

In the early hours of the morning of August 31, 1997, Diana, Princess of Wales, was a passenger in a Mercedes-Benz being driven at high speed through the fashionable 8th Arrondissement of Paris. Passing through a tunnel along the Seine River, the vehicle ran into a wall. An ambulance took her to the decidedly unfashionable 13th Arrondissement, where she was pronounced dead about 2 hours later at La Salpêtrière Hospital.
La Salpêtrière, or saltpeter works (intriguing name for a hospital!), the largest hospital in Paris, has a fascinating history. About 400 years ago, an arsenal for the manufacture of munitions was relocated to the present Salpêtrière site from across the river. Since gunpowder is largely a mixture of sulfur and saltpeter (KNO3), the site was referred to as the saltpeter works. This appellation has been applied to the successive institutions that have stood on this site, and persists to this day.
Under Louis XIV, who reigned from 1643 to 1715, a large proportion — estimated as high as 10% — of the Paris population of 400,000 were homeless beggars. They were not just underprivileged, they had nothing: no money, no honest way to earn money, nothing to eat, nowhere to live. They were dressed in rags. Of course they had some alternatives: crime, begging, prostitution, and suicide. All these alternatives were employed. Clearly, this situation had the potential for major social disorder.
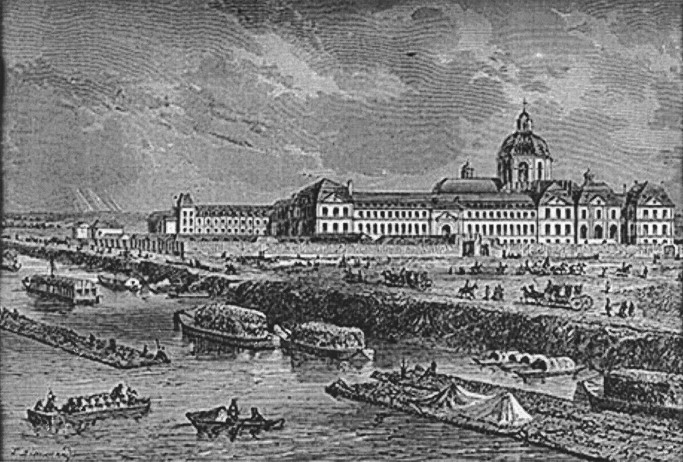
At the same time, the middle of the 17th century saw the rise of concern for the poor, spearheaded by the efforts of St. Vincent de Paul. His influence, combined with the perceived need for greater social stability, prompted the King in 1656 to remove undesirable members of society from the streets by sheltering them in grand settings1. His motivation: “to put an end to beggary and idleness, as being the source of all disorder.” All paupers were to be housed at the new Hôpital Général, with separate sections for men, boys, and women2. Women were housed in a large complex of buildings erected on the site of La Salpêtrière1 (Figure 1). These Parisian institutions became a gigantic alms-house into which 10% of the population of Paris was herded: the feeble-minded, criminals, outcasts, homeless, epileptics, and paralytics. These “hospitals” did not care for the sick. They were only shelters, places of asylum.
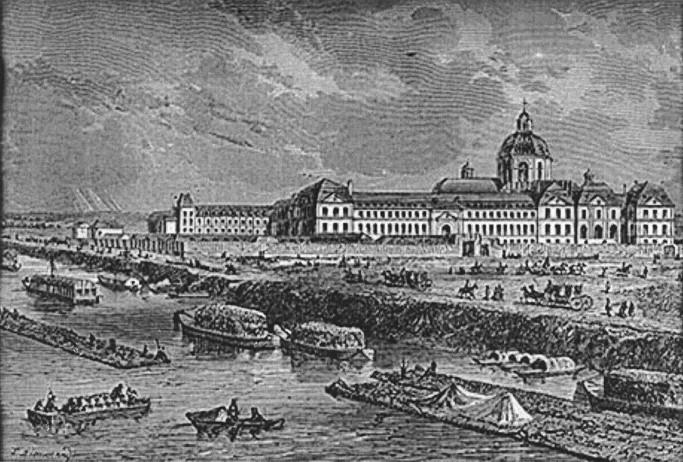
La Salpêtrière toward the end of the 17th century. From Goudon de Genouillac. Paris a travers les siecles. Paris; 1882. Courtesy Musée de la civilisation, bibliotheque du Séminaire de Quèbec, fonds ancien.
