
Abstract
Objective. Previous work has suggested involvement of the muscle microvasculature in the pathogenesis of dermatomyositis (DM). Our study evaluates whether standard histochemical reactions can identify microvascular changes in muscle biopsies from patients with DM compared to myopathic and nonmyopathic controls.
Methods. Muscle biopsies were obtained from 111 patients, including 45 patients with DM. Microvascular quantitation was performed on transversely oriented 1-μm toluidine blue-stained plastic sections. Histoenzymatic procedures included alkaline phosphatase (AP), nicotinamide adenine dinucleotide tetrazolium reductase (NADH-TR), succinate dehydrogenase (SDH), cytochrome C oxidase (COX), and myosin ATPase reactions.
Results. Capillary density was significantly lower in DM muscle biopsies compared to biopsies from patients with noninflammatory myopathies (NIM; n = 26) and healthy control muscle (n = 27; mean ± SD: 252 ± 114 vs 402 ± 56 and 325 ± 109 capillaries/mm2, respectively; p values < 0.05). In contrast, a marked increase in the number of capillaries staining with NADH-TR was noted in DM compared to other idiopathic inflammatory myopathies (IIM; n = 13), NIM, and controls (49.8 ± 50.7 vs 8.0 ± 7.1, 6.7 ± 7.2, and 3.6 ± 2.8 capillaries/mm2; p < 0.05 compared to DM). DM capillaries also demonstrated mildly increased staining with AP compared to controls; however, no increased SDH or COX reactivity was observed.
Conclusion. DM muscle capillaries are highly reactive with NADH-TR compared to myopathic and nonmyopathic controls. The lack of staining of DM capillaries with mitochondrial SDH and COX reactions suggests that NADH-TR reactivity may be secondary to activation of the microvascular endoplasmic reticulum, rather than mitochondrial hyperplasia.
- DERMATOMYOSITIS
- ETIOLOGY
- HISTOCHEMICAL REACTIONS
Dermatomyositis (DM) is an idiopathic inflammatory myopathy associated with proximal muscle weakness and characteristic cutaneous manifestations1. While the cause for DM remains unclear, involvement of the muscle microvasculature is implicated in disease pathogenesis2. Capillary loss is believed to precede other pathological muscle changes, and the inflammatory infiltrate in DM is predominantly perivascular as well as perimysial2,3.
Multiple standard histochemical reactions are routinely performed to evaluate muscle tissue for aid in diagnosis of clinical disease. The nicotinamide adenine dinucleotide tetrazolium reductase (NADH-TR) reaction is a histochemical reaction used for evaluation of the space between the myofibrils referred to as the intermyofibrillary matrix. Electrons are transferred from NADH to the colorless soluble tetrazolium salt, converting it to an insoluble blue formazan compound. This reaction is catalyzed by enzymes in the mitochondria (NADH-dehydrogenase) or in the endoplasmic reticulum (NADH cytochrome b5 reductase). The alkaline phosphatase (AP) reaction is a histochemical reaction done at alkaline pH, which uses an esterase reaction to provide an excellent evaluation of regenerating muscle fibers and regions of the microvasculature. Succinate dehydrogenase (SDH) and cytochrome C oxidase (COX) are reactions specific for mitochondria that are typically used to screen for mitochondrial myopathies. While NADH-TR reactivity implies activation of enzymes in the mitochondria or endoplasmic reticulum, SDH or COX reactivity implies activation of enzymes specific to the mitochondria.
Our study examines muscle biopsies from 111 patients including 45 patients with DM and evaluates staining of the muscle microvasculature with the NADH-TR, AP, SDH, and COX reactions. It identifies significantly increased staining of the microvasculature in DM muscle with NADH-TR compared to inflammatory and noninflammatory myopathies and healthy muscle. The lack of staining of DM capillaries with SDH and COX suggests that this increased staining in DM may be due to activation of the microvascular endoplasmic reticulum, rather than mitochondrial hyperplasia. Further evaluation of this finding may be warranted to develop NADH-TR as a potential biomarker of DM when classic pathologic findings such as perifascicular atrophy are absent.
