

Abstract
Objective. To study possible associations between extended mannose-binding lectin (MBL) expression genotypes and clinical manifestations and infections in children with systemic lupus erythematosus (SLE).
Methods. Clinical and laboratory variables for a cohort of 125 patients with pediatric-onset SLE were obtained by clinical examinations and chart reviews. Controls were 137 age-matched and sex-matched healthy children and adolescents. MBL gene polymorphisms were genotyped by polymerase chain reaction. Serum MBL concentrations were measured by ELISA.
Results. The frequencies of extended MBL expression genotypes did not differ between patients and controls. There were 82 patients with SLE who had high MBL expression genotypes and 43 who had medium and low MBL expression genotypes. Patients with the high MBL expression genotype had renal disorders more frequently than patients in the group with medium and low MBL expression genotypes [54/82 (65.9%) vs 18/43 (41.9%), respectively; p = 0.013] and fewer serious bacterial infections [22/82 (26.8%) vs 20/43 (46.5%); p = 0.030]. Using logistic regression for patients with SLE, a high MBL expression genotype was independently associated with renal disorders (OR 2.49, 95% CI 1.15–5.39, p = 0.021) and had a protective effect against serious bacterial infections (OR 0.29, 95% CI 0.12–0.71, p = 0.007). MBL levels decreased significantly when patients with active SLE reached an inactive stage (1.56 ± 0.55 μg/ml vs 1.08 ± 0.65 μg/ml; p = 0.001), but these levels were still higher than those in controls.
Conclusion. Our findings suggest that a high MBL expression genotype is a risk factor for renal disorder, while it has a protective effect against infections. Serum MBL levels reflect SLE activity.
Mannose-binding lectin (MBL), a component of the complement system, plays an important role in innate host defense. Serum MBL can directly opsonize microorganisms and enhance their uptake by phagocytic cells by activation of the lectin pathway of the complement system1. In addition, it has been suggested that MBL modulates inflammation and autoimmune diseases2,3. Six single-nucleotide polymorphisms (SNP) in the promoter and structural region of the human MBL gene on chromosome 10q are known to influence plasma levels of MBL.
Individuals who are heterozygous or homozygous for SNP in codons 52 (allele D, rs5030737), 54 (allele B, rs1800450), or 57 (allele C, rs1800451) in exon 1 of the MBL gene have structural changes that lead to reduced or deficient plasma levels of MBL2,4. The wild-type allele is designated A, while the common designation for variant alleles is O. In addition, MBL concentrations fluctuate because of the presence or absence of 3 SNP in the promoter region of the MBL gene (position −550: alleles H/L, rs11003125; position −221: alleles X/Y, rs7096206; and position +4: alleles P/Q, rs7095891). Only the X/Y variant has a pronounced influence on serum MBL levels5,6; the X allele is associated with decreased plasma MBL levels and the Y variant with high plasma MBL levels. Thus, individuals can be classified into high (YA/YA and YA/XA), medium (XA/XA and YA/O), and low (XA/O and O/O) MBL expression genotype groups.
The ability of MBL to bind to apoptotic cell debris by its lectin domain and its involvement in the phagocytosis of apoptotic cells by macrophages suggests an association between MBL and the occurrence of systemic lupus erythematosus (SLE)2. Previous studies of different ethnic populations indicated that several SNP in the promoter or structural region of the MBL gene are candidates for SLE, although this remains controversial because of inconsistent genetic associations7,8. Aside from autoimmune diseases, MBL deficiency has been associated with an increased susceptibility to and the severity of infections in children, adults, and those with immunodeficiencies3,4. Patients with SLE are inherently immunocompromised, and immunosuppressants that are used for treating major organ involvement further predispose these patients to infections9,10,11,12,13,14,15. MBL gene polymorphisms are associated with higher risks of infection in adult patients with SLE16,17. However, a possible predisposition to infection due to MBL genotypes in children with SLE has not been explored. In addition, possible relationships between serum MBL levels and SLE disease activity have not been well studied.
Our previous study showed that SNP in exon 1 of the MBL gene were not associated with susceptibility to SLE for children18. The purpose of our longitudinal study was to further investigate the associations of extended MBL expression genotype groups with susceptibility to pediatric-onset SLE; and to determine whether MBL expression genotypes were associated with the occurrence of major organ involvement and a predisposition to infections in a cohort of Chinese children over a period of 7 years. We also prospectively investigated a possible association between serum MBL levels and SLE disease activity.
MATERIALS AND METHODS
Study subjects
From June 2002 to May 2009, patients with SLE who met the American College of Rheumatology criteria for the diagnosis of SLE19,20 were enrolled from a well documented longitudinal cohort in a tertiary teaching medical center18,21. Patients who were younger than 18 years at the time of diagnosis of SLE disease were invited to participate in our study. During the study period, these patients with pediatric-onset SLE were regularly monitored for clinical manifestations, laboratory measures of disease activity, and current treatments.
