

Abstract
The 2008 World Health Report emphasizes the need for patient-centered primary care service delivery models in which patients are equal partners in the planning and management of their health. It is argued that this involvement will lead to improved management of disease, improved health outcomes and patient satisfaction, better informed decision-making, increased compliance with healthcare decisions, and better resource utilization. This article investigates the domains captured by the Effective Consumer Scale (EC-17) in relation to vulnerable population groups that experience health inequity. Particular focus is paid to the domain of health literacy as an area fundamental to patients’ involvement in managing their condition and negotiating the healthcare system. In examining the possible influence of Outcome Measures in Rheumatology Clinical Trials (OMERACT) on health equity, we used the recent translation and validation of the EC-17 scale into Spanish and tested Argentina as an example. Future plans to use the EC-17 with vulnerable groups include formal collaboration and needs assessment with the community to tailor an intervention to meet its needs in a culturally relevant manner. Some systematic reviews have questioned whether interventions to improve effective consumer skills are appropriate in vulnerable populations. We propose that these populations may have the most to gain from such interventions since they might be expected to have relatively lower skills and health literacy than other groups.
There is growing support for an increased role for patients in improving the quality of healthcare through their participation and consultation1. It is hoped that through patient engagement, interventions will be safe and more appropriate, and patients more responsive2. The same trend can be seen in health research. Outcome Measures in Rheumatology Clinical Trials (OMERACT) is a leader in involving patients in rheumatology research and has an active patient group. OMERACT executive members and working groups value the meaningful input given by patients and invest resources to ensure that patients are able to attend OMERACT meetings. Patients’ ability to contribute to discussions on outcomes is supported by experienced group members and designated researchers at these OMERACT meetings. OMERACT and other academic and research groups recognize the potential of engaged patients to contribute to defining useful health outcomes. Similarly, other national and international agencies increasingly encourage patients to play a more active role in their own healthcare to improve the quality and efficiency of service delivery. For instance, the National Health Service in the United Kingdom has a center devoted to patient engagement and encouraging patient involvement3. When patients are involved, services can be tailored to meet the needs of local patients with longterm conditions. The organization contends that patients are likely to be more satisfied and happier with services if they have played a part in their design. Similarly, if patients can help set health research priorities (including outcomes), there is a greater chance that the research will answer patient questions about a particular condition, potentially reducing health inequalities.
The Effective Consumer Scale (EC-17) was developed by members of our team to measure patients’ ability to participate in their health and manage their interaction with the healthcare system4,5. The EC-17 assesses patients’ perception of their skills and behaviors that are important for effectively managing, participating in, or leading their healthcare (Figure 1). Interventions linked to empowering patients in their own health could increase their adherence to suggested treatments or preventive actions, thus improving patient safety6. Shared decision-making (a decision-making process jointly shared by patients and their healthcare providers7) and self-management (the knowledge, tools, and skills patients possess to manage their disease or diseases) techniques have emerged as possible interventions. However, shared decision-making and self-management have been criticized as being narrowly focused as they do not consider broader determinants of health and rely on a weak evidence base8. Further, including patients in research activities or guideline development represents a major challenge as the patients must be adequately informed and allowed to participate fully, rather than being token representatives9.