MATERIALS AND METHODS
Patients
Evaluation of all human tissue samples was done in accord with the guidelines of the Human Research Subject Protection Committee at the University of California at Los Angeles. All biopsies were evaluated and scored by the same pathologist. Patients with DM and polymyositis (PM) fulfilled the diagnostic criteria of Bohan and Peter4,5. No juvenile cases were included. Biopsies from patients with DM had at least 3 of the following 4 histological characteristics: perifascicular atrophy, perivascular inflammation, single-fiber hyperlipidation, or subsarcolemnal and fiber MHC-1 expression. Patients with PM had elevated serum creatine kinase, no evidence of malignancy, and randomly distributed scattered fiber necrosis associated with inflammatory infiltrates, with a predominance of CD8-positive T cells. Patients with inclusion body myositis (IBM) had biopsies with inclusions noted as rimmed vacuoles in H&E and trichrome reactions and confirmed on 1-μm section analysis. Noninflammatory myopathies were defined histologically by the absence of inflammatory cell infiltrates and the presence of denervation/reinnervation changes including scattered angular fiber atrophy, grouped fiber atrophy, and variable degrees of reinnervation characterized by fiber-type grouping. Normal muscle specimens were obtained from patients with complaints of myalgias but no myopathic or neuropathic changes noted on the multiple histochemical and histoenzymatic reactions performed.
Muscle histochemistry
For all specimens, fresh muscle was quenched in isopentane and cooled to −180°C in liquid nitrogen. Transversely oriented cryostat sections were prepared and analyzed with multiple histochemical and histoenzymatic reactions including NADH-TR, SDH, COX, a modified Gomori trichrome, Oil Red O stain, periodic acid-Schiff with and without diastase predigestion, myosin ATPase following preincubation at pH 9.4, 4.6 and 4.3, myophosphorylase, and acid and AP6. Myosin ATPase at pH 4.3 was used for calculation of fiber numbers unless the reaction was poor quality, in which case either pH 9.4 or pH 4.6 was used based on the best-quality reaction. Small sections of each muscle biopsy were also fixed in 10% formalin and embedded in paraffin.
Quantitation of total fiber number
The density of type 1 and type 2 fibers was quantitatively assessed at 10× magnification on myosin ATPase reactions as described. Four to 7 grid fields were assessed, allowing for the enumeration and fiber typing of 250–400 fibers per muscle biopsy. Fiber number and type were expressed per mm2.
1-micrometer section analysis
For analysis of microvascular density [number of capillaries/small arterioles per muscle area (mm2)], 1-μm plastic-embedded sections were evaluated. For each biopsy, a thin fascicle measuring about 1 cm × 2 mm was obtained, placed on filter paper under slight tension for about 3 min, and fixed in 3% buffered glutaraldehyde/2% paraformaldehyde. Following fixation, 4–6 blocks were prepared and subsequently processed routinely, cut transversely at 1 μm, and stained with toluidine blue. Three blocks were selected for analysis and counts performed at objective 40× on a minimum of 2 blocks. Contiguous fields were counted if possible, passing over the fascicles including the central and perifascicular zones. In a given patient, 22–36 fields were assessed. No quantitative assessment of capillary density was performed on frozen sections.
NADH-TR microvasculature reactivity
Capillaries and small arterioles throughout the endomysium were assessed for NADH-TR reactivity in grid squares at 20× magnification. Fields were arbitrarily selected without artifact but all attempts were made to count contiguous grid fields. For each biopsy, 10–30 fields were assessed, and the NADH-TR-positive vascular index was calculated as number of NADH-TR-reactive microvessels/mm2. The intensity of NADH-TR staining of the type 1 and type 2 fibers did not appear to affect quantitation. Vascular profiles for capillaries were 1–3 μm in diameter with a central unstained lumen, while small arterioles were assessed at 8 μm or less. Macrophages and very atrophic myofibers were carefully excluded.
