germany). The median purity and recovery after CD34 selection were 94.5% (range 41.0%–99.1%) and 70.7% (range 46.8%–99.4%), respectively.
Additional immunosuppressive therapy was discontinued before pretransplant conditioning. All patients received acyclovir, levofloxacin, fluconazol, and trimethoprim-sulfamethoxazole for infection prophylaxis.
Outcome measures
Primary endpoint was response to treatment at Month 6, defined as 25% improvement of the modified Rodnan skin score (mRSS) until Month 6. In addition, pulmonary function tests with measurement of DLCO (percentage of predicted) and the inspiratory vital capacity (percentage of predicted) were assessed. Erythrocyte sedimentation rate (ESR; mm/h) and C-reactive protein (CRP; mg/dl) served as laboratory indicators. Disease progression and relapse were defined as any worsening of skin fibrosis or decrease of DLCO with new ground-glass pattern as a sign for alveolitis in HRCT scans after transplantation.
Major secondary outcome measures were the 100-day transplant-related mortality, defined as death without relapse or progression of autoimmune disease as usually used in hematological reports on transplantation for malignancy or hematological disorders, and as applied by the European Group for Blood and Marrow Transplantation Working Party on Autoimmune Diseases3, as well as the treatment-related mortality, defined as any death within 100 days after treatment and the progression-free survival, defined as survival without mortality, relapse, or progression of SSc.
Neutrophil and platelet engraftment was defined as the first day after transplantation when the absolute neutrophil count was > 500 cells/μl and > 20,000 platelets/μl without platelet transfusion, respectively.
Statistics
All data are reported in median values with minimum/maximum range or mean values with SD. SPSS version 18.0 (SPSS, Chicago, IL, USA) was used for statistical analyses with Wilcoxon test for differences between baseline and followup. A p value < 0.05 was considered statistically significant. Progression-free survival and overall survival were calculated using the Kaplan-Meier estimate, with the mobilization therapy as starting point.
RESULTS
Patients and treatment
For patient characteristics see Table 1. Twenty-six patients (18 women/8 men) with either lcSSc (n = 2) or dcSSc (n = 24) were included. The median age at the time of the decision for aSCT was 39 years (range 19–65 yrs), the median disease duration was 2.25 years (range 1–6.5 yrs). Nineteen patients tested positive for Scl-70 antibodies. Twenty-five patients were mobilized with CYC/GCSF; in 1 patient who had intolerance for CYC, direct bone marrow aspiration without CD34 selection was used after unsuccessful mobilization treatment with GCSF alone. Melphalan was substituted for CYC for conditioning in this patient. In 1 case of severe cardiac involvement (ventricular arrhythmia Lown class IV in 24-hour ECG and fibrosis in the myocardial biopsy), CYC was reduced to 2 × 50 mg/kg and partially substituted by thiotepa (2 × 5 mg/kg) as described17,18 to reduce cardiotoxicity. A quantity of CD34-positive cells, median 3.9 × 106 cells/kg (range 2.3–9.2), was transplanted with a median proportion of remaining CD3-positive T cells of 0.25 × 104 cells/kg (range 0.07–2.22; n = 20) after CD34 selection.
Demographic data of the patients (n = 26) at the time of decision for autologous stem cell transplant and outcome.
Side effects and engraftment
Three patients died during or shortly after the mobilization. One patient died due to aspiration in consequence of a severe disease progression with intestinal dysfunction and renal crisis. One woman presented with fever in aplasia 8 days after mobilization. Despite antiviral, antibiotic, and antifungal treatment and neutrophil regeneration, she died at Day 14 due to respiratory failure. Histopathology revealed a massive progression of SSc with fresh interstitial pulmonary and myocardial fibrosis (Figure 1). The third patient succumbed to pulmonary failure as a consequence of severe leukostasis, leukocyte infiltration, and alveolar hemorrhage 11 days after mobilization. This death was considered treatment-related since an autopsy ruled out an infectious cause and histopathology showed diffuse interstitial and intraalveolar granulocyte accumulations, due most probably to GCSF treatment. Alternatively, CYC toxicity was also considered. In 2 additional patients, similar noninfectious pulmonary leukocyte infiltrations appeared during GCSF treatment 11 and 12 days after CYC therapy, requiring therapy in the intensive care unit in both cases. Both recovered without sequelae under high-dose steroids and assisted ventilation. Twelve patients had fever during aplasia; in 7 patients an infectious focus could be identified, but none required intensive care treatment. Four patients had a severe cytokine release during ATG therapy, with severe chilling and hypotension; in 2 cases the ATG therapy had to be stopped ahead of schedule. No other serious adverse event occurred. Neutrophils and platelets engrafted at a median of 11 (range 8–16) and 12 (range 5–23) days after aSCT, respectively.
