
Abstract
Objective. Spondyloarthritides (SpA) can present different disease spectra according to ethnic background. The Brazilian Registry of Spondyloarthritis (RBE) is a nationwide registry that comprises a large databank on clinical, functional, and treatment data on Brazilian patients with SpA. The aim of our study was to analyze the influence of ethnic background in SpA disease patterns in a large series of Brazilian patients.
Methods. A common protocol of investigation was prospectively applied to 1318 SpA patients in 29 centers distributed through the main geographical regions in Brazil. The group comprised whites (65%), African Brazilians (31.3%), and people of mixed origins (3.7%). Clinical and demographic variables and various disease index scores were compiled. Ankylosing spondylitis (AS) was the most frequent disease in the group (65.1%); others were psoriatic arthritis (18.3%), undifferentiated SpA (6.8%), enteropathic arthritis (3.7%), and reactive arthritis (3.4%).
Results. White patients were significantly associated with psoriasis (p = 0.002), positive HLA-B27 (p = 0.014), and use of corticosteroids (p < 0.0001). Hip involvement (p = 0.02), axial inflammatory pain (p = 0.04), and radiographic sacroiliitis (p = 0.025) were associated with African Brazilian descent. Sex distribution, family history, and presence of peripheral arthritis, uveitis, dactylitis, urethritis, and inflammatory bowel disease were similar in the 3 groups, as well as age at disease onset, time from first symptom until diagnosis, and use of anti-tumor necrosis factor-α agents (p > 0.05). Schober test and thoracic expansion were similar in the 3 groups, whereas African Brazilians had higher Maastricht Ankylosing Spondylitis Enthesitis Scores (p = 0.005) and decreased lateral lumbar flexion (p = 0.003), while whites had a higher occiput-to-wall distance (p = 0.02). African Brazilians reported a worse patient global assessment of disease (p = 0.011). Other index scores and prevalence of work incapacity were similar in the 3 groups, although African Brazilians had worse performance in the Ankylosing Spondylitis Quality of Life questionnaire (p < 0.001).
Conclusion. Ethnic background is associated with distinct clinical aspects of SpA in Brazilian patients. African Brazilian patients with SpA have a poorer quality of life and report worse disease compared to whites.
- SPONDYLOARTHRITIS
- ETHNIC GROUPS
- BRAZILIAN
- POPULATION
- EPIDEMIOLOGY
Spondyloarthritis (SpA) is a group of diseases that includes ankylosing spondylitis (AS), psoriatic arthritis (PsA), reactive arthritis (ReA), arthritis associated with inflammatory bowel disease (IBDA), and undifferentiated spondyloarthritis (USpA)1. The prevalence and phenotype of SpA can be modulated by genetic, environmental, and hormonal factors. Among genetic factors associated with SpA are the MHC class I2, interleukin 23 receptor (IL-23R), and endoplasmic reticulum-associated aminopeptidase 1 (ERAP-1)3,4. European populations with elevated prevalence of certain subtypes of HLA-B27 have higher prevalence of SpA, which is considered rare in sub-Saharan African countries where these HLA variants are rare2,5,6. The association of AS and ERAP-1 has been found in nearly all ethnic groups4, yet the association with IL-23R observed in studies from the United Kingdom, United States, Canada, Spain, and Portugal was not found in populations from Korea and China4. Despite all identified genetic effects, monozygotic twin studies showed a concordance rate for the disease in 70%, suggesting that 30% of susceptibility results from the environment7. Infections with gastrointestinal and genitourinary pathogens such as Campylobacter, Chlamydia, Salmonella, and Shigella are well-known trigger factors for ReA; patients with AS may have subclinical gut inflammation that can be a source of antigen stimuli to initiate the disease process7,8. Social and economic aspects may also influence higher exposure to infectious events, and also access to healthcare and treatment9.
In Brazil, few studies have described the features of SpA. As in other Latin American countries, Brazil has a particular multicultural genetic pool due to population miscegenation secondary to colonization in the last 500 years. After the European colonization (predominantly of Portuguese and Spanish origin), there was immigration of around 5 million black people from Africa between the 17th and the 19th centuries. In the 19th and 20th centuries, after the abolition of slavery, the country received a large number of immigrants, notably Italians (in the southeast), Japanese (southeast and center-west), and Germans (south). Descendants of the original Indians were mostly in communities in the Amazon region.