AP microvasculature reactivity
Capillaries and small arterioles were assessed for AP reactivity in grid squares at 10× magnification. Longitudinal vessel profiles passing across grid squares were counted in each square. It was noted that an apparent increased density of AP-positive vessels occurred in near fields of intrafascicular nerve bundles and nonspecific esterase-positive motor endplates.
SDH/COX reactivity
The SDH and COX reactions were performed by standard methods, and capillaries and small arterioles were assessed for SDH and COX reactivity in grid squares at 20× magnification.
RESULTS
Muscle fiber density is increased in patients with DM compared to myopathic and nonmyopathic controls
Perifascicular muscle fiber atrophy is a classic microscopic finding in patients with DM7. Examination of fiber numbers per mm2 measured by the myosin ATPase reaction revealed significantly increased muscle fiber density in DM biopsies compared to both myopathic and nonmyopathic controls (Table 1).
Capillary and myofiber density in muscle from patients with dermatomyositis (DM), other idiopathic inflammatory myopathies, noninflammatory myopathies (NIM), and healthy muscle. Values are mean ± SD.
Numbers of capillaries are decreased in muscle from patients with DM compared to noninflammatory myopathies and normal muscle controls
Muscle biopsies from 45 patients with DM were compared to 27 normal muscle biopsies, 26 noninflammatory myopathic muscle biopsies (NIM), and 13 biopsies from patients with other idiopathic inflammatory myopathies (IIM; 4 IBM, 9 PM). Total numbers of capillaries and small arterioles measured per muscle area (mm2) by 1-μm section analysis were significantly decreased in DM muscle compared to controls and NIM (Table 1). Differences in microvascular numbers between DM muscle and control groups were magnified when compared as numbers of blood vessels per muscle fiber (Table 1). No differences in muscle capillary numbers were found between patients with DM and other IIM (Table 1).
Numbers of muscle capillaries staining with NADH-TR are increased in biopsies from patients with DM compared to myopathic and nonmyopathic controls
Total numbers of capillaries and small arterioles staining with NADH-TR were significantly increased in muscle from patients with DM compared to controls and other IIM and NIM. Differences were significant in assessment of capillary numbers per muscle area as well as in capillaries measured per muscle fiber (Table 2, Figure 1).
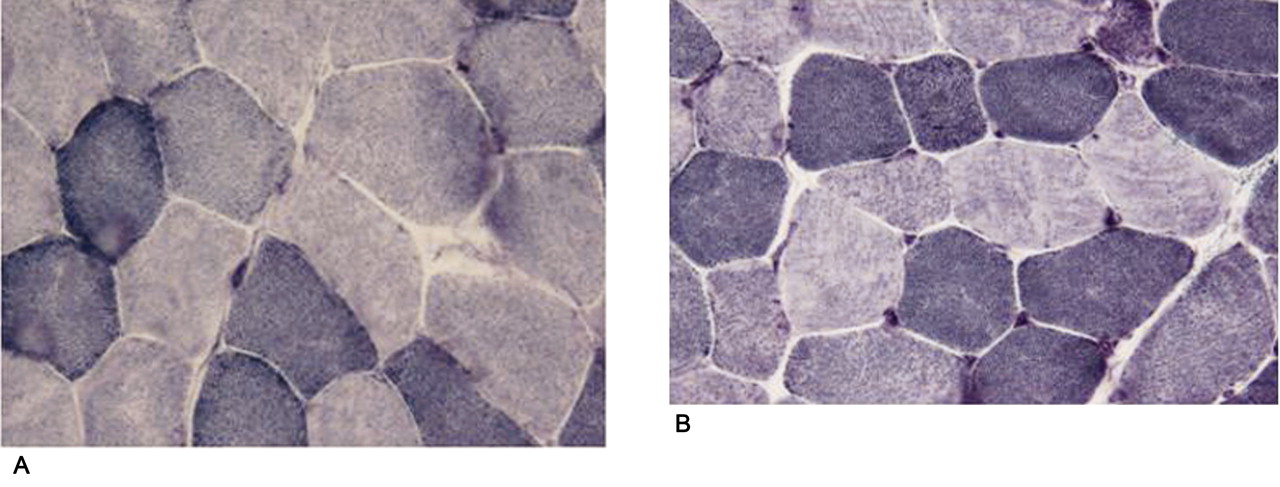
Representative grid fields from (A) normal muscle, showing a single NADH-TR-reactive capillary; and (B) dermatomyositis muscle, showing multiple NADH-TR-reactive capillaries.
