

Abstract
Objective. To determine the association of knee bone size, cartilage volume, and body mass index (BMI) at baseline with knee cartilage loss over 2 years in younger or middle-aged adults.
Methods. A total of 324 subjects (mean age 45 yrs, range 26–61) were measured at baseline and about 2 years later. Knee cartilage volume and bone size were determined using T1-weighted fat-saturated magnetic resonance imaging.
Results. In multivariable analysis, baseline knee bone size was negatively associated with annual change in knee cartilage volume at medial and lateral tibial sites (ß = −0.62% to −0.47%/cm2, all p < 0.001). The associations disappeared at medial tibial site after adjustment for baseline cartilage volume and became of borderline statistical significance at lateral tibial site after adjustment for both baseline cartilage volume and osteophytes (ß = −0.29, p = 0.059). Baseline knee cartilage volume was consistently and negatively associated with annual change in knee cartilage volume at all 3 medial tibial, lateral tibial, and patellar sites (ß = −4.41% to −1.37%/ml, all p < 0.001). Baseline BMI was negatively associated with an annual change in knee cartilage volume, but only in subjects within the upper tertile of baseline cartilage volume, even after adjusting for cartilage defects (ß = −0.16% to −0.34%/kg/m2, all p < 0.05).
Conclusion. Our study suggests that both higher baseline tibial bone area and knee cartilage volume (most likely due to cartilage swelling) are associated with greater knee cartilage loss over 2 years. A higher BMI was associated with greater knee cartilage loss only in subjects with higher baseline cartilage volume.
Osteoarthritis (OA) is the most common form of arthritis and is characterized by gradual loss of articular cartilage and abnormalities of subchondral bone such as osteophytosis and subchondral sclerosis. It is widely accepted that subchondral bone plays a central role in the pathogenesis of OA, but it remains controversial whether the subchondral bone abnormalities precede the cartilage degeneration in the early stage of this disease1. We have reported that, cross-sectionally, tibial bone size was consistently and positively associated with the severity and prevalence of knee cartilage defects in men and women2, and longitudinally, baseline tibial bone area was positively associated with the worsening in knee cartilage defects over time3,4,5. This suggests knee bone size is causally related to knee cartilage defects. Cartilage defects can contribute to cartilage volume loss6,7 and theoretically, tibial bone area may be associated with loss of cartilage volume. Indeed, a recent study reported that bone area predicts loss of medial tibial cartilage volume in a group of older adults4; however, there are very few data in younger adult men and women8,9,10. There are numerous, more current, human studies suggesting that cartilage swelling (expressed as greater cartilage volume or thickness) occurs in early OA followed by cartilage degeneration11,12, and in subjects with established knee OA, initial cartilage volume was significantly associated with the loss of tibial cartilage volume8. There are no data to report the association between initial knee cartilage volume and knee cartilage loss in healthy younger subjects.
Further, body mass index (BMI) is an established risk factor for knee OA. Studies have reported consistent associations between overweight and onset or progression of radiographic knee OA13,14. BMI and obesity were associated with tibial bone size15 and prevalent15 and incident3 knee cartilage defects, but there is no clear evidence to suggest that BMI is directly associated with loss in tibial cartilage volume8,9,10. The aim of our longitudinal and magnetic resonance imaging (MRI)-based study was to determine the associations between baseline knee bone size, cartilage volume, BMI, and knee cartilage loss over time in a convenience sample of younger adult men and women.
