
Abstract
Objective. To compare the performance of the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) criteria with the 1987 American Rheumatism Association (ARA) criteria for rheumatoid arthritis (RA) in an early arthritis cohort.
Methods. The study included 79 patients with early arthritis (symptoms < 12 months) and a minimum of 1 year of followup between January 2004 and August 2010. Case notes were reviewed to determine which criteria were fulfilled at initial, 3-month, 1-year, and 2-year visits. Requirements for disease-modifying antirheumatic drug (DMARD) therapy and presence of joint erosions were compared at 2 years.
Results. At the initial visit, twice as many patients fulfilled the 2010 criteria (67%) compared with the 1987 criteria (34%; p < 0.001). Forty-four percent of patients who fulfilled only the 2010 criteria at the initial visit went on to fulfill both 1987 and 2010 criteria at 3 months (p < 0.001). Eight patients did not meet the 1987 RA criteria solely because of short symptom duration. All 17/79 patients who developed joint erosions went on to eventually fulfill both criteria. Of those patients who fulfilled only the 2010 criteria at baseline, 25/27 (93%) ultimately received DMARD therapy compared with 24/26 (92%) of those fulfilling both 1987 and 2010 criteria.
Conclusion. The 2010 ACR/EULAR RA criteria allowed earlier RA classification compared to the 1987 ARA criteria, although both criteria were equivalent in predicting joint erosions and subsequent need for DMARD (Australian New Zealand Clinical Trials Registry ANZCTR 12608000292370).
- RHEUMATOID ARTHRITIS
- CLASSIFICATION
- CRITERIA
- 2010 ACR/EULAR
- 1987 ARA
- EARLY ARTHRITIS
Rheumatoid arthritis (RA) is a progressive deforming erosive arthropathy that can lead to severe functional disability. Recognition and management of RA at an early stage is known to result in better longterm radiographic and functional outcomes1. However, predicting those patients who are likely to develop persistent and/or erosive disease that requires early disease-modifying antirheumatic (DMARD) therapy is a challenge. The American Rheumatism Association (ARA) 1987 RA classification criteria were developed to distinguish established RA from other arthropathies2. However, they have been criticized for lack of sensitivity in identifying patients with early RA. A literature review and metaanalysis found the 1987 ARA criteria to have a sensitivity of 77% and specificity of 77% in predicting RA in early arthritis3. With advances in therapeutic management for RA in the last decade, there is a need for clinical trials in patients with RA at an early stage of disease, but this is hampered by the lack of criteria to classify these patients. In response, the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) RA classification criteria were developed to stratify and standardize patient recruitment into clinical trials, to facilitate study at an earlier disease stage4. The aim of the new classification criteria is to identify earlier those patients who are likely to develop persistent erosive disease.
The authors of the 2010 criteria acknowledge that the new criteria will probably increase heterogeneity. The 2010 criteria thus propose a new model for the entity of RA and redefine RA itself. The aim is to move away from the previous concept of an established RA entity and to focus on early RA instead.
The aim of our study was to compare the performance of the 2010 ACR/EULAR criteria with the 1987 ARA criteria in an early arthritis cohort in New Zealand. We also wished to determine which specific variables in the 2010 criteria allowed earlier criteria fulfillment.
MATERIALS AND METHODS
The Early Arthritis Study at Christchurch Hospital, New Zealand, was established in 2004 to assess patients with symptoms of inflammatory arthritis (inflammatory joint pain and stiffness) of < 12 months duration and at least 1 swollen joint. The study was registered by the Australian New Zealand Clinical Trials Registry (ANZCTR 12608000292370) and received ethical approval from the Upper South A Ethics Committee, New Zealand. Written informed consent was obtained from all patients.
Patients were seen every 3 to 6 months for the first year and then at least annually. Standard demographic data were collected including age, sex, ethnicity, and smoking history. Joint assessment using a 44-joint count was undertaken. Disease activity was measured using the 28-joint Disease Activity Score (DAS28). Routine laboratory tests at each visit included full blood count, liver function tests, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Rheumatoid factor (RF) and anticitrullinated protein antibodies (ACPA) were measured at initial and 1-year visits. Radiological assessment of hands, wrists, and feet was performed annually. Medications including DMARD, nonsteroidal antiinflammatory drugs, and corticosteroid use were recorded at each visit.
