
Abstract
Objective. To describe the clinical findings and prevalence of patients with cryofibrinogenemia (CF) and to determine whether CF is associated with primary Raynaud’s phenomenon.
Methods. Between June 2006 and December 2009, 227 patients were tested for CF in a single university hospital. Forty-five patients with primary Raynaud’s phenomenon were tested for CF.
Results. A total of 117 patients with CF without cryoglobulinemia were included. The main clinical manifestations included skin manifestations (50%) and arthralgia (35%). There were 67 patients with primary CF and 50 patients with secondary CF. There was no significant difference in the mean concentration of the cryoprecipitate in primary CF as compared to the secondary form (172 ± 18.6 vs 192 ± 20.9 mg/dl, respectively; p = 0.41). Highest concentrations of cryoprecipitate were observed in those containing fibrinogen only as compared to cryoprecipitates containing fibrinogen and fibronectin (301 ± 43.5 vs 125 ± 10.6 mg/dl; p < 0.001). Patients having skin necrosis (n = 3) had significantly higher values of cryofibrinogen compared to those without necrosis (638 ± 105 vs 160 ± 10.2 mg/dl; p = 0.0046). Among the 45 patients with primary Raynaud’s phenomenon, 36 had associated CF. There was no significant difference in the mean concentration of the cryoprecipitate in these patients compared to those with primary CF.
Conclusion. There seems to be a significant correlation between cryofibrinogen concentration and the severity of the clinical signs, particularly when cryoprecipitate is composed of fibrinogen alone. CF might have a possible pathophysiological role in primary Raynaud’s phenomenon.
- CRYOFIBRINOGENEMIA
- RAYNAUD’S PHENOMENON
- VASCULITIS
- AUTOIMMUNE DISEASE
Cryofibrinogenemia (CF) is considered a rare disease, initially described in 1955 by Korst and Kratochvil1. Cryofibrinogen is a precipitate arising in plasma cooled at 4°C and which becomes soluble again when the temperature of the sample is brought back to 37°C. The cryoprecipitate consists of fibrinogen, fibrin, fibronectin, and smaller amounts of various proteins2. Cryofibrinogen is easily distinguishable from cryoglobulin because it can be detected only in plasma and not in serum. Although primary CF is rare, its prevalence is not known and data might still be underestimated due to the lack of awareness of this entity by many physicians. An overall prevalence of 3.4% has been reported in hospitalized patients3. CF may be classified as primary (or essential or idiopathic) or secondary4. Several disease processes have been associated to the secondary form of CF including autoimmune diseases, malignancies, infections, drugs, and thromboembolic conditions5,6. Familial forms of CF have been described but the pathophysiological significance remains to be resolved7. It is also notable that CF could be detected in healthy asymptomatic persons8,9,10. The prevalence of CF in healthy subjects has been estimated to be from 2% to 9%8. In these studies, the amounts of cryofibrinogen were classically < 50 mg/dl as compared to significantly higher levels in patients with symptomatic CF in whom the levels are > 500 mg/dl8,10.
The pathogenesis of CF remains unknown. One possible etiopathological clue might be the high level of plasma protease inhibitors (α1-antitrypsin and α2-macroglobulin) found in patients with CF8,10. These proteins inhibit plasmin activity, blocking fibrinolysis, and hence enhancing fibrinogen concentration that decreases its solubility, thereby favoring thromboembolic events. The clinical manifestations of CF are protean and include Raynaud’s phenomenon (RP), painful ulcers, livedo reticularis, purpura, and in more severe forms gangrene and ischemic necrosis8,9,10,11,12.
Because of limited data on CF, consisting primarily of isolated case reports and small series, the clinical significance of CF is not well known. We retrospectively analyzed all patients presenting with CF from June 2006 to December 2009. We determined the levels of cryofibrinogen in patients presenting with primary RP in order to determine a possible pathophysiological role in that condition.