Yet another class of homeless people was also felt to need attention. Accordingly, Les Invalides was constructed in Paris to house wounded war veterans in 1671. (I like to refer to this as the first modern veterans administration hospital.) Charles II of England, not to be outdone, followed Louis’ example. A decade later he established the Royal Hospital in Chelsea, now London, to care for wounded veterans of his army.
By 1684, the problem of prostitution was felt to have worsened, and a prison was established at La Salpêtrière for women “guilty of debauchery and scandalous prostitution.” A major roundup occurred; the welcoming bouquets of laurel that had been used to indicate the doors of the hospitable and accommodating ladies were cut down, giving rise to a song of lament: Nous n’irons plus au bois, les lauriers sont coupés. (We go to the woods no more; the laurels have been cut down.) This enchanting tune has since evolved into a beloved children’s folk song.
Throughout the first half of the 18th century, roundups of homeless women served an additional state and commercial purpose. Settlers were needed to populate the French possessions abroad — to become the mothers of a new population of North Americans of European ancestry1. They were drafted; they had no option of refusal. Thousands of women were sent to La Salpêtrière and then forwarded to the New World to be spouses for the men already there. The men at the receiving port generally drew lots the night before their arrival and then selected from the new arrivals accordingly. The next morning, after a mass marriage, they set out for their new lives. (Many years later, an impoverished Italian composer, Giacomo Puccini, achieved his breakthrough success with the opera Manon Lescaut, whose heroine was locked up for debauchery in the prison section of La Salpêtrière before being deported to the New World.)
In September 1792, during the French Revolution, La Salpêtrière became the site of one of the terrible massacres that took place in Paris. A frenzied, drunken mob assaulted La Salpêtrière. By the time they got there, alcohol had overcome their original good intention of freeing the women, and their enterprise turned into an orgy of blood. Forty-five women were dragged into the street, mutilated, and massacred, while many were raped.
Before the Revolution, La Salpêtrière had been the largest hospice in the world. There were 10,000 women in 15 buildings, comprising a poorhouse, a prostitutes’ prison, a girls’ reformatory, a prison for female criminals, and a madhouse. After the Revolution, hospitals were transformed: hospitals, reserved for the sick, and hospices, philanthropic residences reserved for orphans or old people, etc., were now separated from the prisons. The prison of La Salpêtrière was eliminated in 1795, leaving a hospice for the homeless, sick, incurable, and insane women.
At the same time, a revolution in medicine was occurring in Paris, driven by one of the philosophical currents that led to the French Revolution — the rejection of authority. In the opinion of many this was the beginning of the era of modern medicine. The new medicine emphasized observation and analysis, and was skeptical of the ancient texts of Galen and Avicenna. During the next half-century the hospitals of Paris became the workshops of this new medicine, and of its 3 tools: physical examination, correlation with autopsies, and clinical statistics3. For example, the stethoscope was invented by René Laennec. Percussion of the chest, ignored since its introduction 47 years earlier by Josef Leopold Auenbrugger in Vienna, was revived by Jean-Nicolas Corvisart, Napoleon’s physician. Pierre Louis began to apply statistics to medicine. After 1600 years, medicine and surgery were finally reunited.
From 1794 to about 1848, Parisian hospitals were preeminent in world medicine. Paris became the mecca for foreign medical students and practitioners. Oliver Wendell Holmes wrote home: “Merely to have breathed a concentrated scientific atmosphere like that of Paris must have an effect on anyone who has lived where stupidity is tolerated, mediocrity applauded, and excellence defied.”4
Until this time, people with psychosis were regarded as possessed — the beast within had gained control over the human faculties. They were permanently chained in dungeon-like settings and were treated by bleeding, purging, or blistering. At this point in history, several thoughtful physicians, acting independently in different countries, revolted against this approach. In France it was Dr. Philippe Pinel who set this revolution in motion. Pinel essentially introduced medical care into French mental hospitals5. He released the “wild beasts” from their chains, and some even got well6. An iconic painting of Pinel unchaining the lunatics in 1795 hangs in La Salpêtrière (Figure 2).

Philippe Pinel releasing lunatics from their chains at the Salpêtrière asylum in Paris in 1795. By Tony Robert-Fleury, 1876. From Réunion des Musées Nationaux/Art Resource, NY, NY, USA; with permission.
Once physicians started observing rather than theorizing, they noticed things they hadn’t noticed before. New clinical entities were recognized. La Salpêtrière, with thousands of aging women and chronically ill patients, constituted a living museum, a setting in which chronic diseases could be recognized for the first time.