Patients with a minimum of 1 year of followup between January 2004 and August 2010 were included in the current analysis. Patients other than those with a definitive diagnosis of RA or undifferentiated inflammatory arthritis (UIA) at the initial study visit were excluded. Case notes were retrospectively reviewed to determine fulfillment of the 1987 ARA2 and 2010 ACR/EULAR RA criteria at initial, 3-month, 1-year, and 2-year visits4 (Appendix 1). Patients who did not fulfill either the 1987 or the 2010 RA classification criteria and did not fulfill criteria for an alternative diagnosis were classified as having UIA. Diagnosis, requirement for DMARD therapy, and presence of joint erosions were compared at 2 years. Patients were defined as having a self-limiting inflammatory arthritis if at the end of the followup period they had no clinical evidence of synovitis, no radiological evidence of joint erosion, and did not require DMARD or ongoing corticosteroid therapy. Factors determining earlier fulfillment of the 2010 RA criteria were identified by comparing fulfillment characteristics of both sets of RA criteria in patients who met only the 2010 RA criteria at initial visit. Criteria compared were duration of symptoms, joint involvement, autoantibody positivity, and presence of elevated inflammatory markers (CRP or ESR).
Statistical analysis
The proportion of patients meeting either or both sets of classification criteria was compared using McNemar’s chi-square test. The median time to meeting criteria from presentation was compared between classification criteria using a Wilcoxon signed-rank test. The median time to starting a DMARD was compared between initial classification criteria groups also using Wilcoxon signed-rank tests. A 2-tailed p value < 0.05 was taken to indicate statistical significance.
RESULTS
Demographics and baseline characteristics
Seventy-nine of the 117 patients enrolled in the early arthritis study were included in the current analysis. Of the 38 patients who were excluded, 37 did not meet the minimum followup period of 1 year and 1 patient had an alternative diagnosis at initial visit. Demographics and baseline characteristics are out-lined in Table 1.
Demographic and baseline characteristics for 79 patients.
Classification outcome
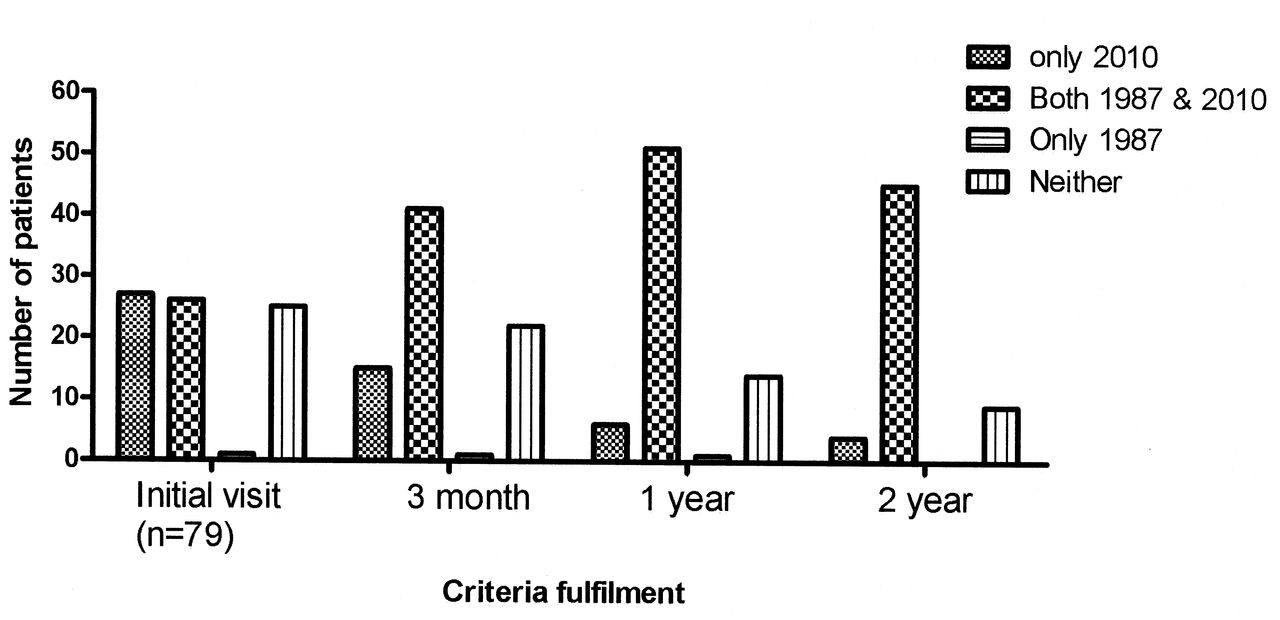
During the 2-year period, 7/79 (9%) patients received a diagnosis other than RA or UIA. Of those patients, 6 fulfilled neither set of RA criteria and 1 fulfilled only the 2010 criteria. Figure 1 illustrates the classification outcome of the cohort (n = 79) at the initial and 2-year visits.