In the census of 2010, 48.7% of Brazilian people declared themselves as whites (predominantly European ancestry, with Portuguese, Spanish, or Italian origin), 43.6% as Mestizos (most originating from the mixing of whites and blacks), 7.0% black (pure origin), and 0.7% Asian ancestry (predominantly Japanese) and Indians10.
We analyzed the influence of the ethnic background in a large series of Brazilian patients with SpA, known as the Brazilian Registry of Spondyloarthritis (Registro Brasileiro de Espondiloartrites; RBE).
MATERIALS AND METHODS
This was a prospective, observational, and multicentric cohort of consecutive patients with SpA recruited from 29 referral centers participating in the RBE. All patients, from all the 5 major geographic areas in Brazil, were classified according to the European Spondylarthropathy Study Group criteria11, with data collected from June 2006 to December 2009. The RBE is part of the RESPONDIA group comprising 9 Latin American countries (Argentina, Brazil, Costa Rica, Chile, Ecuador, México, Perú, Uruguay, and Venezuela) and the 2 Iberian Peninsula countries (Spain and Portugal).
A protocol of investigation was applied to 1318 patients with SpA. The diagnosis of AS was considered if the patients fulfilled the New York modified criteria12, and the diagnosis of PsA if they fulfilled the Moll and Wright criteria13; ReA was considered when asymmetric inflammatory oligoarthritis of lower limbs was present, associated with enthesopathy and/or inflammatory low back pain following enteric or urogenital infections14; and enteropathic arthritis when the patient presented inflammatory axial and/or peripheral joint involvement associated with confirmed inflammatory bowel disease (IBD; Crohn’s disease or ulcerative colitis). Juvenile SpA was considered when the patient started SpA symptoms before 16 years of age.
Race was divided into whites and African Brazilians (black patients of unmixed ancestry and Mulattos, i.e., originating from the mixture of white and black populations) and other origins (including a few Indians and Japanese Brazilians, and white and/or African Brazilian miscegenation with indigenous and/or Asian-descent patients).
Demographic and clinical data were collected, including time of disease duration, tender and swollen joint count, visual analog scale for pain according to the patient (VAS for pain) and disease activity according to patient and physician (patient and physician VAS for disease activity). Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) values were recorded. The Bath Ankylosing Spondylitis Metrology Index (BASMI)15 was used for evaluation of spinal mobility. The presence of pain at enthesis sites was evaluated by Maastricht Ankylosing Spondylitis Enthesitis Score (MASES); MASES scores varied from 0 to 1316. Peripheral articular involvement was assessed by the 66 tender/swollen joint count. Disease activity and functional status were evaluated according to Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)17 and Bath Ankylosing Spondylitis Functional Index (BASFI)18, respectively. Quality of life data were recorded with the Ankylosing Spondylitis Quality of Life questionnaire (ASQoL), varying from 0 to 1819. All questionnaires had previously been translated, cross-translated, validated, and culturally adapted to the Portuguese language20. Radiological evaluation was performed by Bath Ankylosing Spondylitis Radiologic Index (BASRI), including BASRI-spine (lumbar and cervical spine and sacroiliac joints) and BASRI-total (BASRI-spine and BASRI-hips)21. The investigation center coordinators participated in a training session on radiographic interpretation before the start of the study. Cervical spine involvement was determined by goniometric measurement of cervical rotation (defined as < 20°, 20°–70°, and > 70°). Shoulder involvement was evaluated by the presence of pain and/or limitation of motion. Hip involvement was also assessed by clinical (presence of pain and/or limitation) and radiological evaluations (classified as normal, suspicious, mild, moderate, or severe) regarding BASRI-hips.
Statistical analysis
Categorical variables were compared by chi-square and Fisher exact tests, and continuous variables by ANOVA or Kruskal-Wallis test. A value of p < 0.05 was considered significant, and 0.05 > p > 0.10 was considered a statistical trend.