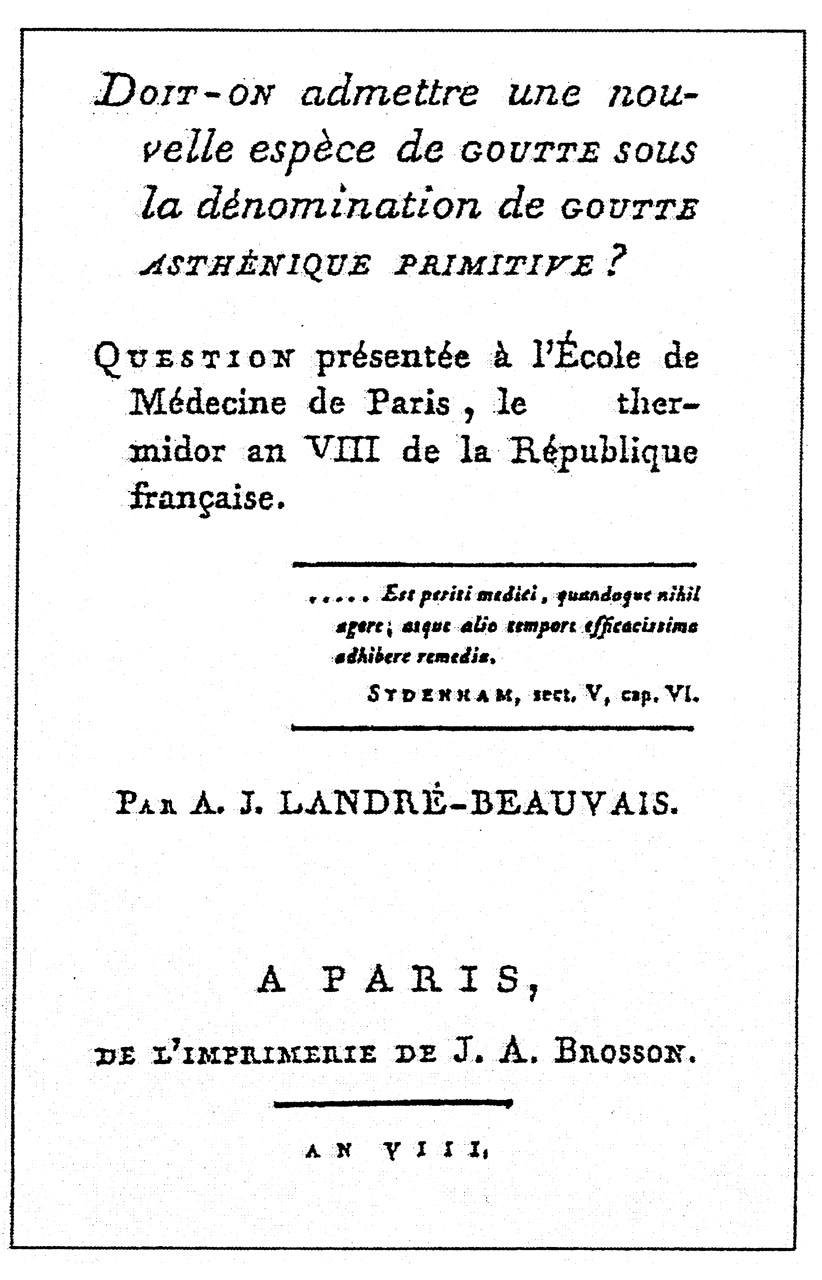
Since the time of Hippocrates, the various types of arthritis had been presumed to be gout in one form or another. In 1800, Augustin Jacob Landré-Beauvais, working under Pinel, observed what he thought might be a different kind of arthritis. He described 9 women, longterm residents of La Salpêtrière, who manifested several distinct features (Figure 3)7. While gout occurred as intermittent episodes, usually monoarticular, in otherwise vigorous and hearty men, these patients differed in several important ways. All were of course women and were often feeble and weak. They displayed a chronic course, with involvement of many joints from the outset, joint deformities, and a decline in general health. His title had a tentative tone: “Doit-on admettre une nouvelle espèce de goutte sous la dènomination de goutte asthènique primitive?” (Should we recognize a new type of gout to be called primary asthenic gout?), but the last sentence of his dissertation establishes that Landré-Beauvais was sure he was describing a new, previously unrecognized entity: “...we must recognize the existence of a new form of gout under the designation primary asthenic gout.” Landré-Beauvais’ doctoral thesis is generally acknowledged as the first formal description of rheumatoid arthritis (RA)7.