Classification criteria outcomes. UIA: undifferentiated inflammatory arthritis; PsA: psoriatic arthritis; ReA: reactive arthritis; IBD: inflammatory bowel disease–related arthritis; SS: Sjögren’s syndrome; NR: visit not reached; FU: followup.
A total of 10/79 patients (13%) had a self-limiting arthritis (7/10 fulfilled neither set of RA criteria, 2/10 fulfilled only 2010 criteria, and 1/10 fulfilled both criteria at the initial visit). Four out of 79 patients had not reached the 2-year visit at the time of the analysis. A further 3 patients were lost to followup and 10 patients were discharged from clinic prior to the 2-year visit (self-limiting arthritis, n = 7; nonerosive arthritis in remission on DMARD, n = 3). Thus data were available for 62/79 patients at the 2-year timepoint. At 2 years, 49/62 patients (79%) fulfilled either RA criteria while 9/62 patients (15%) still had a diagnosis of UIA.
Comparison of the 1987 ACR and the 2010 ACR/EULAR criteria
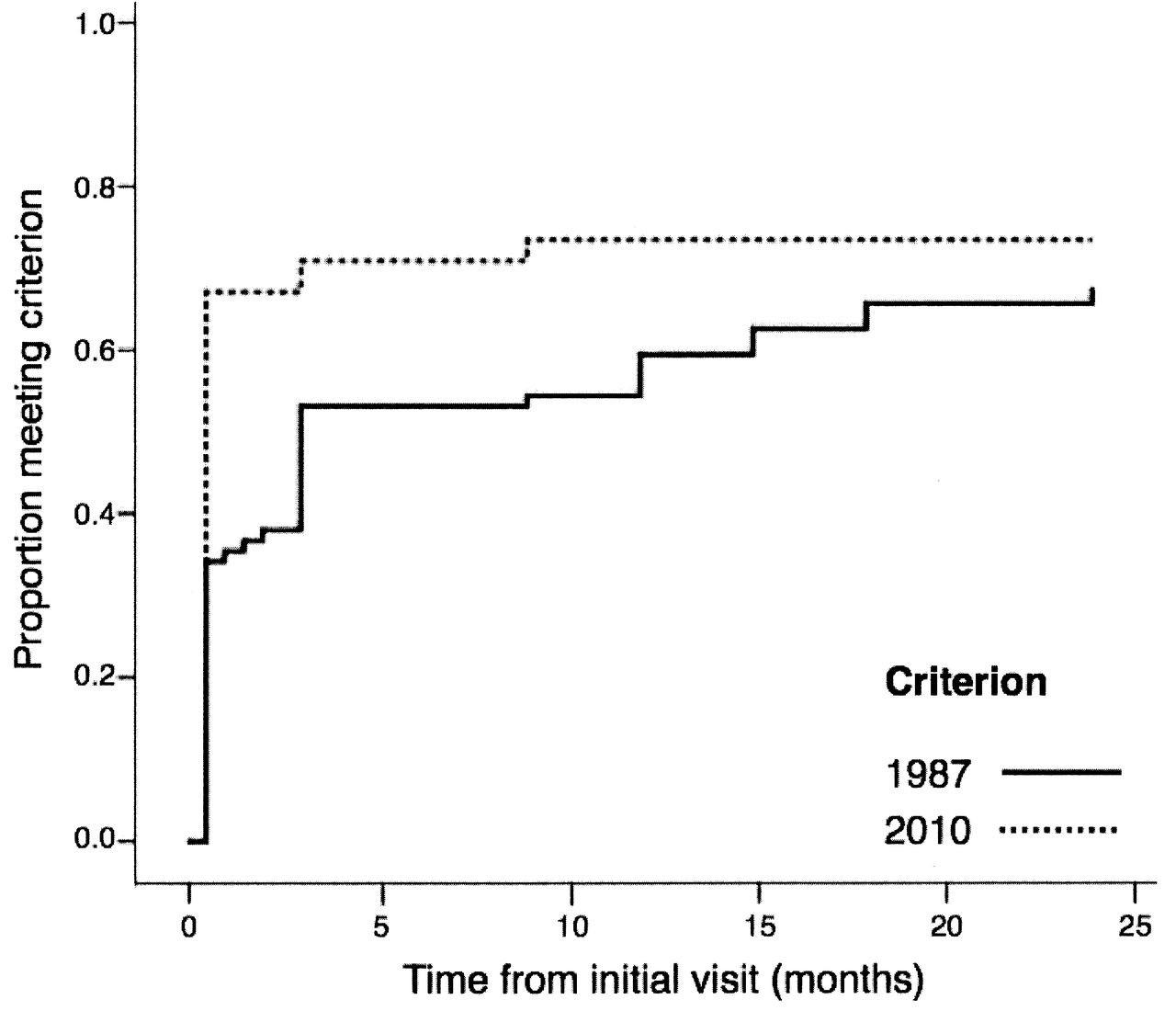
At the initial visit, 27 patients fulfilled only the 2010 criteria, 26 patients fulfilled both criteria, and 25 patients fulfilled neither. One patient fulfilled only the 1987 criteria. Twice as many patients fulfilled the 2010 criteria (53/79, 67%) at initial visit compared to the 1987 criteria (27/79, 34%; p < 0.001). There was a statistically significant increase in the number