MATERIALS AND METHODS
Patients
We retrospectively analyzed by chart review the clinical and biological characteristics of 227 patients who had undergone testing for cryofibrinogen in the Immunobiology Department of Erasme University Hospital between June 2006 and December 2009. Patients were recruited from the internal medicine, rheumatology, and vascular clinics. Indications for cryofibrinogen testing were mainly acrosyndromes, polyarthralgia and polyalgia, neurological symptoms (suggestive of multineuritis or cerebrovascular disease), and skin manifestations (livedo, purpura, urticaria). The mean age of patients was 45.7 ± 1.37 years. All patients were tested at least twice for CF and cryoglobulinemia. Patients who were positive for cryoglobulinemia were excluded. For every patient, data were collected concerning clinical features, hemogram, presence of antinuclear antibodies, rheumatoid factor, and complement and α1-antitrypsin and α2-macroglobulin levels (evaluated by quantification of α-1 and α-2 fractions by serum electrophoresis). In cases of thrombotic events, levels of antiphospholipid antibodies, anticardiolipin antibodies, lupus anticoagulant, plasma homocysteine, C protein, and S protein were determined and antithrombin deficiencies, mutations for factor V Leiden, prothrombin, and methylene-tetrahydrofolate-reductase were investigated. Autoimmune and connective tissue diseases and vasculitis were diagnosed according to standard criteria. Diagnosis of infections was based on hemocultures and microbiological investigations.
Raynaud’s phenomenon was considered as primary on the basis of absence of secondary cause, absence of ulcerations, tissue necrosis or gangrene, symmetric attacks, normal nailfold capillaries, negative antinuclear antibodies, and normal erythrocyte sedimentation rate (ESR).
Analysis of cryoprecipitate
Using previously warmed equipment, blood was collected into EDTA-containing tubes that were kept at 37°C until centrifugation (2000 g, 10 min). The plasma was immediately chilled at 4°C for 8 days, then presence of a precipitate or gel formation was evaluated. For the positive samples, the reversible property of the cryoprecipitate was checked by heating the plasma at 37°C. The composition of the cryoprecipitate was then analyzed by immunofixation electrophoresis (IFE) after a purification step consisting of 2 washes with ice-cold 0.9% NaCl, 5 mM EDTA. The washed precipitate was loaded on the gel, and the immunofixation performed using the Hydragel 9IF kit on a Hydrasys 2 instrument (Sebia, Vilvorde, Belgium) with the following tracks: fixative solution (total IFE), pentavalent antiserum (anti-human-IgG, −IgA, −IgM, −kappa light chains, −lambda light chains; Sebia), antihuman fibrinogen (Dako, Zebra Biosciences, Enschede, The Netherlands), and antihuman fibronectin (Dako). A second aliquot of the cooled plasma was washed in the same way, except that the cryoprecipitate was redissolved by adding 0.1 M NaOH, the added volume of 0.1 M NaOH being equivalent to the volume of plasma discarded after the first wash. The concentration of the precipitate was finally determined by measuring the optical density at 280 nm and calculated using the calculation (OD280 / 0.66) x 100, which gives the concentration in mg/dl. The cryoprecipitate was characterized according to the different constituents into fibrinogen; fibrinogen and fibronectin; and fibrinogen, fibronectin, and immunoglobulins.
Nailfold capillaroscopy
Capillaroscopy was performed in patients with RP by 2 experienced physicians specialized in vascular pathology. A drop of grade B immersion oil was placed on the patient’s skin at the base of the fingernail and the corresponding area was viewed and analyzed with a stereoscopic microscope by transillumination.
Statistical analysis
Statistical analysis was performed with GraphPad prism 5.0 software (GraphPad Software, San Diego, CA, USA). Comparisons between groups were by Mann-Whitney U test. All values are expressed as the mean ± SE of the mean (SEM). P values < 0.05 were considered statistically significant.
RESULTS
After excluding 5 patients positive for a cryoglobulin, 227 patients were tested for cryofibrinogen: 117 were positive and 110 were negative. Forty-five patients presenting with primary RP were also tested for cryofibrinogen, among which 36 patients were positive.
Primary and secondary CF
Table 1 shows the clinical features and characteristics of the 117 patients with CF. There were 67 patients with primary CF and 50 patients with secondary CF. Patients presenting with primary CF did not have any biologic features of systemic disease, with normal C-reactive protein levels and normal ESR. There were no low levels of complement C3 or C4. Rheumatoid factor, antinuclear antibodies, and antiphospholipid and anticardiolipin antibodies were also negative. There were no detectable increases in the values of α1-antitrypsin and α2-macroglobulin. Patients with primary CF mostly had RP (54%), cold sensitivity (57%), arthralgia (18%), and neurological disorders (cerebrovascular disease and multineuritis: 15%). Interestingly, clinical manifestations were similar for the patients with secondary CF, but with the frequency of the 2 first inverted, i.e., arthralgia at 58% and RP at 24%; cold sensitivity was reported to be 25%, while neurological disorders (cerebrovascular disease, infections of central nervous system, and multineuritis) occurred at the same frequency (15%). This difference of the frequency of arthralgia and RP between primary and secondary CF was statistically significant (p < 0.05, Mann-Whitney U nonparametric test).