Nicotinamide adenine dinucleotide tetrazolium reductase (NADH-TR) reactivity of muscle microvasculature in muscle from patients with dermatomyositis (DM), other idiopathic inflammatory myopathies, noninflammatory myopathies (NIM), and healthy muscle. Values are mean ± SD.
The ratio of NADH-TR-positive capillaries to the total number of capillaries in muscle was over 15 times higher in the DM group compared to the control group (0.29 ± 0.44 DM vs 0.018 ± 0.026 control; p < 0.0001). Similar differences were also seen in comparison of DM biopsies with other IIM and NIM groups (Table 2).
The percentage of muscle capillaries staining with NADH-TR is negatively correlated with total capillary number in patients with DM
A significant negative correlation of the percentage of capillaries staining positive for NADH-TR with the total capillary number was observed in muscle biopsies from patients with DM (r = −0.55, p < 0.0001). A higher percentage of NADH-TR-reactive capillaries was associated with a lower total number of capillaries in DM muscle. No significant correlations were seen in other myopathic and nonmyopathic control groups. However, there was a trend in the other IIM muscle group for a similar correlation between the percentage of capillaries staining positive for NADH-TR and the total capillary number (r = −0.41, p = 0.36).
Microvascular SDH and COX staining are not increased in DM or other myopathic/nonmyopathic controls
No abnormal SDH or COX reactivity was observed in intramuscular capillaries or muscle fibers in DM, other IIM, NIM, or control biopsies.
AP reactivity is increased in DM capillaries compared to nonmyopathic controls
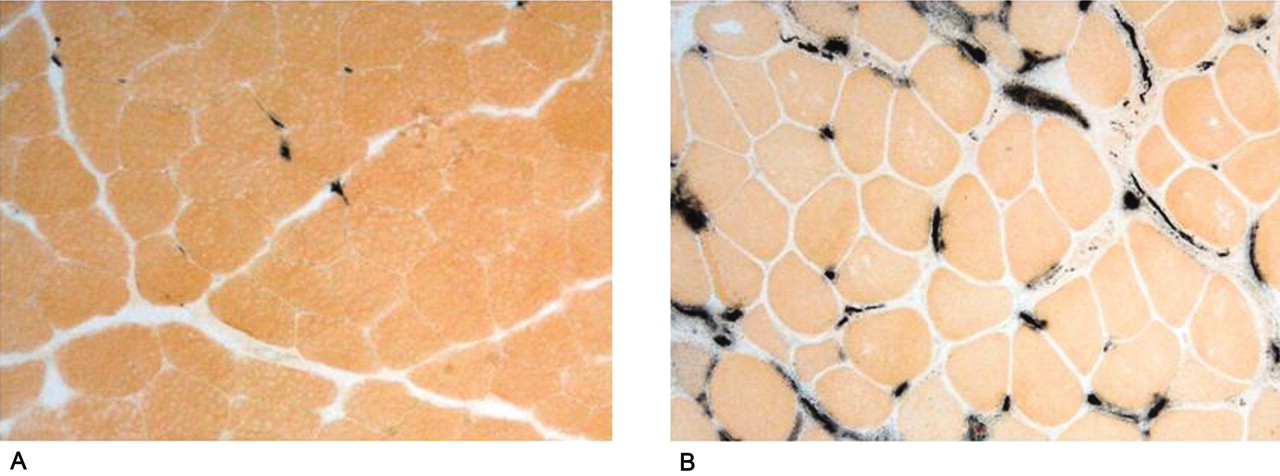
Total numbers of capillaries reacting positively with the AP reaction were significantly increased in muscle biopsies from patients with DM compared to control biopsies (p < 0.0001; Table 3, Figure 2). Trends were also seen for increased reactivity of DM muscle capillaries with AP compared to other IIM and NIM (Table 3).