of patients fulfilling both criteria between the initial and 3-month visit. This increase occurred because 12/27 patients (44%) who fulfilled only the 2010 criteria at the initial visit went on to also fulfill the 1987 criteria by 3 months (p < 0.001; Figure 2). At 1 year, 14/79 patients (18%) still had a diagnosis of UIA. This declined to 9/62 by 2 years (15%). At the 2-year timepoint, the majority of patients (45/62, 73%) fulfilled both criteria. The 2010 criteria allowed more patients to fulfill RA classification criteria at an earlier stage (p < 0.001; Figure 3). The median time to fulfilling the 2010 criteria and 1987 criteria was 0 months (range 0–9 months) and 2.0 months (range 0–24 months), respectively.
Comparison of the 1987 ARA and 2010 ACR/EULAR criteria fulfillment.
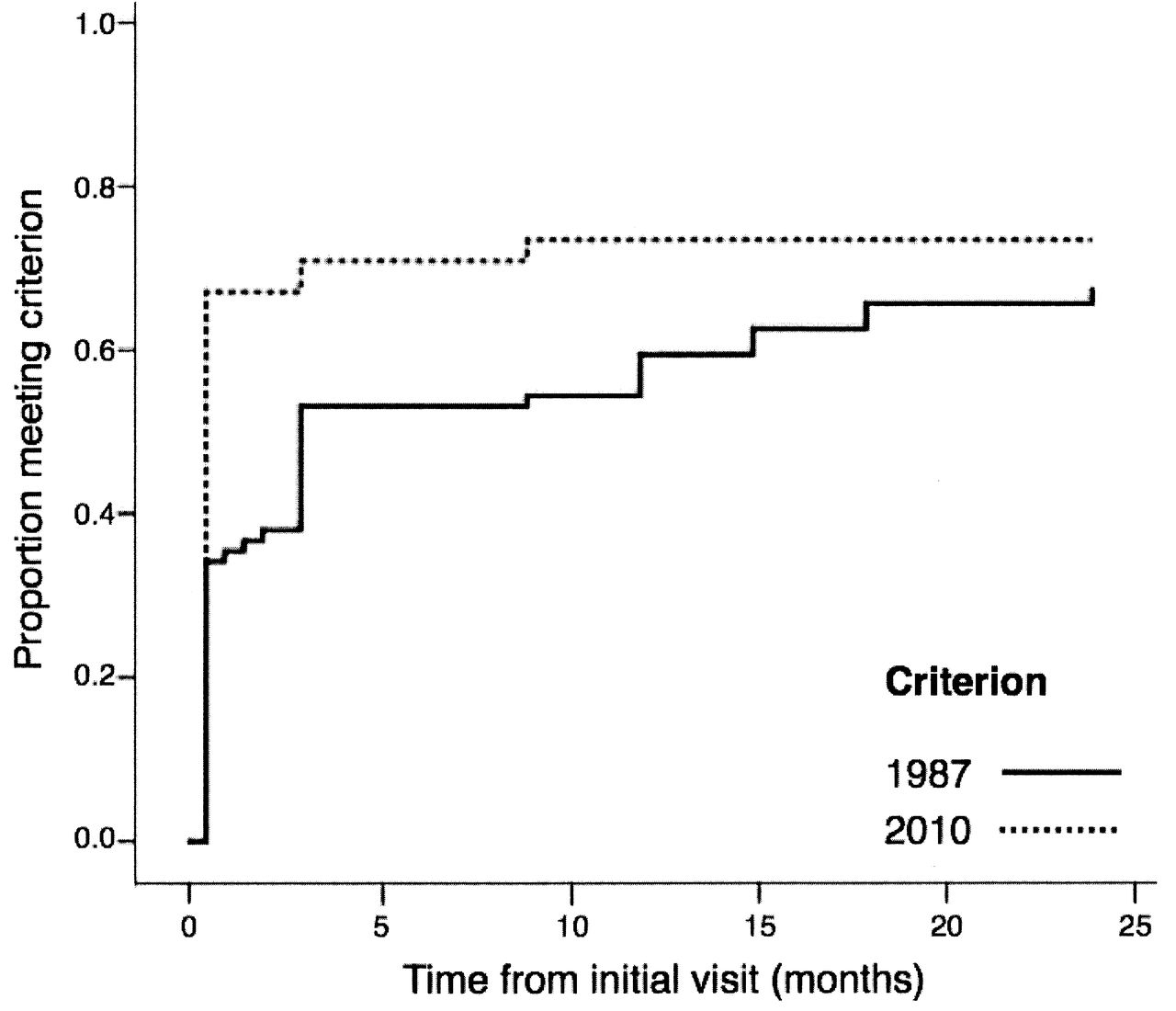
Time to fulfill classification criteria. At 2 years, 57 patients fulfilled the 2010 criteria and 52 patients fulfilled the 1987 criteria.
Factors determining earlier fulfillment of the RA criteria
There were 27 patients who fulfilled only the 2010 criteria at initial visit. For each of these patients, we looked at which factors of the 2010 criteria contributed to additional points when compared to the 1987 criteria, allowing 2010 criteria fulfillment. Factors allowing earlier fulfillment of the 2010 RA criteria were the requirement for fewer swollen and