The title page of Landré-Beauvais’ doctoral thesis in which he described a new condition: rheumatoid arthritis. From Joint Bone Spine 2001;68:130–437; with permission.
In the 19th century, the inmates of La Salpêtrière were the female dregs of society: paupers, vagabonds, beggars, prostitutes, the decrepit, senile, and insane. In the middle of that century the greatest name in the history of La Salpêtrière appeared, Jean-Martin Charcot, born in 1825. Charcot is considered by many to be the founder of modern neurology. His students constitute some of the great names in the history of that discipline. At the age of 27 he began an association with La Salpêtrière. Twenty years later, a prestigious chair in neurology was created specifically for him, a position he held until he died in 1893. Although Charcot’s reputation is based on his work as a neurologist, he is best known among American physicians for his contributions to rheumatology: neuropathic joints (Charcot’s joints), which he saw primarily in women with Tabes dorsalis, a form of neurosyphilis. This was a period of rapidly arriving insights in rheumatology, when the foundations of our current understanding of rheumatic disease were laid.
Charcot’s participation and interests were not limited to neurology. His first publication — the subject of his doctoral thesis in 1853 — reminded the medical public of the somewhat overlooked disease described by Landré-Beauvais 53 years earlier: primary asthenic gout (now known as RA). In this thesis, like Landré-Beauvais before him, Charcot made good use of the abundant human material at La Salpêtrière to describe the clinical picture of RA in 40 patients.
Six years later in England, Sir Alfred Garrod published his classic treatise on gout, in which 24 of the 25 chapters were devoted to gout. Sometimes forgotten, however, is that in the additional chapter he also clearly distinguished RA from gout and rheumatic fever and gave it its name. He boldly stated that RA was “in no way related to gout, and not necessarily” to rheumatic fever. Charcot supervised the French translation of Garrod’s book by one of his own students 8 years later. He also annotated it, wrote an introduction, and added 2 colored plates of his own.
Charcot was particularly fascinated by “hysteria,” a condition that is much less common today. In his celebrated Tuesday public lectures, Charcot illustrated his findings on hysteria by live demonstrations8 (Figure 4)9. The patients put on display were young women who had found refuge in La Salpêtrière from lives of unremitting violence, exploitation, and rape. The asylum provided them with more safety and protection than they had ever known. In addition, the selected group of women who became Charcot’s star performers achieved something close to fame. It is not surprising that they put on a good show.
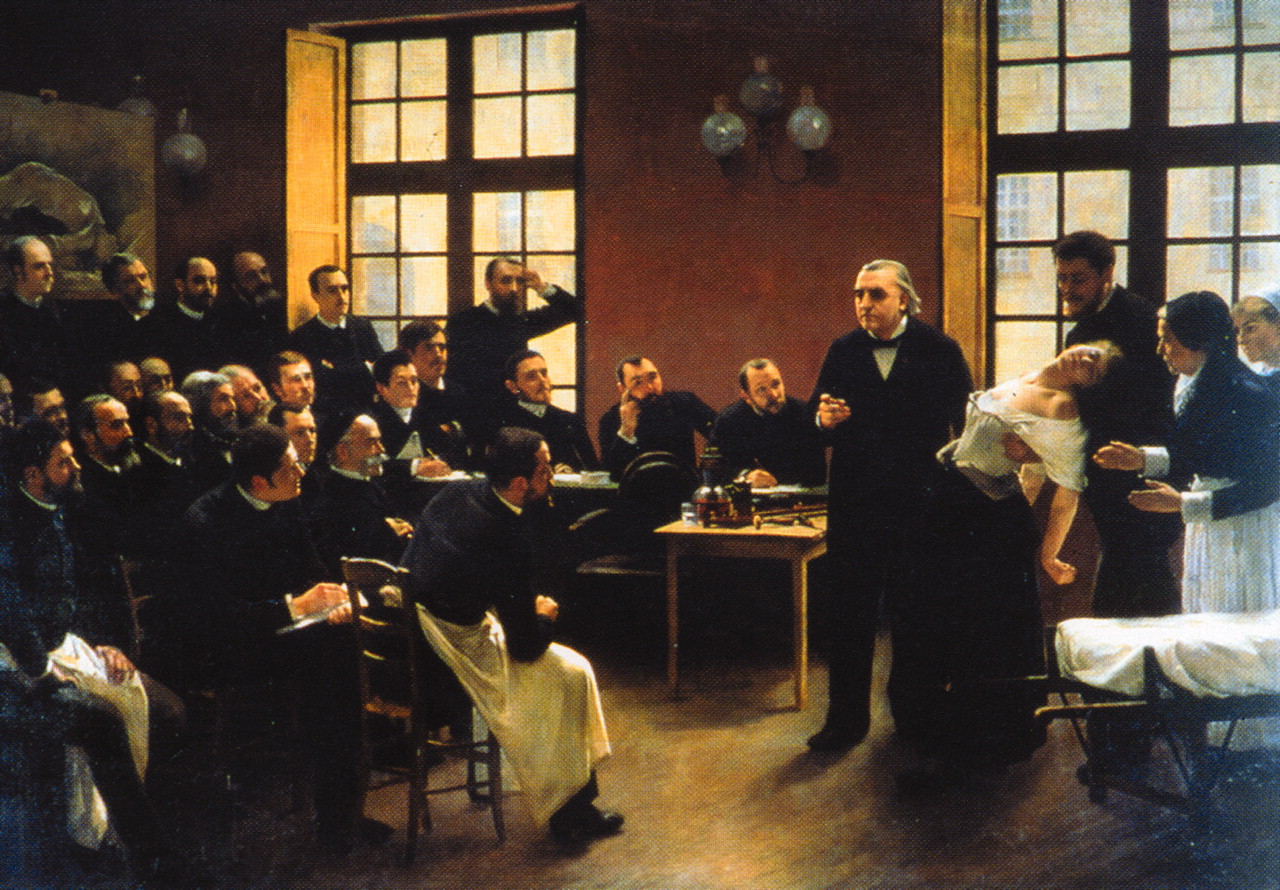