Materials and Methods
Subjects
We carried out our study in southern Tasmania, and primarily in the capital city, Hobart, from June 2000 to December 2001. The followup study was conducted about 2 years later. Subjects were selected from 2 sources. Half the subjects were the adult children (offspring) of patients who had a knee replacement performed for primary knee OA at any Hobart hospital in 1996–2000. This diagnosis was confirmed by reference to the medical records of the orthopedic surgeon and the original radiograph where possible. The other half were age-matched and sex-matched controls selected at random from the State Electoral Roll, a comprehensive listing of the population. Subjects from either group were excluded on the basis of contraindication to MRI (including metal sutures, presence of shrapnel, iron filings in the eye, and claustrophobia), significant knee trauma and/or pain, having an occupation that puts them at risk of OA of the knee, rheumatoid arthritis, and other inflammatory arthritis. Subjects selected as controls were included as cases if they had a parent who had had a knee replacement for OA. No women were on hormone replacement therapy during the study period. Our study was approved by the Southern Tasmanian Health and Medical Human Research Ethics Committee and all subjects provided informed written consent.
Anthropometrics
Weight was measured to the nearest 0.1 kg (with shoes, socks, and bulky clothing removed) using a single pair of electronic scales (Seca Delta Model 707), which were calibrated using a known weight at the beginning of each clinic. Height was measured to the nearest 0.1 cm (with shoes and socks removed) using a stadiometer. BMI (kg/m2) was calculated.
Radiograph
A standing anteroposterior (AP) semiflexed view of the right knee was performed in all subjects at baseline and scored individually for osteophytes and joint space narrowing as described16. Radiographic OA was defined if any score of osteophytes or joint space narrowing measured ≥ 1.
Knee cartilage volume measurement
MRI scans of the right knees were performed at baseline and at the 2-year followup. Knees were imaged in the sagittal plane on a 1.5-T whole-body magnetic resonance unit (Picker, Cleveland, OH, USA) with use of a commercial transmit-receive extremity coil. The following image sequence was used: a T1-weighted fat saturation 3-D gradient recall acquisition in the steady state; flip angle 55°, repetition time 58 ms, echo time 12 ms, field of view 16 cm, 60 partitions, 512 × 512 matrix, acquisition time 11 min 56 s, 1 acquisition. Sagittal images were obtained at a partition thickness of 1.5 mm and in-plane resolution 0.31 × 0.31 (512 × 512 pixels). Knee cartilage volume was determined by means of image processing on an independent workstation using Osiris (University of Geneva) as described2,8,9,10,17. The volumes of individual cartilage plates (medial tibial, lateral tibial, and patella) were isolated from the total volume by manually drawing disarticulation contours around the cartilage boundaries on a section-by-section basis. These data were then resampled by means of bilinear and cubic interpolation (area of 312 and 312 μm and 1.5 mm thickness, continuous sections) for the final 3-D rendering. The volume of the particular cartilage plate was then determined by summing all the pertinent voxels within the resultant binary volume. Femoral cartilage volume was not assessed as we have published that 2 tibial sites and the patella site correlate strongly with this site18. Using this method we had high intraobserver and interobserver reproducibility. The coefficient of variation (CV) for cartilage volume measures was 2.1% for medial tibial, 2.2% for lateral tibial, and 2.6% for patella17.
Knee cartilage defect measurement
Knee cartilage defects were measured from the same MRI scans that were used for volume measurements. Normal cartilage was graded as 0 and abnormal intrachondral signals with a normal chondral surface were graded as 1. Mild surface irregularity or focal loss of < 50% of cartilage thickness and severe surface irregularities with focal loss of > 50% of cartilage thickness were graded as 2 and 3, respectively. Complete loss of articular cartilage with exposure of subchondral bone was graded 4. We also took into consideration the cartilage defects in the surface adjacent to subchondral bone, even though the cartilage surface was intact. A cartilage defect also had to be present in ≥ 2 consecutive slices. The cartilage defects were regraded 1 month later and the average scores of cartilage defects at medial tibiofemoral (0–8), lateral tibiofemoral (0–8), patellar (0–4), and whole compartments (0–20) were used in the study. Intraobserver reliability (expressed as intraclass correlation coefficient, ICC) was 0.89–0.94 and interobserver reliability was 0.85–0.932,3.