{kind=link}
{kind=link}
Representative grid fields from (A) normal muscle, showing few alkaline phosphatase-reactive capillaries; and (B) dermatomyositis muscle, showing multiple alkaline phosphatase-reactive capillaries.
Alkaline phosphatase (AP) reactivity of muscle microvasculature in muscle from patients with dermatomyositis (DM), other idiopathic inflammatory myopathies, noninflammatory myopathies (NIM), and healthy muscle. Values are the mean ± SD.
The percentage of DM muscle capillaries reacting with AP was negatively correlated with total capillary numbers (r = −0.66, p < 0.0001); a higher percentage of reactive capillaries was associated with a lower total capillary number in muscle. In contrast, NIM muscle biopsies showed a positive correlation between the percentage of AP-reactive capillaries and the total capillary number; a higher percentage of AP-reactive capillaries was associated with a higher total capillary number in NIM (r = 0.62, p = 0.01).
DISCUSSION
Work by Emslie-Smith and Engel2 and others in a small number of patients with DM demonstrated both focal capillary depletion and reduced capillary density in DM muscle. Muscle biopsies from patients with early DM showed minimal structural damage but significantly lower capillary density compared to normal muscle specimens. Findings from advanced DM biopsies were similar to those of early DM but with more severe capillary loss2,8.
We examined muscle biopsies from a cohort of 111 patients, including 45 patients with DM, and confirmed the capillary dropout in muscle from adult patients with DM compared to noninflammatory myositis and normal muscle controls. Interestingly, no differences in muscle capillary numbers were found between patients with DM and other IIM — a finding that has also been reported by Grundtman, et al9. Our current work also demonstrated increased myofiber density in DM compared to myopathic and nonmyopathic controls, consistent with the classic microscopic finding of perifascicular muscle fiber atrophy in DM. Other patterns of presumed microvascular injury including necrotizing myopathy with pipestem capillaries are not associated with perifascicular atrophy, although a chronic small-vessel ischemic myopathy is also postulated10.
Apart from the well defined perifascicular fiber atrophy and associated myofibrillar degenerative changes in this compartment, increased fiber size variability and a component of Type 2 fiber atrophy throughout the DM biopsies all contributed to the significant increase in muscle fiber density assessed on an areal basis (Table 1). However, there was no significant shift in the ratio of type 1/type 2 fibers. Notably, while we confirmed the reduction in the number of capillaries per unit area, when expressed in terms of capillaries per muscle fiber, the degree of significance was markedly increased in DM as well as in other inflammatory myopathies. Grundtman and colleagues9 assessed CD31-expressing capillaries using computerized image analysis, and also found a significant capillary reduction in the patients with DM without inflammatory infiltrates compared to normal subjects. Moreover, they did not find a difference in capillaries during both early and chronic phases of disease, and they did not find a difference in capillary number between DM and PM similar to our work9. Additional data were obtained by Nagaraju, et al, who showed that the number of CD146-positive blood vessels per muscle fiber was not different between juvenile DM and childhood controls; however, the index was significantly reduced in adult DM compared to adult controls (1.3 ± 0.2 vs 2.2 ± 0.3 capillaries per muscle fiber, respectively)3. These values are remarkably similar to those we obtained using 1-μm plastic section analysis and ATPase-stained fiber morphometry (Table 1). Although CD31 and CD146 are well recognized immunohistochemical markers for capillaries and have been used in a semiquantitative way to assess microvascular numbers, we wished to obtain an accurate baseline for capillary density using 1-μm plastic section analysis in which normal and slightly damaged vessels could be easily determined.
When DM capillaries in the current cohort were further examined with multiple histochemical stains, they were strongly reactive with NADH-TR, a standard histochemical reaction traditionally used for evaluation of the intermyofibrillary reticulum and mitochondria. NADH-TR reactivity was markedly increased in DM capillaries compared to controls, and distinguished DM muscle from other IIM, noninflammatory myopathies, and healthy, normal muscle. To our knowledge, this finding has not been previously reported.