Charcot demonstrating hysteria at La Salpêtrière. By Andre Brouillet 1887. [Internet. Accessed May 11, 2011.] Available from: http://en.wikipedia.org/wiki/Jean-Martin_Charcot
Jane Avril, the Moulin Rouge dancer immortalized by Toulouse-Lautrec (Figure 5), was admitted to Charcot’s service at the Salpêtrière at the age of 149. In her memoirs, she describes the lengths the “crazy girls” would go to in order to capture attention — to become Charcot’s “stars of hysteria.” These memoirs partially explain why hysteria was regarded as contagious.

Jane Avril as depicted by Toulouse-Lautrec. [Internet. Accessed May 11, 2011.] Available from: http://en.wikipedia.org/wiki/Jane_Avril
Charcot attracted students from all over the world. At that time neurology and psychiatry had not yet separated themselves from one another, and gifted and ambitious men in these new disciplines made the pilgrimage to Paris to study with the master. Among them were Alfred Binet, William James, and an ambitious young neurologist from Vienna, Sigmund Freud. Freud’s stay at La Salpêtrière for 4 months made an indelible impression; he even named his first son after Charcot, and ultimately wrote Charcot’s obituary.
Charcot was convinced that he understood the underlying cause of hysteria. Freud once heard Charcot exclaim, very excitedly: “Mais, dans des cas pareils c’est toujours la chose génitale, toujours...toujours”. I translate this as “In cases of this type, there is always something sexual going on; always....” It is very tempting to speculate that this comment shaped Freud’s subsequent thinking.
Charcot made other contributions to rheumatology. He described urate crystals in gouty fluid, the gouty kidney, and the bony deformities of acromegaly. In his studies of hysteria, he opened the door to the still fuzzy psychophysiological dysregulation that we confront today in chronic fatigue syndrome and fibromyalgia. His student and successor Pierre Marie, following Charcot’s lead, described ankylosing spondylitis and hypertrophic osteoarthropathy.
In our own lifetimes, the evolution has continued. When Salpêtrière fused in 1968 with historic La Pitié hospital, a large multidisciplinary university hospital with a new medical school was formed. By the next year, the remaining elderly residents had disappeared. The hospital currently has nearly 1900 beds, and a very strong rheumatology service.
And so we arrive at 1997, and Princess Diana’s final journey. It is ironic, and a bit poignant, that that glamorous and celebrated woman’s journey ended at La Salpêtrière, an institution built to shelter the outcast and rejected women of society. Another bit of history has thus been added to its fabled past.
Acknowledgment
I am exceedingly grateful to Prof. Marcel-Francis Kahn of Paris for calling my attention to Charcot’s substantial contributions to rheumatology.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}