Knee bone size measurement
Knee tibial plateau bone area and patellar bone volume were determined by means of image processing in an independent workstation using the Osiris program as described17. The Analyse Software package developed by the Mayo Clinic was used to transform the images to the axial plane. Medial and lateral tibial plateau bone areas were determined by creating an isotropic volume from the 3 input images closest to the knee joint. This method does not take tibial curvature into account and is a composite measure of the subchondral plate and cancellous bone. The bone area of the medial and lateral tibial plateau was then directly measured from the reformatted axial images. Area of patellar bone was determined individually by manually drawing contours around the target patella boundaries on a slice-by-slice basis on sagittal views. The volume of the patella bone was then determined by summing all the pertinent voxels within the resultant binary volume. Total volume was calculated for the patellar bone because of its irregular shape, which made it difficult to identify a simpler, representative measure of patellar size. The CV for these measures in our hands are 2.2–2.6%17.
Data analysis
Rates of change in cartilage volume were calculated as percentage change per year = 100 × (followup cartilage volume – baseline cartilage volume)/baseline cartilage volume/time between 2 scans in years.
Linear regression analysis was used to examine the associations between annual change in cartilage loss, baseline knee bone size, baseline knee cartilage volume, and BMI before and after adjustment for age, sex, BMI, off-spring-control status, and/or radiographic OA. Tertiles of baseline knee bone size and cartilage volume were calculated in men and women, respectively, and the associations between annual change in cartilage loss and tertiles of baseline knee bone size or cartilage volume were also examined. Because we found significant interactions between baseline cartilage volume and BMI in the regression of annual changes in cartilage volume, the associations between BMI and annual changes in cartilage volume were examined separately in subjects with lower (first), middle (second), and upper (third) tertile of baseline cartilage volume. ANOVA test was used to compare difference between subjects with lower, middle, and upper tertile of baseline cartilage volume.
To test whether the results were subject to influences of regression toward mean, we redid the analyses using the methods provided by Hopkins19. We subtracted the baseline mean cartilage volume from each subject’s baseline cartilage volume, then multiplied this difference by (1 − r), where r was the retest correlation coefficient. The result was added to the change in cartilage volume for the subject, and this corrected change score was free of the artefact caused by regression toward mean.
A p value < 0.05 (2-tailed) or a 95% CI not including the null point was regarded as statistically significant. All statistical analyses were performed on SPSS version 12.0 for Windows (SPSS, Chicago, IL, USA).
RESULTS
A total of 324 subjects (135 men, 189 women) completed the study (87% of those originally studied). This was a younger sample, with an average age of 45 years at baseline (range 26–61). The average time between visits was 2.3 (range 1.8–2.6) years. Characteristics of the subjects are presented in Table 1. There were no significant differences among subjects with lower, middle, and higher tertile of baseline cartilage volume in terms of sex, age, weight, BMI, and osteophytes (all p > 0.05); however, those in the highest tertile of baseline cartilage volume were taller, had lesser radiographic OA, lesser medial joint space narrowing, and fewer cartilage defects, and had greater bone size compared to subjects in the lower baseline cartilage volume (all p < 0.05).
Characteristics of participants at baseline.
Over 2.3 years, there is no significant difference in BMI change among groups divided by tertiles of baseline cartilage volume; however, a significant loss of cartilage volume was noted in the middle and higher tertiles of baseline cartilage volume (Table 2).
Change in body mass index (BMI) and cartilage volume after 2 years. All data except BMI and p values are percentage change per year (SD).