The main characteristics of patients with cryofibrinogenemia (CF); comparison of the clinical findings and outcome between patients with primary CF and secondary CF.
The diseases associated with secondary CF are summarized in Table 2. Autoimmune diseases and vasculitis represented 84% of the etiologies of secondary CF. In addition, there were 5 infectious causes and 4 cases related to hematological cancers.
Diseases associated with secondary cryofibrinogenemia.
Cryoprecipitate analysis in primary and secondary forms of CF
Figures 1A and 1B represent the characterization of the cryoprecipitate in primary CF and secondary CF. In the primary forms, the cryoprecipitate contains mostly fibrinogen (36%), fibrinogen plus fibronectin (41%), and sometimes fibrinogen, fibronectin, and polyclonal immunoglobulins (23%). In contrast, the cryoprecipitate in the secondary forms is essentially composed of fibrinogen; fibronectin and immunoglobulins (51%); fibrinogen and fibronectin (36%); and fibrinogen only (13%).

Differential analysis and concentrations of cryoprecipitates in primary (A) and secondary (B) cryofibrinogenemia.
The mean concentration of the cryoprecipitate was 181 ± 13.8 mg/dl for all CF, 172 ± 18.6 mg/dl for patients with primary CF, and 192 ± 20.9 mg/dl for patients with secondary CF (p > 0.05 for cryoprecipitate values among different groups). Patients with CF presenting with fibrinogen exclusively, for primary as well as for secondary CF, had significantly higher values compared to those with fibrinogen and fibronectin and immunoglobulins (Figure 1).
CF associated with skin necrosis and Raynaud’s phenomenon
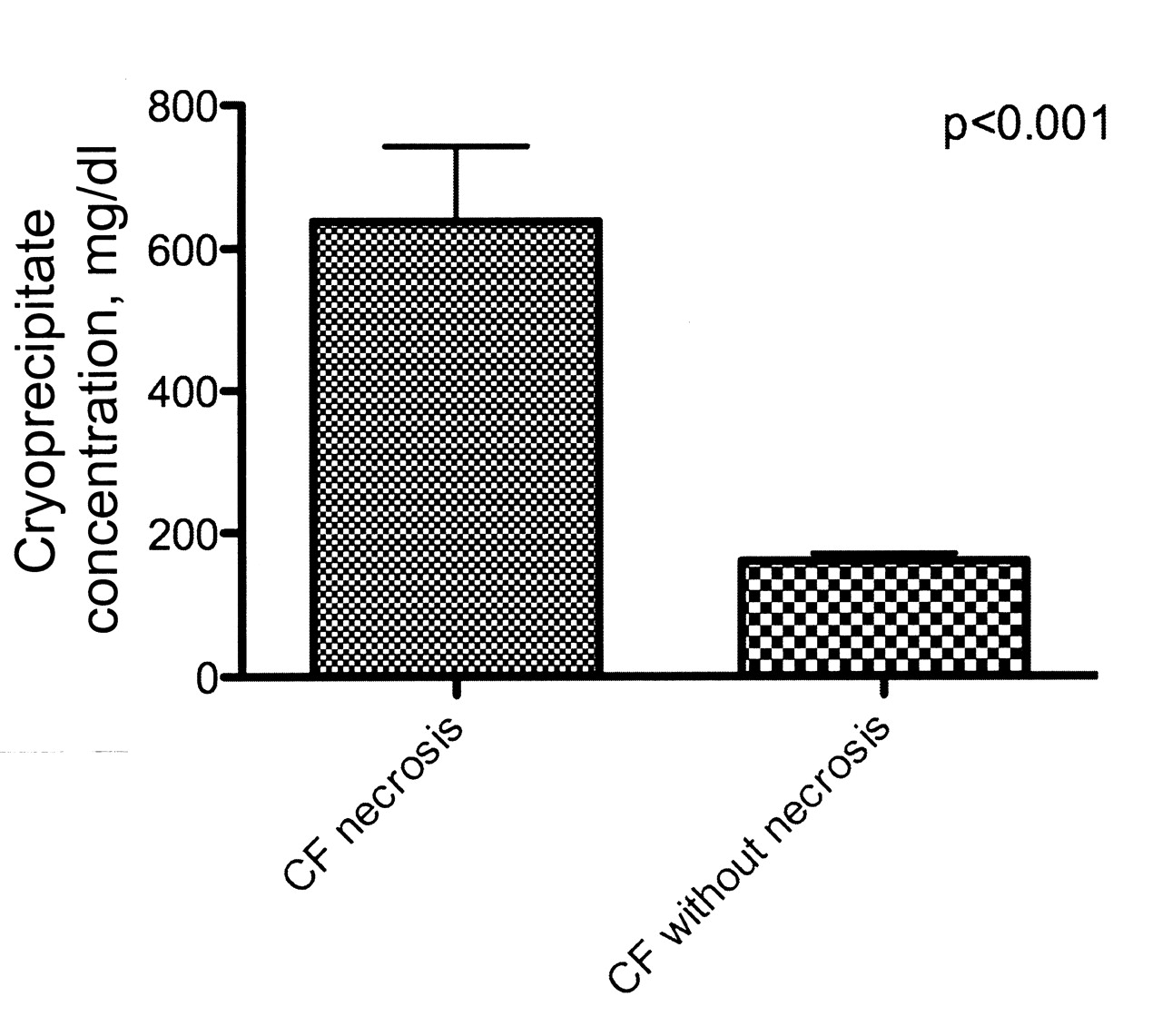
The highest values of cryofibrinogen were observed in patients (n = 3) presenting with skin necrosis and gangrene (mean value 638 ± 105 mg/dl, median 561 mg/dl), compared to 160 ± 10 mg/dl for the other patients without necrotic manifestations (p < 0.01; Figure 2). These patients had a cryoprecipitate composed only of fibrinogen. Treatment of these patients (2 were treated with intravenous heparin and 1 with cyclophosphamide and methylprednisolone) resulted in normalization of cryofibrinogen levels.
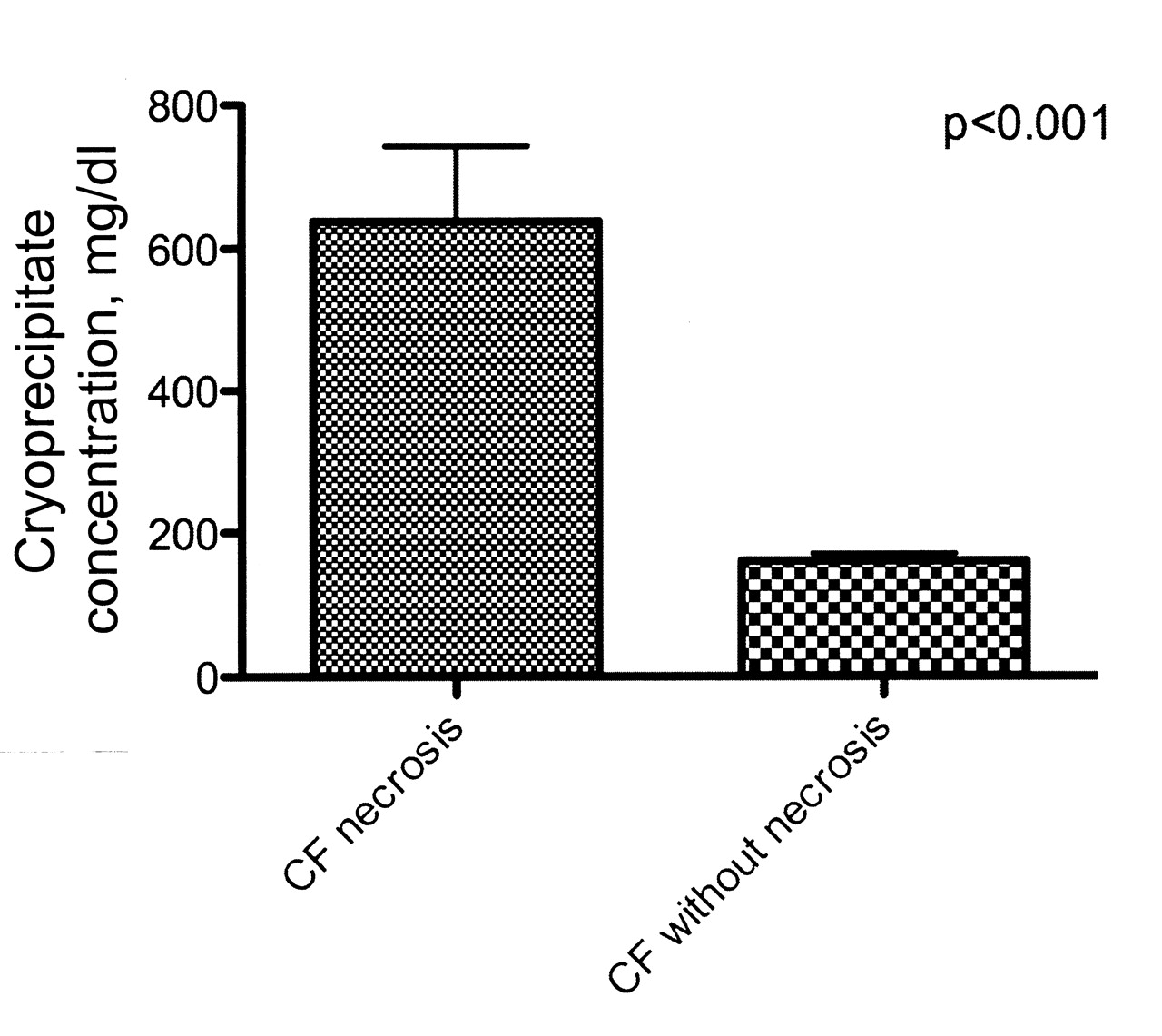
Comparison of cryoprecipitate concentrations in patients with cryofibrinogenemia (CF) with and without necrosis. Patients with necrosis had significantly higher levels of cryoprecipitate concentration compared to those without necrosis (p < 0.001).