RESULTS
In the 1318 patients with SpA, AS was the most frequent disease in the group (65.1%) that also included PsA (18.3%), USpA (6.8%), enteropathic arthritis (3.5%), ReA (3.5%), and juvenile SpA (3.3%). Mean disease duration was 14.23 ± 10.42 years.
Demographic data showed that 65% of patients were white, with 31.3% African Brazilians and 3.7% other origins; in the African Brazilian group, only 5.8% reported pure black origin.
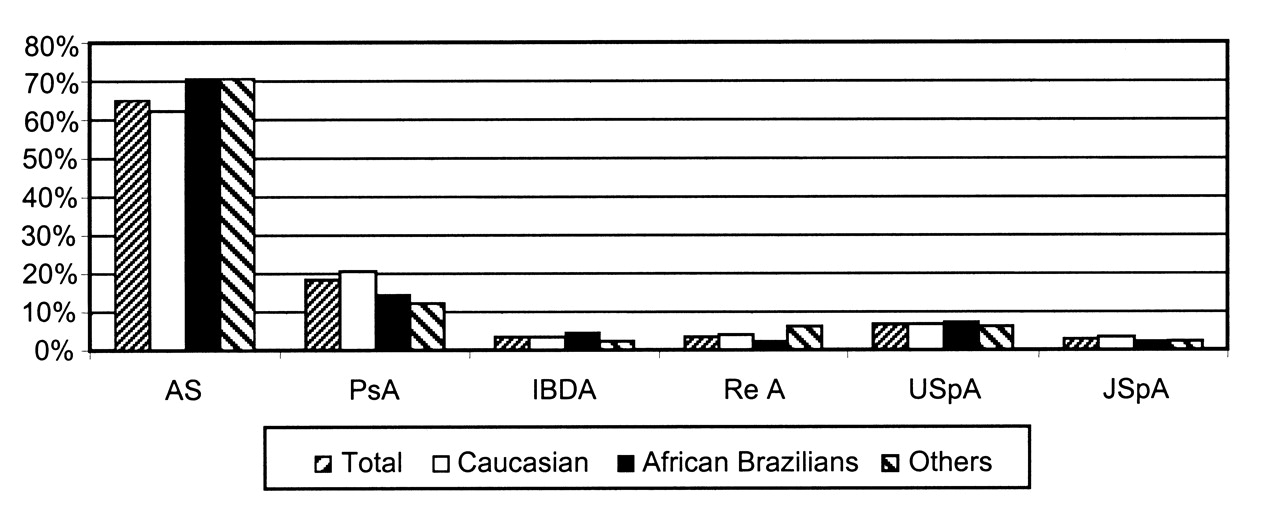
According to ethnic groups, there were similar distributions of diseases of the SpA group (Figure 1). Equal distribution of SpA involvement (axial, peripheral, and entheseal) was also found in the different ethnic groups.
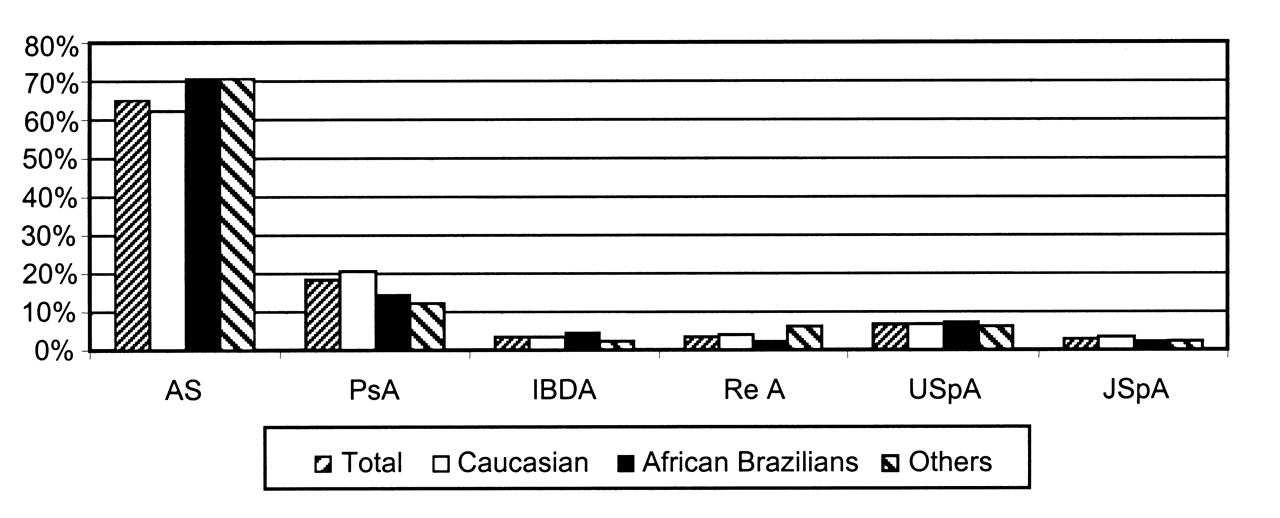
Spondyloarthritis in 1318 Brazilian patients according to ethnic background (p = 0.089). AS: ankylosing spondylitis; PsA: psoriatic arthritis; IBDA: arthritis associated with inflammatory bowel disease; ReA: reactive arthritis; USpA: undifferentiated spondyloarthritis; JSpA: juvenile spondyloarthritis.