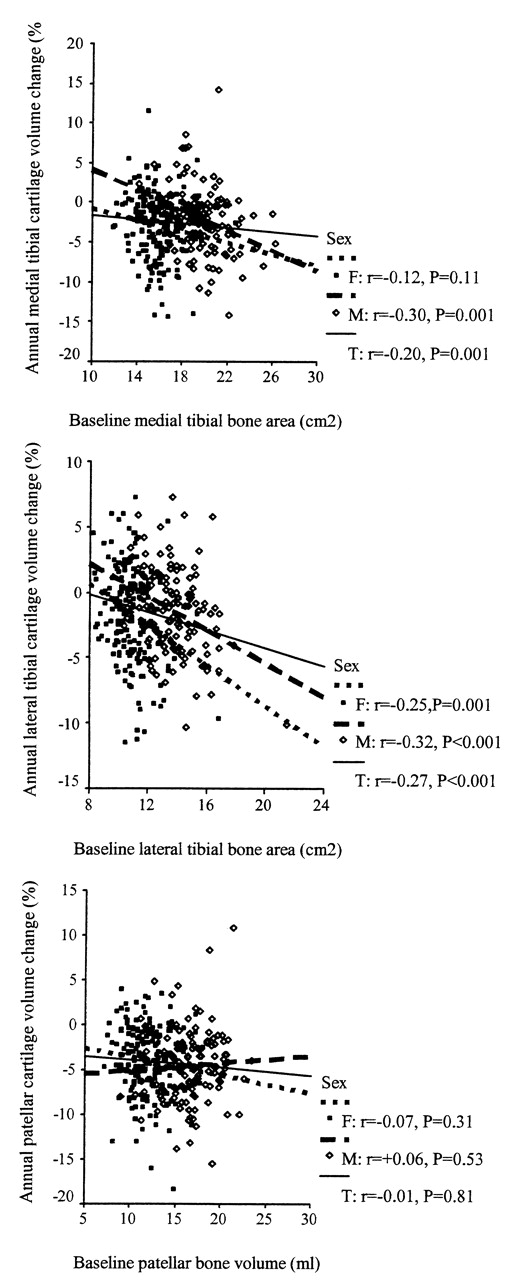
In multivariable analyses including adjustment for cartilage defects, baseline tibial bone size was negatively associated with change in tibial cartilage volume (Figure 1, Table 3). After further adjustment for baseline tibial cartilage volume, the statistically significant negative associations between baseline tibial bone area and change in cartilage volume disappeared at the medial tibial site, decreased in magnitude at the lateral tibial site, and even became positive at the patellar site (Table 3). Baseline knee cartilage volume was negatively associated with change in knee cartilage volume at all 3 sites in the whole sample (Table 3), as well as in men and women separately (Figure 2). After adjustment for cartilage defects and baseline knee bone size (Table 3), these associations remained at all sites.

Correlation between baseline knee bone size and change in knee cartilage volume. Baseline knee bone size was negatively associated with change in medial and lateral tibial cartilage volume. All correlations (r) were those after adjustment for age, body mass index, offspring-control status, and/or sex.

Correlation between baseline knee cartilage volume and change in knee cartilage volume. Baseline knee cartilage volume was negatively associated with change in knee cartilage volume at medial tibial, lateral tibial and patellar sites. All correlations (r) were those after adjustment for age, body mass index, offspring-control status, and/or sex.
Associations of baseline knee bone size and cartilage volume with change in knee cartilage volume per year: multivariate analysis. Data are ß 95% CI (%). Bold type denotes statistically significant result.
In multivariable analysis, BMI was significantly associated with change in patellar cartilage volume, but not with changes in tibial cartilage volume in the whole sample; however, BMI was significantly associated with changes in tibial and patellar cartilage volume in subjects within the upper tertile of baseline cartilage volume after adjustment for factors including baseline cartilage defect score (Table 4). There were no significant associations between BMI and change in cartilage volume in subjects within lower and middle tertile of baseline cartilage volume (Table 4). Change in BMI was also significantly associated with change in medial tibial cartilage volume in subjects within the upper tertile of baseline cartilage volume (ß = −0.49 per kg/cm2, p = 0.038), but not in subjects within the lower and middle tertile of baseline cartilage volume (ß = +0.13 to +0.20 per kg/cm2, p > 0.3). No significant associations between change in BMI and change in lateral tibial or patellar cartilage volume were found (data not shown).