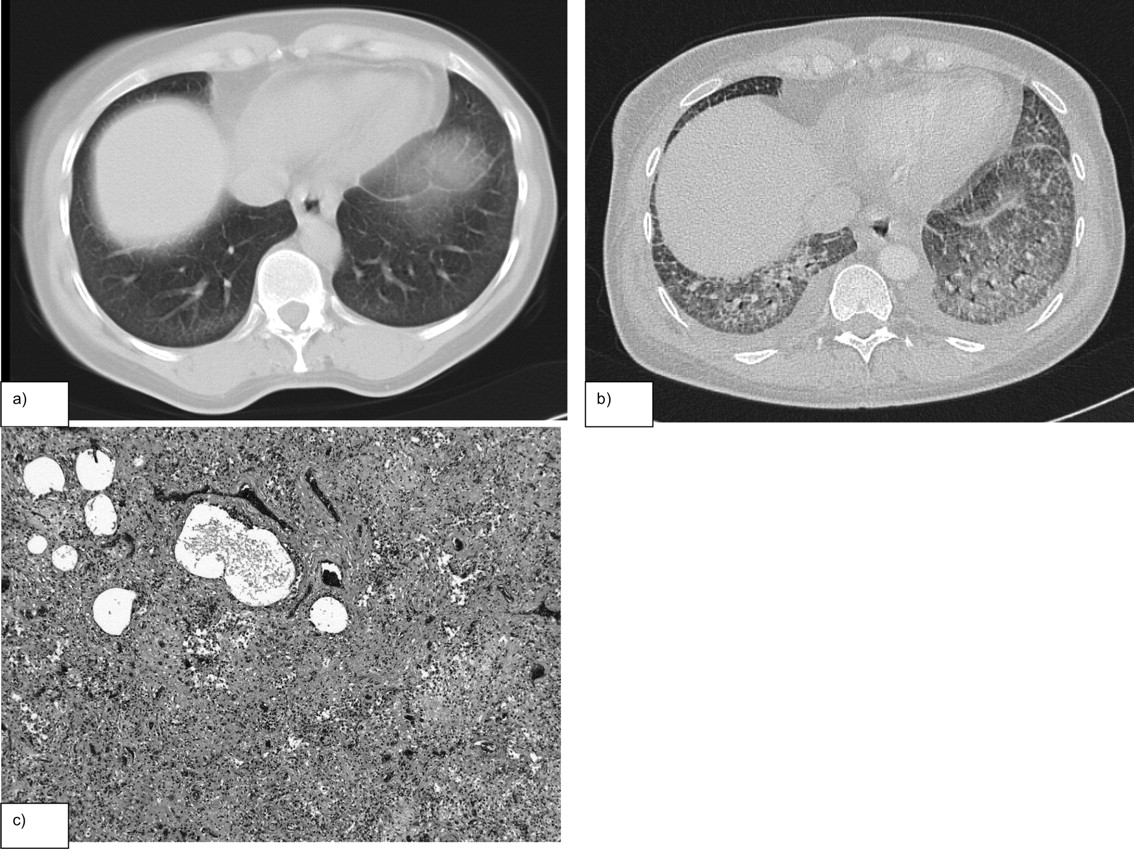
Patient 23: thoracic computed tomography scan (a) before and (b) shortly after mobilization therapy with CYC/GCSF showing diffuse pulmonary infiltration after treatment. There was no evidence for bacterial, viral, or fungal infection. Differential diagnosis included CYC toxicity, GCSF toxicity, and disease progression. Autopsy revealed massive progression despite mobilization therapy. Panel (c): corresponding H&E stain of the lung shows noninfectious alveolitis and severe fibrosis. CYC: cyclophosphamide; GCSF: granulocyte colony-stimulating factor.