Comparing demographic and clinical data on the 3 ethnic groups, it was observed that white patients presented statistical association with psoriasis, nail involvement, positive HLA-B27, and use of corticosteroids. African Brazilians were statistically associated with hip involvement, axial inflammatory pain, and radiographic sacroiliitis. Sex distribution, family history, presence of peripheral arthritis, uveitis, dactylitis, urethritis, and IBD were similar in the 3 groups, as well as age of disease onset, time from first symptom until diagnosis, and use of anti-tumor necrosis factor (TNF)-α agents (Tables 1 and 2).
Demographic and clinical data in 1318 Brazilian SpA patients, according to ethnic background.
Treatment data in 1318 Brazilian SpA patients.
The most commonly affected peripheral joints in the group were the ankles (20.5%) and knees (20.3%). No ethnic difference was observed in peripheral joint involvement, except for the small joints of the feet — the metatarsophalangeal (p = 0.0024) and interphalangeal (p = 0.019) joints, which were more commonly affected in the African Brazilians. The entheses most commonly affected were L5 spinal process (21.1%), anterior-superior (20.1%) and posterior spina iliaca (24.5%), and the Achilles tendon insertion (20.1%). There was a similar distribution of entheseal involvement according to race, except for the posterior spina iliaca, which was more commonly affected in African Brazilians (p = 0.029).