RP appeared to be the most frequent complaint associated with CF. Indeed, RP was observed in more than half the patients (54%) with primary CF, with a cryoprecipitate concentration of 115 ± 11.3 mg/dl, which is lower compared to patients presenting with secondary CF (p = 0.01; Figure 3). Our study confirms that RP largely affects women (78%), and revealed that this clinical entity is associated with a cryoprecipitate principally composed of fibrinogen and fibronectin (Table 3).

{kind=link}
{kind=link}
{kind=link}
Comparison of cryoprecipitate concentrations in patients with cryofibrinogenemia (CF) and primary Raynaud’s phenomenon (RP), primary CF, and secondary CF. Patients with primary RP had significantly lower cryoprecipitate concentration compared to patients with secondary CF (p < 0.01).
Characteristics of patients (n = 36) with primary Raynaud’s phenomenon associated with cryofibrinogenemia (CF). Values are mean ± SE of the mean.
DISCUSSION
We retrospectively analyzed data from patients presenting with CF. From June 2006 to December 2009, 122 out of 232 patients were tested and found to be positive for CF. Among the 122 patients, 5 were excluded because they tested positive for cryoglobulinemia. We found 67 patients with primary CF and 50 patients with CF-associated disease. Ours is the first study with a higher prevalence of CF as compared to others, which highlights that CF is still an underestimated disease. The diagnosis of CF is based on the detection of plasma cryofibrinogen and on the presence of clinical signs and symptoms or characteristic skin biopsy8. False-negative CF results could be due to improper technical processing such as blood collection at < 37°C, blood sampling in adequate solutions, or the use of sera instead of plasma13,14. A false-positive result may occur if heparin is present as an anticoagulant in the blood collection tube or from therapeutic use, because it can complex with fibrinogen, fibrin, and fibronectin15,16,17,18. In our study, blood sampling for analysis of cryofibrinogen was performed in EDTA tubes, whereas in other series, collection was carried out in citrate or oxalate tubes. Even though the potential inhibition of cryoprecipitation of fibrin-fibrinogen complexes by EDTA has been reported by the Blood Research Foundation, there are scant data supporting this. On the other hand, there are several lines of evidence supporting the use of the 3 types of anticoagulants (citrate, oxalate, and EDTA) for detection of plasma cryofibrinogen.
In accord with the previous studies on CF, skin involvement and arthralgia were the most frequent manifestations8,9,10. However, our study differs by the higher prevalence of primary CF compared to the findings of Saadoun, et al10. We had an increased incidence of CF in patients with primary RP as compared to other studies and more specifically the French studies. This might be explained by the fact that we searched systematically for the presence of CF in patients with RP, as we had previously observed increased levels of cryofibrinogen in some patients. The possible role of CF in primary RP has not previously been suggested. The levels of cryofibrinogen in this subgroup of patients were not significantly lower than those found in other causes of primary CF, but were significantly lower than those encountered in secondary CF. In addition, patients with RP-associated CF did not present with more severe vascular manifestations, compared to those without CF. Patients with primary RP and CF did not progress to secondary RP due to underlying diseases. Whether CF could be responsible for the primary RP may not be assumed by results from our study, but our observation clearly delineates a possible new pathophysiological pathway, which needs to be confirmed by systematic determinations of CF in a larger series of patients with RP.