No transplanted patient died within 100 days after aSCT. Transplant-related mortality as defined above excluded the 2 patients who died due to progression of SSc, and therefore is considered 4%. Treatment-related mortality includes all 3 patients who died shortly after mobilization and thus was 11%.
Response to treatment
Of the 23 transplanted patients, 78.3% (n = 18) had improvement of > 25% of the mRSS at Month 6. The mean mRSS was 18.2 (SD ± 7.9) at baseline, 11.2 (± 7.0) at Month 6, and 9.3 (± 6.5) at Month 12; both reductions were statistically significant (p < 0.0001). Mean ESR and CRP declined significantly by Month 6 after aSCT from 37 mm/h (± 25.4) to 21 mm/h (± 19.9; p = 0.04) and 3.5 mg/dl (± 5.0) to 1.1 mg/dl (± 1.6; p = 0.026), respectively. DLCO was nearly unchanged during followup, with a mean value of 58.3% (± 20.6%) at baseline, 57.0% (± 14.0%) at Month 6, and 61.4% (± 13.0%) at Month 12; but mean inspiratory vital capacity improved significantly: 66.0% at Month 6 (n = 21) and 76.1% at Month 12 (n = 17; p = 0.02; Figure 2). This improvement went along with skin improvement in all patients. Of the 5 patients who did not reach the response criterion at Month 6, 3 patients showed a marked skin improvement with no further progression of organ damage during the course of disease. These 3 patients were regarded as late responders to aSCT. The remaining 2 patients had disease progression; 1 had to go for dialysis 2 months after aSCT due to a renal crisis and 1 died due to severe cardiac involvement and fatal arrhythmias.
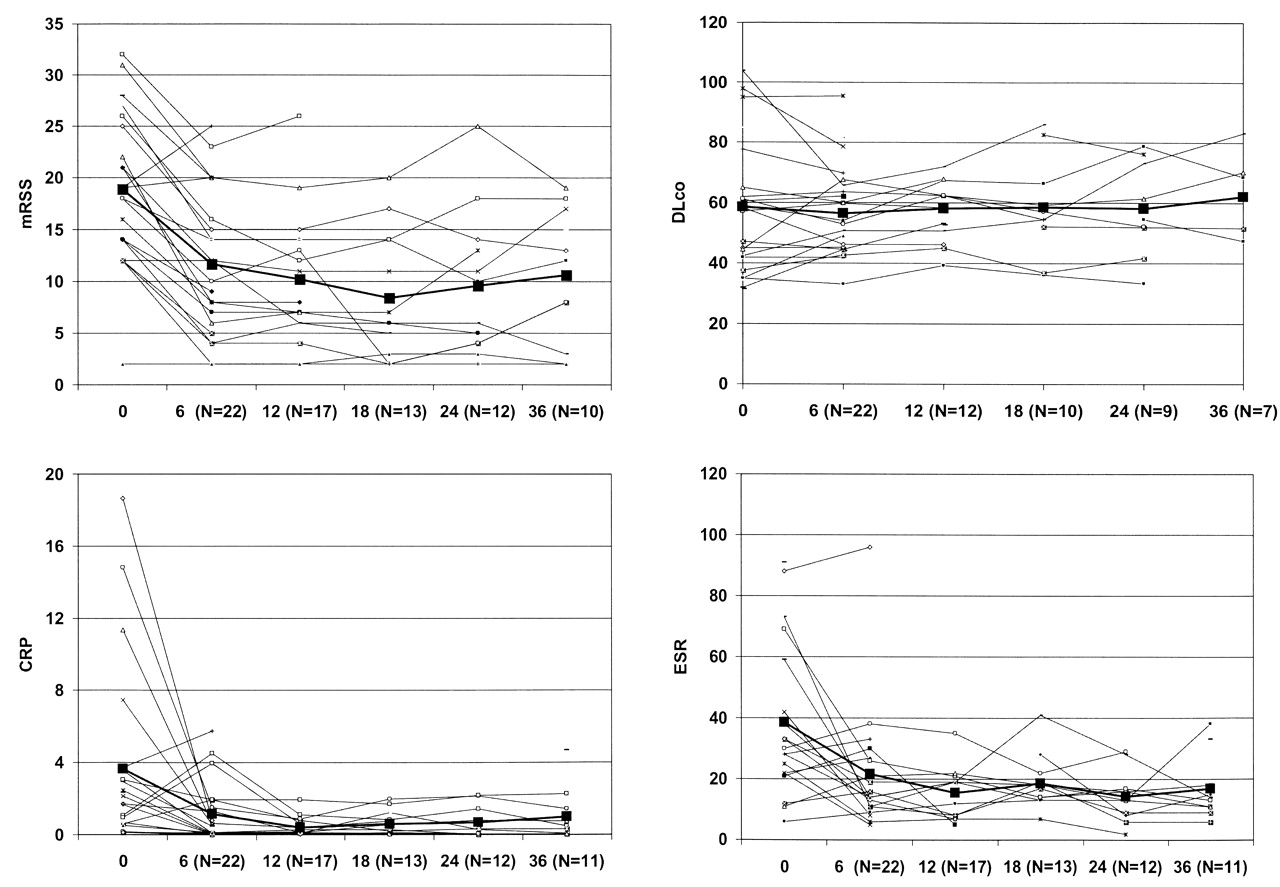
Modified Rodnan skin score (mRSS), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and DLCO at baseline and during followup showing a sustained reduction in mRSS, CRP, and ESR and stabilization in DLCO after aSCT. Black line indicates mean values.
Followup to treatment
Two patients, both with response to treatment, were lost to followup after 0.2 years and 4.6 years, respectively. During the median followup of 4.4 years (range 1.1–12.2 yrs), 7 major relapses occurred in the 21 patients with response to aSCT after a median of 16 months (range 5–33 mo). Five of the patients (71%) who relapsed were men. Hence 5 of 8 men relapsed versus 2 