Analyzing the physical examination results, whites showed a higher occiput-to-wall distance, while African Brazilians presented with decreased lateral lumbar flexion and higher MASES scores (Table 3). Schober test and thoracic expansion findings did not differ in the 3 groups.
Data on physical examination in 1318 Brazilian SpA patients. Data are mean ± SE.
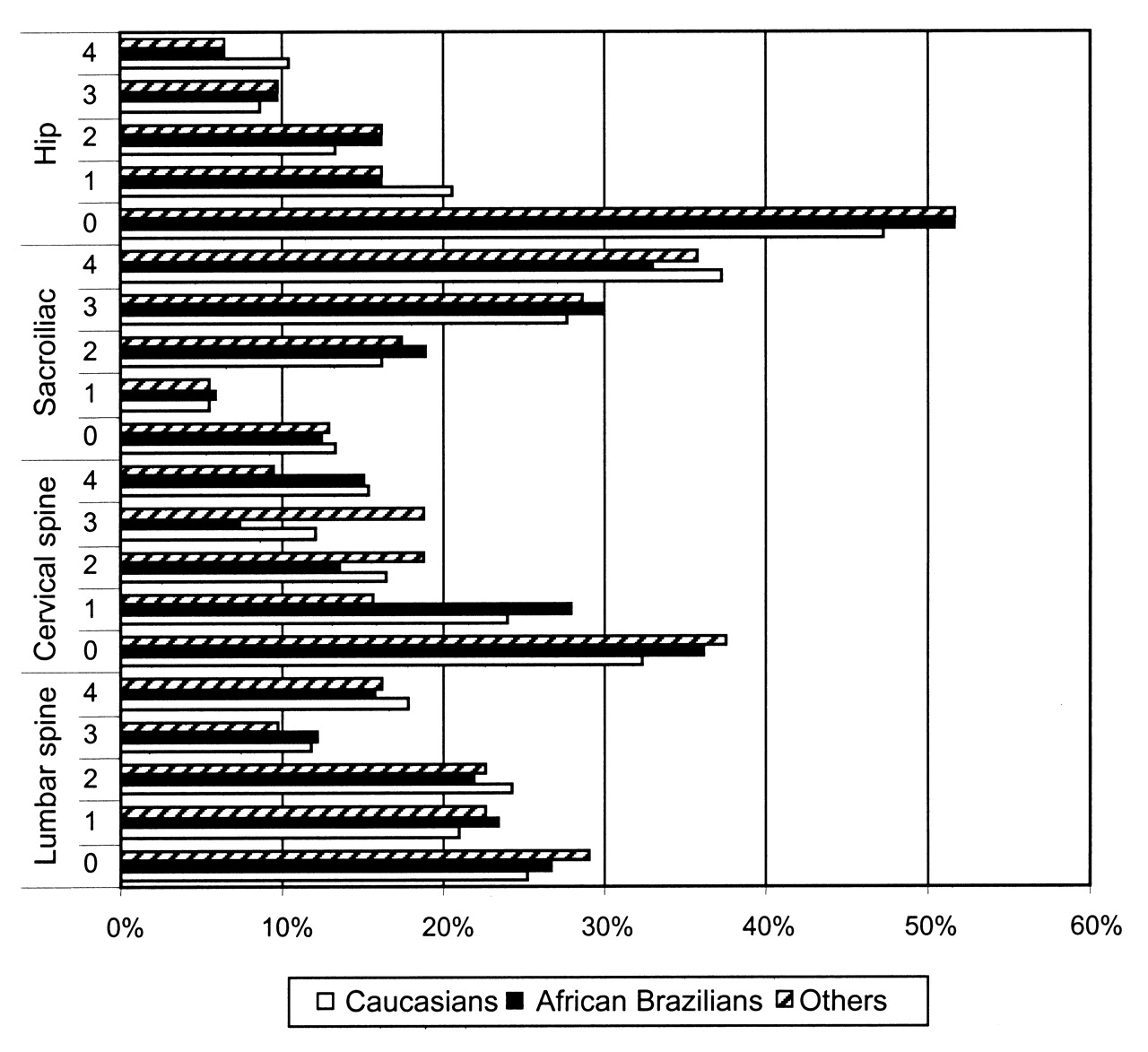
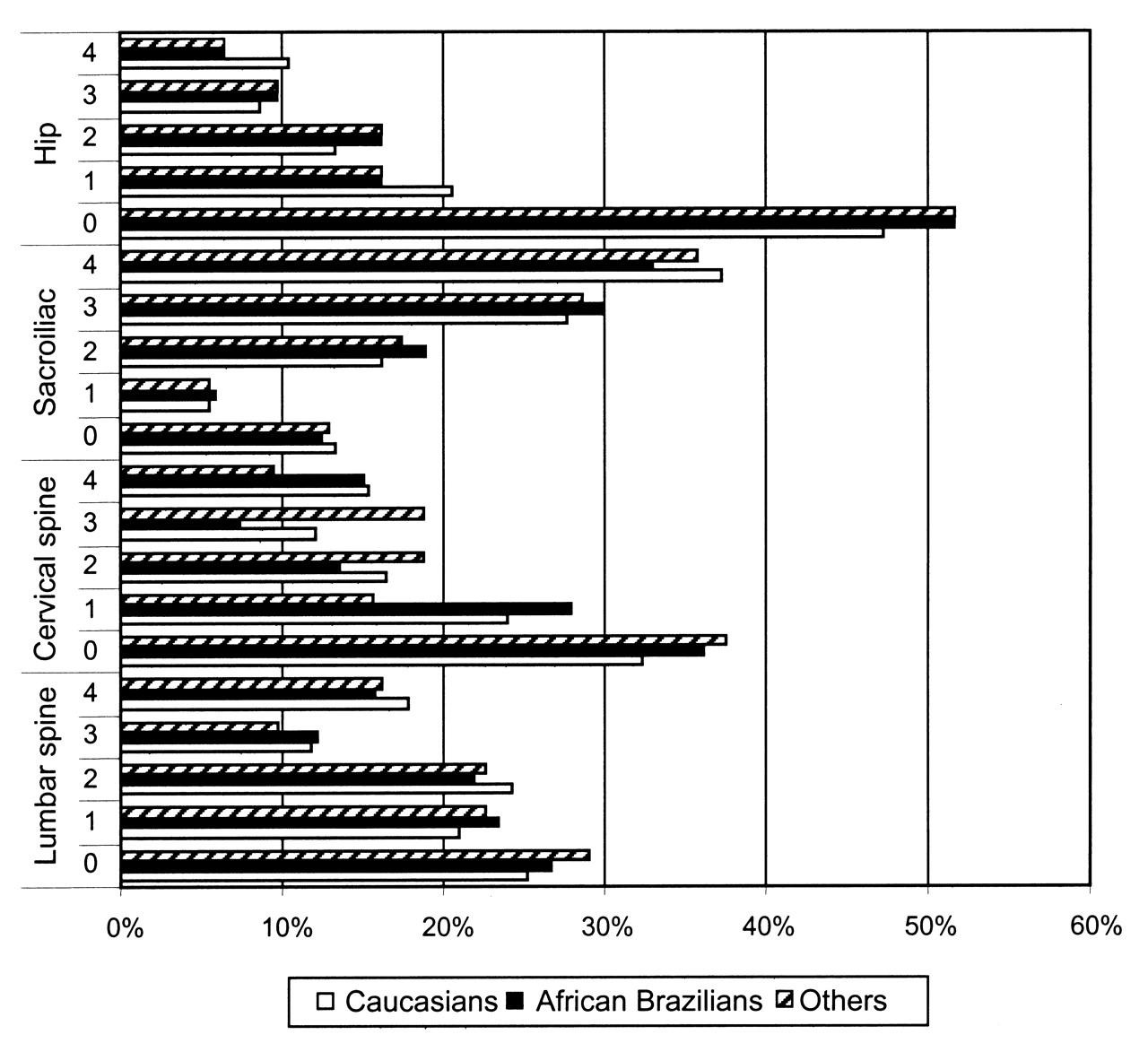
Although physician’s global assessment of disease was similar in the 3 groups, African Brazilians reported a worse patient global disease assessment (p = 0.011). BASDAI and BASFI scores and prevalence of work incapacity were not different in the 3 groups, although African Brazilians had worse performance in the ASQoL (Table 4). BASRI indexes (total and hip) showed no significant differences among the ethnic groups. The analysis of radiographic findings is summarized in Figure 2.
{kind=link}
{kind=link}
Bath Ankylosing Spondylitis Radiologic Index (BASRI) scores in 1318 Brazilian patients with SpA, according to ethnic background.
Data on inflammatory activity, function, and quality of life in 1318 Brazilian SpA patients.
DISCUSSION
In this large series of Brazilian patients with SpA, representing the 5 major geographic areas, a striking white (European ancestry) predominance was observed (65%), higher than that of the general Brazilian population (48.7%). White patients presented statistical associations with psoriasis and HLA-B27. A population-based study in the United States estimated that the prevalence of psoriasis was twice as common in whites than in African Americans (2.5% vs 1.3%, respectively)22. PsA is also more common in whites than in Asians and West Africans23; most African Brazilians are of West African descent24. HLA-B27 is characteristically associated with white SpA populations2, as also observed in several Brazilian series25,26,27,28,29.
African Brazilians represented 31.3% of the SpA patients; 25.5% had mixed white and black origin (lower than the general Brazilian population), although 5.8% referred to pure black ancestry (similar to the general Brazilian population). African Brazilian patients with SpA presented statistical associations with inflammatory back pain, radiographic sacroiliitis, hip involvement, and higher MASES scores. It is interesting that, despite similar mean scores on BASDAI, BASFI, and BASRI, African Brazilian patients with SpA reported higher mean ASQoL scores and a worse patient global assessment. These data, representing a lower quality of life, can result from different reasons, including the genetic background, the influence of socioeconomic factors (such as access to health services and access to treatment), and earlier exposure to infections. In our series, the time from initial symptoms to diagnosis was similar in whites and African Brazilians, as was the access to conventional disease-modifying antirheumatic drugs and TNF blockers. Exposure to infectious trigger events, associated with ReA, was similar in both ethnic groups. Socioeconomic factors can influence the SpA profile — patients with SpA from Ibero-America with lower socioeconomic status are younger at disease onset, present more tarsitis and limited cervical spinal mobility, and have higher BASFI scores9.