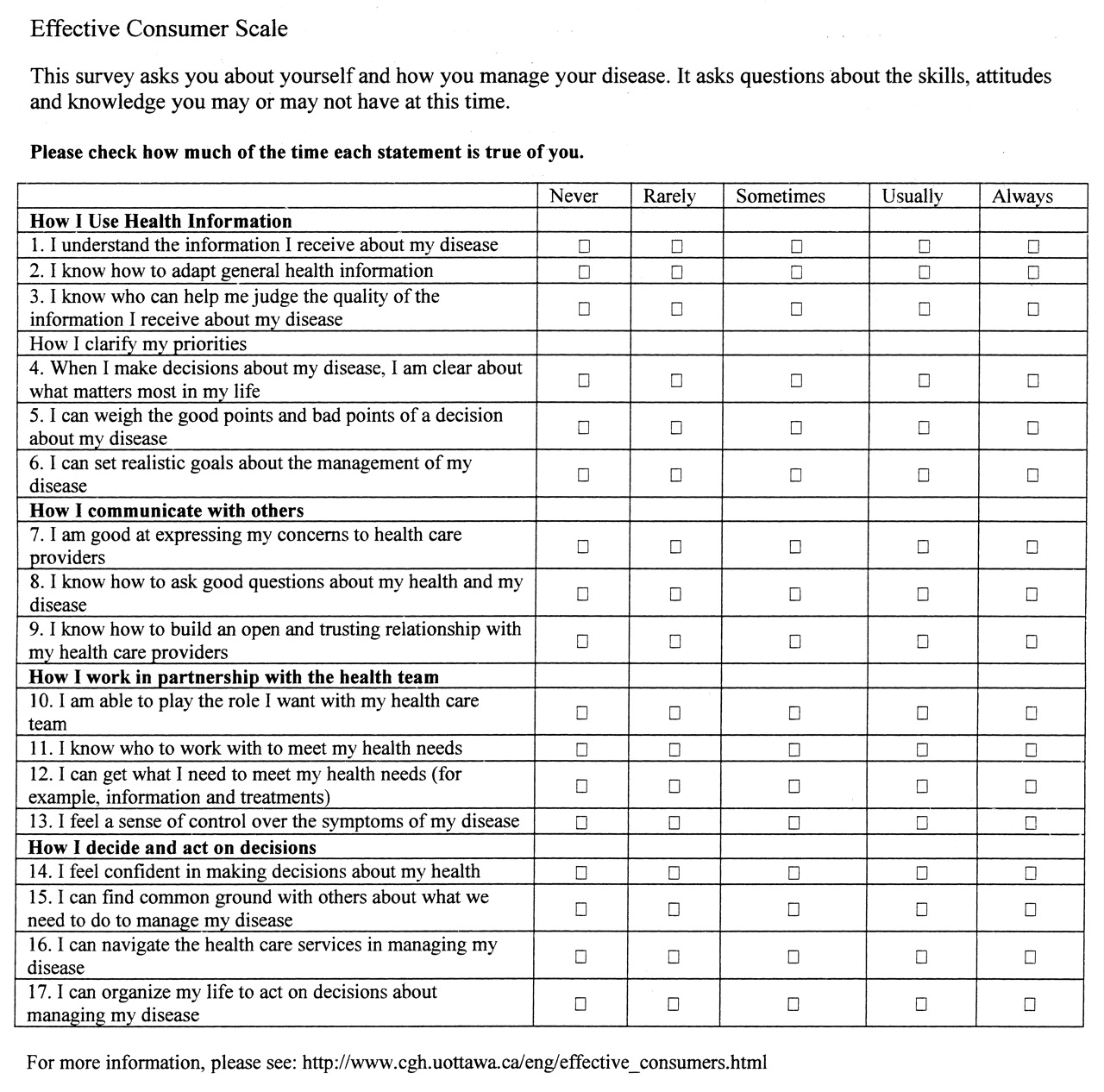
Effective consumer scale EC-17. From Kristjansson, et al. J Rheumatol 2007;34:1392–400.
Although there is extensive literature supporting stronger involvement from patients in their health, systematic reviews of interventions to improve health literacy at a community level often are focused on improving participants’ knowledge instead of their skills10. Health literacy is sometimes misconstrued as the ability to read and comprehend medical information. Health literacy is actually a much broader concept: it can be defined as “the ability to make sound health decisions in the context of everyday life.” This includes reading and comprehending medical information; the application of health prevention and self-care behaviors; verbal communication with health professionals; analytical and decision-making skills; and health advocacy and activism10. Some systematic reviews question whether interventions to improve skills are effective in low-literacy, disadvantaged populations. However, low-literacy populations may have the most to gain from skills interventions since these groups might have lower skills and health literacy than others. Based on experiences with populations in Argentina and other countries, health literacy appears to be a key domain to influence effective consumer skills among disadvantaged and vulnerable groups.