of 18 women (62.5% vs 11.1%, respectively). In 2 patients an aggravation of skin fibrosis as well as a relapse of myositis/fasciitis manifested after 5 months. Both patients died in the further disease course. Three patients presented with active alveolitis after 14, 15, and 18 months. Rituximab and mycophenolate mofetil were used in 1 and CYC pulses in the other 2 to halt disease progression. One patient relapsed with a renal crisis and progression of the skin fibrosis 19 months after initially very effective aSCT. He died 1 year later, due most probably to fatal arrhythmias. One patient presented after 31 months with morphea as a secondary autoimmune disease and new-onset erosive arthritis, most probably SSc-related (negative for rheumatoid factor and anticitrullinated protein antibodies), which were effectively treated with methotrexate. The patient who was transplanted using the regimen with thiotepa experienced a significant improvement of the skin but relapsed with alveolitis after 18 months. A cardioverter defibrillator was implanted to protect him from arrhythmia and no further reduction of ventricular function was observed after the transplant.
Three years after aSCT, overall survival and progression-free survival probabilities estimated from Kaplan-Meier plots were 74% and 53%, respectively (Figure 3). Altogether 7 (27%) of the initial 26 patients considered for transplants died during followup or transplantation; nevertheless, 14 patients remain in remission with no signs of disease activity up to 13 years after aSCT.

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier plot showing the overall survival and the progression-free survival starting with mobilization. Censor events are marked.
DISCUSSION
Autologous hematopoietic stem cell transplantation proved effective in our patients, with a significant reduction of the mRSS as well as the ESR and CRP. Inspiratory vital capacity improved at Month 6, showing a marked influence even on the pulmonary function. These findings are consistent with the experiences from other groups4,7,8. The positive results encourage holding to this aggressive approach in SSc treatment, while remaining aware of the possible side effects of severe immunosuppression.