It is important to emphasize that these data were obtained through rheumatologists, who are usually gathered in larger urban centers, and thus the data may not represent the reality of small cities and rural areas. Most cases from the RBE are seen in public health services linked to universities, and once patients start treatment in these services, they have free access to all medications, including the most expensive, such as anti-TNF-α agents. However, social and economic factors may affect the patients’ access to these services and the African Brazilians may have reached these centers later than the whites. African Brazilians usually belong to a poorer social stratum. Since 1998 an increase in income of this ethnic stratum has been observed, but there is still a great difference compared to whites: in 2008, 75% of the population with lower income in Brazil had black origin, while only 15% in the highest income were black30. Although socioeconomic and regional disparities remain large in Brazil, a country of continental dimensions, the advent of the Unified Health System increased access to healthcare for a substantial proportion of the population31,32.
In our study, the percentage of HLA-B27-positive cases in African Brazilian patients with SpA was 62.4%, significantly higher than that observed in African studies, in which frequency of HLA-B27 varied from 0 to 55%5,6,33,34. The HLA-B27-negative African patients with SpA characterize a profile with later disease onset, absence of family history, and rare extraarticular manifestations6. Nonetheless, our data are similar to those from the United States, where a study showed that HLA-B27 was present in more than 80% of white patients and nearly 60% of American blacks35. These data demonstrate that HLA-B27 can be more significant in the characterization of SpA in Whites than in African Brazilians. AS was the most frequent SpA in our series, similar to that observed by Reveille in the North American population36, but different from findings from Argentina (another South American country), where the most frequent SpA was PsA37.
Acute anterior uveitis (AAU) is considered the most frequent extraarticular manifestation in SpA; it was reported by 30%–50% of patients with AS in a longterm followup study38. In our series, AAU was present in 20% of whites and 17% of African Brazilians, without significant differences between them. In spite of the strong association between AAU and HLA-B27, other genetic markers can explain the difference of this finding in the study population38, such as HLA-DR8 and HLA-B60 in patients with salmonella-induced arthritis and uveitis39,40, as well as polymorphism in LMP-2, an HLA-linked proteosome subunit gene41.
Latin American patients are known to present more frequent and significant peripheral arthritis compared to Europeans9. In our series, upper and lower limb arthritis was found in nearly half the patients with SpA, regardless of the ethnic groups. This finding differs from that of Burch, et al6, that black patients from South Africa have more peripheral arthritis compared to white patients. Interestingly, we found that the small joints of the feet were more commonly affected in those of black origin. The presence of tarsitis has been linked to poorer socioeconomic status9. Despite the higher MASES scores in the African Brazilians, there was no specific entheseal involvement related to race. Other clinical measures that have shown similar distributions according to ethnic background were sex, family history, dactylitis, urethritis, and IBD.
The differences observed in clinimetric measures were not always associated with spine complaints; whites showed a higher occiput-to-wall distance although they did not present complaints of worse cervical spine; African Brazilians presented worse lateral flexion, possibly related to the more significant complaints of inflammatory low back pain.
Brazilian patients with SpA had different patterns of disease according to their ethnic background. White Brazilian patients with SpA had a higher prevalence of HLA-B27 and skin and nail psoriatic findings; while African Brazilians had more hip involvement, higher enthesitis scores, and more inflammatory low back pain and radiographic sacroiliitis, and also a poorer quality of life that was explained by a higher prevalence of painful musculoskeletal manifestations.
Footnotes
-
The Brazilian Registry of Spondyloarthritis is supported by an unrestricted grant from Wyeth/Pfizer Brazil. Dr. Sampaio-Barros is a recipient of a research grant from the Federico Foundation.
- Accepted for publication August 4, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.