When end-users are involved in research, it strengthens the research process, often leads to greater utilization of research findings, and improves public administration planning and management9. Although there is extensive literature supporting stronger involvement from patients in their health, the systematic reviews of interventions to improve health literacy at a community level are often focused on improving patient knowledge, not patient skills4. Education studies have shown that interventions aimed at improving skills are more effective and their benefits remain a longer time than those focused on improving only knowledge11.
Health Equity
Patients’ ability to participate fully in the management of their own condition, to negotiate the healthcare system, and to play a role in the broader realm of health research or advocacy also depends on the extent to which they face health inequity. Health inequity refers to those differences in health that are unnecessary, avoidable, unfair, and unjust12,13,14. Disadvantaged populations are at the highest risk for suffering these unfair and unjust avoidable differences, which can be seen across social groups defined by the mnemonic PROGRESS-Plus. PROGRESS is an acronym for Place of residence, Religion, Occupation, Gender, Race/ethnicity, Education, Socioeconomic status, and Social networks and capital, while Plus refers to additional factors such as age, sexual orientation, and disabilities15,16. Table 1 shows the interplay between these social factors and the 5 domains of the EC-17: (1) use of health information; (2) clarifying personal priorities; (3) communicating with others; (4) negotiating roles and taking control; and (5) deciding and taking action5.
Health inequity and the 5 domains of the Effective Consumer Scale 17 (EC-17).
Background on the EC-17 Scale
To evaluate the readiness and ability of people to engage in self-care, it is important to develop not just clinical outcome measures, but quantifiable assessments of how well individuals with arthritic diseases manage their health and healthcare. The OMERACT initiative has given priority to establishing valid and reliable outcome measures that are important to patients. People with arthritis are invited to participate in OMERACT meetings and in setting research priorities. The measurement of how patients effectively engage in the management of their chronic disease was identified as an OMERACT priority area by 2005. The unidimensional EC-17 was developed to assess patients’ perception of their skills and behaviors that are important for effectively managing, participating in, or leading their healthcare4. Following a literature review, semistructured interviews were conducted with people with arthritic diseases and their networks (e.g., family, healthcare providers, etc.) to identify a set of skills and behaviors that people need to manage their health effectively. These interviews were supplemented by consultations with key stakeholders, including patient and professional organizations and research experts. A pilot project assessed the psychometric properties of the scale, and classical and item response theory analyses reduced the scale from 48 to 17 items5.
How OMERACT Activities Can Consider Health Equity: The Translation and Validation of the Spanish Version of the EC-17
Discussions at the OMERACT 9 Patient Perspective Workshop (Kananaskis, Canada, 2008) indicated that there was significant interest in the development of domain-specific tools (especially in health literacy) to assist people to become more effective consumers. One of the conclusions of that meeting was that the scale may be relevant for individuals with other chronic diseases such as asthma, cardiac disease, and diabetes. With the aim of applying the EC-17 more widely, the scale was recently translated into Spanish. We followed recommended steps for assessing conceptual relevance in the Spanish culture, then performed forward- and back-translation using bilingual editors17. Two bilingual editors and one bilingual patient assessed the EC-17 scale to appraise whether the concept of “effective consumerism” existed and could be measured in Argentina. This assessment considered cultural norms and expectations regarding patients’ participation in their own healthcare. Translation was performed by 2 bilingual editors who were familiar with the content area of patient engagement. One editor translated the EC-17 to Spanish, with the aim of ensuring conceptual equivalence rather than direct linguistic equivalence. The back-translated scale was then discussed with the developers of the scale to ensure conceptual equivalence. The Argentine investigators interviewed 10 patients about their understanding of the items in the back-translated scale. This feedback resulted in subtle changes to the wording of items to improve the relevance to an Argentine context. For example, one English item asked whether patients could judge the quality of information. However, Argentine patients and physicians found the word “quality” too strong and inappropriate for their setting, and suggested changing the wording to assessing whether the information was “good or bad.” Such changes were discussed and approved by the developers of the English version of the scale.