Progressive diffuse SSc with multiple organ involvement is associated with a significant mortality of 40% to 50% in 5 years12,13,15. More recent data describe a 5-year mortality rate of 35% in patients with rapid skin progression14. The total of 7 deaths in our 26 patients during the 4.4 years of followup is thus less than expected in this negative selection. We are very interested in reducing the relatively high mortality. Therefore we critically analyzed the patients with fatal outcome. Excluding the patient whose death was most probably treatment-related, 6 of 25 (24%) of the patients died due to complications of SSc. The main causes of death were fatal arrhythmias and pulmonary failure even in patients successfully transplanted and thought to be in remission according to the measurable data. Similar experiences were reported in other SSc cohorts19,20. As reported recently, patients are at higher risk for severe kidney injury after aSCT for SSc21. In our cohort, 2 patients had renal crisis after aSCT. One who developed renal crisis within 2 months after aSCT had a very aggressive form of SSc, with no response to the conditioning regimen. Additional renal injury through toxic effects of the treatment could not be ruled out, but due to the very progressive development, the underlying disease seems more likely. The other patient had a relapse more than 1.5 years after aSCT, thus no correlation to aSCT treatment was assumed. Both patients had received therapy with angiotensin-converting enzyme inhibitor.
Destruction of the self-reactive immune system and the subsequent reconstitution of a new, self-tolerant immune system are considered to be the mechanism underlying the success of high-dose chemotherapy and aSCT. There is still uncertainty which substances and regimes are optimal to prepare a patient for a new immune system. To reduce the side effects and transplant risks, most centers use lymphoablative instead of myeloablative regimens in autoimmune diseases5. CYC treatment is well established in therapy of SSc and the only substance with proven efficacy in randomized trials22,23, therefore it was clearly the choice for both mobilization and conditioning in aSCT for SSc. To reduce the risk of reinfusion of autoreactive lymphocytes we chose a protocol with in vitro CD34 selection in addition to in vivo lymphocyte depletion with CYC plus ATG therapy. As we demonstrated24, the immune system in patients with SSc shows a shift in B and T cells toward a naive phenotype after lymphocyte depletion and aSCT, supporting the notion of “resetting” the immune system. We decided to maintain our regimen with CYC/ATG and CD34 selection although CD34 purification is associated with a significant reduction in T cells, natural killer cells, and monocytes, and thus with an increase of infectious complications. None of our patients died due to severe infections after conditioning.
From our experiences with the first 26 patients we are presently modifying our protocol. In order to reduce fatal arrhythmias we intensified our screening for cardiac involvement. Every patient planned for aSCT will receive a 24-hour ECG, stress echocardiography, assessment of brain natriuretic peptide and troponin25, and right heart catheterization with an additional myocardial biopsy, if pathologies are found by laboratory and clinical investigations. Consequently, patients with cardiac involvement will undergo transplant only under the protection of an implantable cardioverter defibrillator. In addition, those patients will receive a conditioning regimen with thiotepa and a reduced CYC dose to diminish CYC-induced cardiotoxicity. To shorten the period of neutropenia and thus infectious complications as well as cardiac and pulmonary toxicity, we also reduced CYC for mobilization to 2 × 1 g/m2 or 2 × 1.5 g/m2, respectively. Pulmonary adverse events during GCSF treatment, especially neutrophilic hemorrhagic alveolitis, are rare, but have been reported even in healthy donors and especially in patients with underlying pulmonary pathologies26,27. We consider that leukostasis and leukocyte congestion in the injured lung during GCSF treatment and hematopoietic regeneration in addition to active alveolitis are responsible for the acute respiratory failure in 3 of our patients; thus oral prednisolone 15 mg/day during the period of GCSF treatment was added to a higher dose of 2 × 1.5 g/m2 CYC. In addition, the GCSF dose was reduced and started earlier, on Day 5 of mobilization in all patients.
The biggest challenge remains the improvement of screening and use of new diagnostic tools to identify those patients at risk for transplant-related mortality and those who will most probably benefit from early transplantation.
Due to the retrospective design of our analysis and the small number of patients, the general implications of these results are limited. However, in a rare disease such as SSc, single-center experiences are helpful to identify differences in outcome and to optimize future protocols. Transplant-related mortality in aSCT varies widely in different centers3,9 and therefore an exchange of experiences is important. It is hoped that results of the randomized phase 3 trials with more than 100 patients in Europe (ASTIS) and the United States (SCOT) that are expected for 2012 will emphasize the efficacy of this treatment approach and help to reduce the concerns about safety.
We hope to contribute with our critical analysis and our recommendation for protocol adaptations to optimize aSCT for treatment of SSc. Protocols for aSCT worldwide remain under development and modifications are needed for SSc subgroups, such as for patients with active alveolitis or cardiac involvement.
- Accepted for publication September 15, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.