In DM muscle there was also a moderate to strong correlation of capillary numbers with NADH-TR reactivity. A higher percentage of NADH-TR-reactive capillaries was associated with a lower number of total muscle capillaries. These data imply a potential link between the pathologic process driving capillary dropout in DM, and the process driving the NADH-TR reactivity. Whether NADH-TR-reactive capillaries could also represent new blood vessel formation in response to capillary damage is a subject of future investigation.
The NADH-TR reaction is a multicomponent enzyme reaction that includes rotenone and rotenone-insensitive complex 1 of the electron transport chain, NADH dehydrogenase, and portions of the microsomal (sarcoplasmic reticulum) electron transport system including cytochrome b5 reductase11. DM capillaries were not reactive with the mitochondrial SDH or COX reactions, suggesting that capillary NADH-TR reactivity is not driven by enzymes in the mitochondria due to mitochondrial hyperplasia. Instead, it may be driven by enzymes such as NADH cytochrome b5 reductase in the endoplasmic reticulum (ER). Activation of the microvascular ER in muscle capillaries of patients with DM has not previously been reported. However, work by Gargalovic, et al has suggested that ER stress genes such as the unfolded protein response are activated in endothelial cells in response to oxidative stress12.
Given that the increase in NADH-TR activity of the microcirculation is likely due to activation of the sarcoplasmic reticulum and/or a manifestation of neoangiogenesis in DM, what evidence supports a role for neovascularization in DM? The capillary reduction will contribute to local tissue ischemia, a known stimulus for expression of interleukin, intercellular adhesion molecule, and vascular endothelial growth factor (VEGF)13,14,15 shown to occur in DM and PM in the case of VEGF9, as well as in the upregulation of other proangiogenic molecules that participate in angiogenesis, leukocyte movement, and complement activation3. Therefore, VEGF as well as other factors may contribute to the neoangiogenesis seen in DM and to a lesser extent in PM9. Our study did not analyze the role of steroids given before or after biopsy, but most of the biopsies were taken before or at the time of initiation of steroid therapy. In addition, our study did not evaluate the relationship of characteristic tubuloreticular inclusions seen in DM microvascular endothelium16,17 to SDH, COX, or NADH-TR reactivity. However, when these inclusions were noted in the biopsies, no change in mitochondrial endothelial number/pleomorphism or NADH-TR reactivity was readily observed.
Finally, trends were observed in our study for increases in AP capillary reactivity in DM muscle compared to myopathic and nonmyopathic controls. The magnitude of the increased reactivity was much less than that seen with the NADH-TR stain. However, a similar negative correlation of the percentage of DM muscle capillaries reacting with alkaline phosphatase with the total capillary numbers was observed.
The AP reaction has been used for the demonstration of myofiber degeneration/regeneration change and shows linear reactivity throughout the perimysium in DM11. An increased AP-positive vascular index has previously been observed in some cases of DM/PM18, and localized areas of reactivity are normally evident at arterial branch points and secondary branches in the capillary microcirculation19,20. Our study confirmed an increased AP activity within the DM microcirculation (Table 3). There was no increased staining at the branch points of the microcirculation, so we assume that the enzyme induction may reflect neovascularization or other endothelial cell activation. Given that microvascular degeneration and regeneration occur simultaneously, cases with a high index could represent a more successful neoangiogenesis and potentially a useful prognostic biomarker.
Our work identifies abnormal microvasculature activation in DM with NADH-TR compared to other inflammatory and noninflammatory myopathies as well as normal muscle. While one of the strengths of our study is the relatively large biopsy cohort size, certainly these data warrant further validation in other large cohorts before NADH-TR capillary reactivity can be considered as a potential biomarker of DM. In addition, future study of the role of microvascular ER stress in the pathogenesis of DM may be warranted, and may have potential implications for the development of new therapeutics.
- Accepted for publication August 23, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.