Results of a recent pilot study18 provide initial evidence towards the reliability and validity of the Argentine version of the EC-17. Reliability was confirmed by findings of high levels of Cronbach’s alpha and item correlation. Construct validity was also confirmed by factor analysis. This version has good feasibility in public and private settings in Buenos Aires.
The translated questionnaire was given to Argentine patients with chronic disease in waiting rooms in public and private hospitals before they saw their clinician. We collected 229 completed surveys, of which 155 had fully completed data to be analyzed. Although this was a convenience sample, the sample’s sociodemographic characteristics were considered to be representative of what is usually seen in ambulatory care centers regarding age and sex distribution, level of education, and frequency of self-reported chronic diseases.
The pilot evaluation and self-reported comments from the survey testing showed that the EC-17 was relatively easy to complete. The items were well understood apart from question 15 of the EC-17 (“I can find common ground with others about what we need to do to manage my disease”), which did not perform well on reliability analysis.
a. Score distribution
Average summary and scales scores, standard deviations, ranges, and ceiling and floor effects were calculated. Respondents used the complete range of response options. Ceiling and floor effects were negligible for all items (below 15%).
b. Reliability
We estimated several indicators to evaluate reliability such as Cronbach’s alpha (0.93) and inter-item correlation. All results exceeded the standard threshold of 0.7 for Cronbach’s alpha except for Q15 when we explored the item-rest correlation.
c. Validity
Construct validity was estimated by factor analysis in which we showed that the instrument is unidimensional. This corresponds with what is already reported by the creators of the original version of the EC-17.
Future Research
The Spanish translation and subsequent validation forms the basis for developing interventions that can be measured by the EC-17 in disadvantaged populations. The Spanish version of the EC-17 will be used in future work in rural settings and among vulnerable populations in urban settings. Our goal is to improve the skills of vulnerable populations to deal with the health system, in order to participate and fully engage in primary prevention activities by designing interventions to meet the challenges of being an effective consumer in different communities. In this way, we hope to improve the health status and safety of the participating communities, including Aboriginal communities. This project is framed on the equity-effectiveness loop and knowledge translation framework, which stress the importance of assessing the distribution of effects across socioeconomic gradients; these effects are considered at all steps of research development, from needs assessment and community effectiveness through to knowledge translation and monitoring19.
A participatory action model is the preferred approach to engage members of vulnerable populations. In future research, we will address the following objectives: (1) Using the EC-17 in a needs assessment exercise, we will identify the set of core skills that would empower vulnerable populations to participate in their healthcare. (2) Based on a needs assessment, we will conduct a pilot test of a tailored intervention to improve the relevant skills. (3) We will evaluate the impact of interventions on health status and safety by using appropriate methods in diverse settings.
The interventions will be designed through consultation with members of each community to assess barriers to effectively managing their healthcare. The intervention will be implemented in community or clinic-based group settings. We will base the intervention on a needs assessment, using the EC-17 to address deficits found in any of the EC-17’s five domains: (1) use of health information; (2) clarifying personal priorities; (3) communicating with others; (4) negotiating roles and taking control; and (5) deciding and taking action. Previous research with the EC-17 has shown that health literacy (i.e., the use of health information) is an area of deficit among people with arthritis taking part in a self-management program20. Thus, an intervention that considers health literacy will be developed in collaboration with the community.
It is hoped that with careful collaboration with local communities, we can continue to use the EC-17 to address the needs of disadvantaged groups, as they have much to gain from improved effective consumer skills. Based on experiences with populations in Argentina and other countries, health literacy appears to be a key domain to influence effective consumer skills among disadvantaged and vulnerable groups.
Footnotes
-
P. Tugwell is supported in part by the Canadian Institutes of Health Research. R.H. Osborne is supported in part by an Australian National Health and Medical Research Council Population Health Career Development Award.








{kind=link}