tender joints (n = 11), presence of elevated CRP or ESR (n = 13), and weighting of autoantibodies (n = 12). Eight patients did not meet the 1987 criteria solely because of short symptom duration (mean 3.6 weeks, range 2.0–5.0 weeks). Two patients in the only-2010 criteria group were ACPA-positive and RF-negative.
Comparison of classification criteria and DMARD requirement
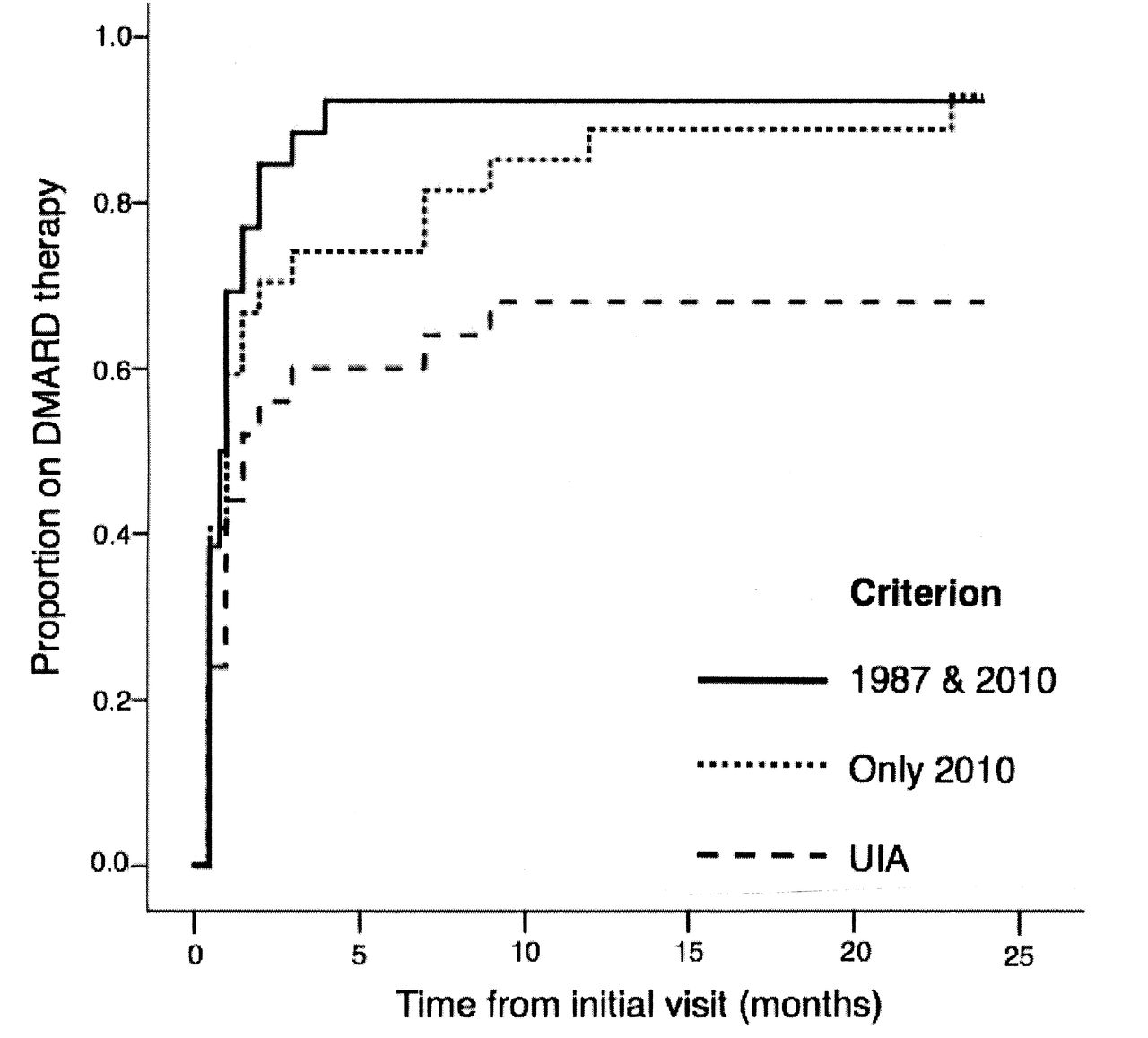
Patients who fulfilled both 1987 and 2010 criteria began taking DMARD earlier than those who fulfilled only the 2010 criteria, but the number of patients was not statistically significant (Figure 4). The median interval to initiating DMARD in those fulfilling only the 2010 criteria was 1.0 month (range 0–24.0 months) compared to 0.8 months (range 0–4.0 months) in those fulfilling both criteria (p = 0.43). At 12 months, 90% or more of patients who had met either RA criteria were taking a DMARD. Those who were not taking a DMARD either had a self-limiting arthritis or were lost to followup. Of those patients who fulfilled only the 2010 criteria at baseline, 25/27 (93%) ultimately received DMARD therapy compared with 24/26 (92%) of those fulfilling both criteria. The 2010 criteria detected more patients (49/79, 62%) at initial visit subsequently requiring DMARD (p = 0.007) compared to the 1987 criteria (25/79, 32%). The predominant choice of DMARD was methotrexate (MTX) in 41/58 patients (71%) who met either RA criteria by 2 years. Prognostic characteristics of the initial classification are shown in Table 2.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of classification criteria and requirement for DMARD. UIA: undifferentiated inflammatory arthritis.
Autoantibody positivity and joint erosion.
Comparison of classification criteria and joint erosion
The presence of joint erosions, DAS28, and prior corticosteroid use was highest among patients fulfilling both criteria at initial visit compared to the other groups (Table 2). Among those fulfilling only the 2010 criteria at the initial visit, 6/27 patients (22%) went on to develop joint erosion. A total of 17/79 patients developed joint erosions among our study cohort, all of whom fulfilled both the 2010 and 1987 criteria by 2 years. RF and ACPA positivity rates were similar between only-2010 criteria and both criteria groups. Prognostic characteristics of the initial classification are shown in Table 2.
DISCUSSION
Early intensive management of RA with DMARD therapy is the current standard of care to prevent permanent joint damage. However, the 1987 ARA classification criteria have lacked sensitivity for early classification of RA. The development of the 2010 ACR/EULAR classification criteria was aimed at allowing early classification and hence treatment of patients with RA.