Higher values of CF were seen in patients presenting with skin necrosis or gangrene. This observation contrasts with that of Blain, et al8, and suggests a possible clinical correlation between CF levels and disease severity. This line of evidence clearly highlights the role of cryofibrinogen in obstructing blood vessels and interfering with blood flow with ensuing thrombosis and ischemia. It is also notable that treating these patients resulted in progressive normalization of CF, and regular control of CF is therefore recommended for such patients. The role of CF in thrombotic events has been highlighted by Saadoun, et al10. The authors described a prevalence of 40% for thrombotic events in their patients with CF. Further, a defect in the fibrinolytic process was reported in primary CF, highlighted by increased levels of α1-antitrypsin and α2-macroglobulin and a delayed euglobulin lysis time10. The corollary of this defect in the fibrinolysis process results in cryofibrinogen formation and ensuing blood clotting. This process might be further exacerbated by reflex vasospasm, vascular stasis, and hyperviscosity. In our patient cohort we did not find significantly increased serum levels of α1-antitrypsin and α2-macroglobulin. Determination of α1-antitrypsin and α2-macroglobulin was not performed in our analysis of the cryofibrinogen cryoprecipitate, and thus we cannot rule out the potential contribution of these proteins in the pathophysiology of the disease process, as described in other studies. However, on the basis of normal serum levels of α1-antitrypsin and α2-macroglobulin, this raises the possibility that pathophysiogical processes are involved other than the defect in the fibrinolysis pathway.
We further characterized the cryofibrinogen cryoprecipitate into its different major components (fibrinogen, fibronectin, and immunoglobulins). Fibronectin has been advocated to be able to bind fibrin and fibrinogen and act as a nucleus for cold-induced cryoprecipitation of fibrinogen-fibrin complexes2. Fibronectin within the cryofibrinogen complex may also interact with circulating immunoglobulins or immune complexes, and therefore contribute an inflammatory component to the potentially prothrombotic character of CF15,19. The potential role of an immunological mechanism underlying the pathophysiology of CF associated with malignancies, infections, and autoimmune diseases could be plausible. Most of the patients had cryofibrinogen cryoprecipitate composed of fibrinogen and fibronectin, followed by fibrinogen, fibronectin and immunoglobulins, and only 29 patients had cryofibrinogen cryoprecipitate with fibrinogen exclusively. Patients having cryofibrinogen cryoprecipitate composed exclusively of fibrinogen had higher values of cryofibrinogen compared to others. Further, these patients presented with more severe complications of CF as indicated by cases of skin necrosis and tissue ischemia. This observation might thus suggest that cryofibrinogen cryoprecipitate composed exclusively of fibrinogen causes more severe “in-situ” thrombosis and corollary ischemia and necrosis. Whether the severe skin manifestations due to cryofibrinogen cryoprecipitate associated with fibrinogen are due to fibrinolysis defects or are a result of altered thrombin-binding capacities remains unknown8. We did not find increased levels of plasma α1-antitrypsin and α2-macroglobulin in these patients, which might suggest increased thrombin-binding capacities and clot formation as more likely than a fibrinolysis defect. Paradoxically, plasma levels of fibrinogen in these patients were not significantly increased. This observation is in agreement with the report of Blain, et al8. They found that fibrinogen levels were not increased in cases of primary CF accompanied by recurrent cutaneous lesions, suggesting that CF in that subgroup of patients does not merely reflect elevated plasma fibrinogen levels. Further studies are needed in the potential role of fibrinogen in the pathophysiological process of cryofibrinogen-associated thrombosis.
It has been reported that one of the possible outcomes of primary CF is lymphoma8,20. Thus, patients initially classified as having primary CF may actually have underlying lymphoma20. In our investigation, only 1 patient had lymphoma, and with a 2-year followup we did not observe the development of lymphoma in our patient group. A longer period of followup of our patients would be needed to corroborate the findings of the French multicenter study20. The reports of Belizna and colleagues9,20 highlight the importance of regular followup of patients with primary CF.
Cryofibrinogenemia is a clinical entity that is still underestimated by many clinicians; the high prevalence observed in our study shows that it might not be such a rare disease. CF should be included in the differential diagnosis of thrombosis, skin ulcerations, and ischemia and necrosis. CF might be involved in the pathophysiological process of primary Raynaud’s phenomenon. This finding must be confirmed by further studies with larger series of patients.
- Accepted for publication August 31, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.