Associations of body mass index with change in knee cartilage volume per year. All data are ß 95% CI (%). Bold type denotes statistically significant result.
The results remained largely unchanged after adjustment for radiographic OA (data not shown); however, the association between baseline bone area and cartilage loss at the lateral tibial site became nonsignificant (ß = −0.29/cm2, p = 0.059) after further adjustment for lateral tibiofemoral osteophytes. Lateral tibiofemoral osteophytes were associated with change in lateral tibial cartilage volume before (ß = −2.42, p = 0.003) and after adjustment for age, sex, BMI, offspring-control status, baseline lateral tibial cartilage volume, and bone area (ß = −1.86/grade, p = 0.026). The results remained unchanged if regression toward mean was accounted for (data not shown).
Analysis was performed separately in a younger (≤ 45 years) and an older (> 45 years) group to see if the associations varied between age groups. The results remain largely unchanged in both age groups (data not shown). There were no significant interactions (all p > 0.10) between age (≤ 45 vs > 45) and baseline measures on loss of cartilage volume, so all participants are combined for analyses.
DISCUSSION
Our longitudinal study documents the associations between annual change in knee cartilage volume and baseline bone size, cartilage volume, and BMI in a large convenience sample of subjects. We found that baseline tibial bone area and cartilage volume were positively associated with loss in knee cartilage volume over 2 years. Further, higher baseline BMI was associated with higher loss of knee cartilage volume in subjects with greater baseline cartilage volume.
Changes in subchondral bone, including remodeling of subchondral trabeculae20,21, stiffening of the subchondral bone22, thickening of the subchondral plate21,23, and a decrease of the ability to absorb energy24, are well described in established OA25. These changes affect the mechanical properties of the subchondral bone and have been proposed to play a role in the initiation and progression of degeneration of the overlying articular cartilage1,4,26. Changes in subchondral bone size may reflect the change in its architecture. We reported in cross-sectional studies that tibial bone size increased with increasing age27 and BMI15 and was positively associated with osteophytes16,18, joint space narrowing18, and knee cartilage defect score2. Our longitudinal study showed that baseline tibial bone area was associated with an increase in knee cartilage defects over 2 years3, suggesting that tibial bone expansion can attenuate the tibial cartilage28.
To our knowledge ours is the first study to report that baseline tibial bone size was associated with loss of tibial cartilage volume over 2 years in both younger or middle-aged men and women. This finding is consistent with the findings in older adults4. This was independent of age, BMI, and offspring-control status; however, this association became nonsignificant or decreased in magnitude after adjustment of baseline cartilage volume. The reasons for this are unclear, but given that baseline tibial bone area was strongly associated with baseline cartilage volume in this sample, we can conjecture that tibial bone expansion could induce cartilage swelling (increased cartilage volume) at an early stage, which is then followed by tibial cartilage loss over time. We also found that the association between baseline lateral tibial bone area and lateral tibial cartilage loss decreased in magnitude after adjustment for baseline lateral tibiofemoral osteophytes, and osteophytes were associated with tibial bone area16 and lateral tibial cartilage loss, supporting the fact that pathological changes in subchondral bone may initiate tibial cartilage loss.
Although knee cartilage volume is greater in men than women29 and is negatively associated with joint space narrowing16 in this sample, it is not significantly associated with risk factors of OA including age27 and BMI15. Further, there was a nonsignificant trend to higher cartilage volume at baseline in the offspring of patients who had a total knee replacement for severe primary knee OA than in age-matched and sex-matched controls, indicating that cartilage volume may increase in some subjects in the early stages of OA because of increased water content30. Our study showed that higher baseline cartilage volume at tibial and patellar sites was strongly associated with greater knee cartilage loss at tibial and patellar sites in both men and women. This loss was independent of age, BMI, offspring-control status, bone size, and radiographic OA. This could be due to a floor effect resulting from lower baseline cartilage volume or a ceiling effect resulting from higher baseline cartilage volume; however, the associations remained the same in each tertile (data not shown). The floor effect may exist when little or no cartilage remains, but it is unlikely to be present in healthy young subjects. It may also be influenced by regression toward mean; however, the results also remained unchanged if regression toward mean was accounted for by a statistical method.