Despite the small size of our study, we confirmed that the 2010 criteria resulted in earlier classification of RA than did the 1987 criteria. The 2010 criteria allowed an additional 26/79 patients (33%) to be identified within the first 3 months, of whom 24/26 (92%) subsequently received DMARD. One of the distinct differences of the 2010 criteria is the introduction of a weighting scoring system for joint assessment and autoantibody positivity. Minimum symptom duration fulfillment is no longer mandatory with the new criteria, which allowed an additional 8 patients to fulfill the 2010 criteria but not the 1987 criteria. Given the differences in scoring methods between the 2010 and 1987 criteria, it was not possible to make direct statistical comparisons. A larger cohort with a more objective methodology may help identify factors determining earlier fulfillment of the criteria more accurately.
Calculating sensitivity and specificity for classification criteria is a challenge because there is no gold standard test for the diagnosis of RA. Instead, studies have calculated sensitivity and specificity based on requirement for DMARD therapy. The working group of the 2010 ACR/EULAR criteria validated the criteria in 3 cohorts and reported that the new criteria were fulfilled in 87%–97% of patients who required MTX4. Recent studies also reported improved sensitivity of the 2010 criteria for early RA. Both Cader, et al5 and van der Linden, et al6 found the 2010 criteria to have higher sensitivity but lower specificity when using DMARD and MTX use as an outcome, compared with the 1987 criteria. In comparison, Varache, et al found no difference in diagnostic accuracies between the 2 criteria7. Our study found that there was no statistically significant difference in the timing of DMARD initiation between the 2 criteria, hence showing no difference in the way we managed our cohort of patients. This finding probably reflects that the new RA criteria are catching up with and reflecting current clinical practice for early DMARD therapy. It also raises the question of whether we could improve our practice further by initiating DMARD earlier. In our study, the median time for DMARD initiation among those fulfilling only 2010 criteria was 1 month from initial visit, while the mean symptom duration at initial presentation was 3.6 months (range 0.5–12.0). The feasibility of starting DMARD any earlier would depend on the time required to complete investigations as well as available resources. Whether starting DMARD earlier than 1 month would improve clinical outcome is uncertain.
RA has been considered a heterogeneous disorder and the 2010 criteria are anticipated to increase heterogeneity and help define very early RA. However, this may lead to increased false positivity, reflected by the lower specificity rate of the 2010 criteria. A large study by van der Linden, et al with 2258 patients with early arthritis found that 18% of patients (194/1099) who fulfilled the 2010 criteria had a revoked diagnosis at followup6. Cader, et al found that 8% of patients (7/87) fulfilling the 2010 criteria at baseline eventually had an alternative diagnosis5. The rate of self-limiting arthritis in their study was higher in the 2010 criteria group compared with the 1987 criteria group (8% vs 2%), and it was felt that overdiagnosis was an important issue to consider. In comparison, our study had a high proportion of 2010 RA criteria fulfillment at baseline with a low rate (1/53, 2%) of eventual non-RA diagnosis in the 2010 criteria group compared with other studies. Most patients (7/10) with self-limiting arthritis in our study had a UIA with 3/10 patients fulfilling RA criteria.
We found that although the 1987 RA criteria took longer to be fulfilled compared to the 2010 RA criteria, both criteria were similar in predicting joint erosions and subsequent need for DMARD. All the patients who developed joint erosions in our cohort went on to fulfill both RA criteria. The DMARD requirement was similar between those fulfilling only the 2010 criteria at baseline compared to those fulfilling both criteria. However, patients who fulfilled only the 2010 criteria at initial visit received DMARD therapy later than those who fulfilled both criteria, although this was not statistically significant. We believe those patients who fulfill only the 2010 criteria in our study do not represent those with milder disease, a finding reflected by the significant number who developed erosions (22%) or required DMARD (93%) at 2 years, as shown in Table 2.
In our early arthritis cohort, the 2010 ACR/EULAR RA criteria allowed earlier RA classification compared with the 1987 ARA criteria. Both criteria had similar performance at predicting joint erosions and subsequent need for DMARD.
Appendix
The 1987 American Rheumatism Association (ARA) and 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) rheumatoid arthritis (RA) classification criteria.
- Accepted for publication August 8, 2012.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.