Current MRI technique to measure cartilage volume does not allow us to differentiate if the increase in cartilage volume is due to gain in normal cartilage matrix or cartilage swelling. New MRI techniques such as T2 mapping may be capable of detecting cartilage swelling, because T2 relaxation reflects the ability of free water protons to move and to exchange energy inside the cartilage matrix; damage to proteoglycan or collagen and increase in water content might increase T2 relaxation time31; however, that possibility needs to be validated by further studies. Our results were consistent with the findings in subjects with established knee OA8, and the finding that higher baseline cartilage volume was associated with greater knee cartilage defect development over 2 years3, suggesting that knee cartilage swelling at early stage is followed by more knee cartilage loss over time.
We reported in a cross-sectional study in 200515 that BMI was associated with knee bone size and prevalent knee cartilage defects, but BMI was not associated with knee cartilage volume. This may be due to the coexistence of cartilage hypertrophy and cartilage thinning in the early stage of arthritis. Longitudinal studies show that BMI is associated with an increase in knee cartilage defects in healthy subjects3 and patellar cartilage loss in subjects with OA32. However, BMI was not associated with tibial cartilage loss in osteoarthritic8 and healthy9,10 subjects, which may reflect study design issues, small sample sizes, and/or the inability of cartilage volume assessment to differentiate swollen from normal cartilage. We found that in the whole sample, BMI was associated with patellar but not tibial cartilage loss over 2 years; however, BMI was significantly associated with knee cartilage loss at all 3 sites in subjects within the higher tertile of baseline cartilage volume, and this was independent of cartilage defects. This suggests that higher BMI predicts greater knee cartilage loss over time in subjects with increased baseline cartilage volume, which is most likely due to cartilage swelling in early disease. Consistently, change in BMI was significantly associated with change in medial tibial cartilage volume in subjects with greater baseline cartilage volume over 2 years, suggesting that weight loss can reduce cartilage loss in subjects with early knee disease.
The loss to followup in this study was small, suggesting that nonparticipation was not a source of major concern, but that study has a number of potential limitations. It was primarily designed to look at genetic mechanisms of knee OA and used a matched design of siblings and controls. The matching was broken for our current study but adjustment for family history did not substantially alter the main results. The sample is a convenience sample that limits the relevance of prevalence estimates; however, as an analytical study, Miettinen33 states that for associations to be generalizable to other populations, 3 key criteria need to be met regarding selection, sample size, and adequate distribution of study factors. Our study meets all of these. In addition, measurement error may influence results, but our measurements of knee cartilage volume, bone size, and radiographic OA measurement were highly reproducible16,17, suggesting that this is unlikely. Lastly, we included participants within a wide age range, a factor that could affect the data. However, the associations remained largely unchanged when the analyses were performed in 2 age groups, and there were no significant interactions between age and baseline measures on cartilage loss.
Our study suggests that both higher baseline tibial bone area and knee cartilage volume (most likely due to cartilage swelling) are associated with greater knee cartilage loss over 2 years. A higher BMI was associated with greater knee cartilage loss only in subjects with higher baseline cartilage volume.
Acknowledgment
A special thanks to the subjects and orthopedic surgeons who made this study possible. The role of Catrina Boon in coordinating the study is gratefully acknowledged. We thank Martin Rush, who performed the MRI scans, and Kevin Morris for technical support.
Footnotes
-
Support from the National Health and Medical Research Council of Australia, Masonic Centenary Medical Research Foundation.
- Accepted for publication April 8, 2011.








{kind=link}
{kind=link}