Hematologic disorders, including hemolytic anemia, lymphopenia, leukopenia, and thrombocytopenia, were defined according to the American College of Rheumatology (ACR) criteria for SLE19,20 and were recorded as positive only if it was verified that cytopenia could be attributed to SLE rather than to the medications that the patients were taking or to other causes. Renal disease was diagnosed based on biopsy-proven lupus nephritis [World Health Organization (WHO) class II–VI] or according to the renal involvement criteria of the ACR19,20. Neuropsychiatric abnormalities were diagnosed based on clinical presentations that met the criteria of the ACR and central nervous system image studies19,20.
Laboratory tests routinely performed at the followup visits were a complete blood cell count, antinuclear antibody (by indirect immunofluorescence assay), anti-dsDNA antibody (by ELISA; normal range < 40 IU/ml), complement C3 (by nephelometry; normal range 90–180 mg/dl), complement C4 (by nephelometry; normal range 10–40 mg/dl), C-reactive protein (normal range < 5 mg/l), renal and liver function, and urinalysis (by reflective photometry and microscopic examination). Disease activity was determined regularly during the study period using the SLE Disease Activity Index (SLEDAI)22. The active stage of SLE was defined as SLE onset and SLEDAI > 5, the inactive stage was SLEDAI ≤ 5, and very high SLE activity was SLEDAI ≥ 2023,24,25. Information was obtained by chart reviews on the use of steroids (current dosage expressed in mg/kg/day) and immunosuppressants, including azathioprine, cyclophosphamide, hydroxychloroquine, cyclosporine, methotrexate, and mycophenolate mofetil.
Major infections, including serious bacterial infections (SBI) or herpes zoster infections that warranted hospitalization for parenteral antibiotics or antiviral agent treatment, were recorded during the study period. SBI included urinary tract infections (UTI), pneumonia, osteomyelitis, septic arthritis, bacterial meningitis, cellulitis, and microbiologically confirmed bacteremia. The diagnoses of infections were confirmed by clinical, microbiological, and imaging criteria.
Age-matched and sex-matched healthy children and adolescents without autoimmune diseases or atopic histories during the study period were enrolled as controls for genotyping. The control subjects were from a group that came to the hospital for vaccinations and healthy volunteers who were students in the Nursing Department of the Chang Gung Institute of Technology. MBL gene haplotype regions (including promoter and exon 1 variants) were analyzed for all patients and control subjects.
In addition, patients with SLE for whom the interval between initial SLE presentations and definite SLE diagnosis was within 1 month and who had an initial SLEDAI > 5 points were recruited for measurements of serum MBL concentrations. Patients with concomitant infections or other systemic diseases during the followup period were excluded. In order to investigate possible relationships between MBL changes and SLE disease activity, serum MBL concentrations were obtained at 2 timepoints: active and inactive stages for each patient23,24,25. Age-matched and sex-matched healthy children were also enrolled for MBL measurements; blood samples in the control group were obtained when they were recruited into the study. Informed consent was obtained from the parents or guardians of each subject before enrollment in the study. The hospital ethics committee approved the study.
MBL genotyping
Genomic DNA was extracted from peripheral blood samples with an Easy Pure Genomic DNA Purification Kit (Bioman Scientific Co., Taipei, Taiwan). A polymerase chain reaction (PCR)-based assay was used to genotype cases and controls for MBL gene polymorphisms, as described18. For amplification of promoter −550, primers 5’-CCA GGG CCA ACG TAG TAA GA-3’ and 5’-GAT GAG CAG TGG GGA TCC TA-3’ were used (PCR product 469 bp). For amplification of promoter −221, and B, C, and D alleles, primers 5’-CAG ACA CCT GGG TTT CCA CT-3’ and 5’-AGA ACA GCC CAA CAC GTA CC-3’ were used (PCR product 587 bp). Sequencing of the PCR products used a Big Dye Terminator kit (Applied Biosystems, Foster City, CA, USA) and an ABI Prism 3100 DNA Sequencer (Applied Biosystems). Genotyping was performed independently of clinical data collection and serum MBL measurements. Patients were classified into 3 MBL genotype groups: high, medium, and low MBL expressions.
Serum MBL measurements
Blood samples were frozen in aliquots and stored at −80°C prior to analysis. A commercial ELISA was used to measure serum MBL (Hycult Biotechnology, Uden, The Netherlands) according to the manufacturer’s instructions. All samples and standards were measured in duplicate and concentrations were determined from a standard curve using mean absorbance values. Serum MBL concentrations were expressed as μg/ml.
Statistical analysis
The genotype distributions for the MBL gene polymorphisms for our study population were in Hardy-Weinberg equilibrium. Categorical measures were compared using a chi-squared test or Fisher’s exact test, as appropriate. OR and 95% CI were determined by logistic regression and used as measures of associations between MBL expression genotypes and clinical presentations. For continuous variables, comparisons among > 2 groups used ANOVA or a Kruskal-Wallis test, and comparisons between 2 groups were done by a Mann-Whitney U test or paired t-test. Pearson’s correlation coefficient was used to evaluate associations between variables. Statistical analysis used SPSS statistical package version 10.0 for Windows (SPSS, Chicago, IL, USA). A p value < 0.05 was considered statistically significant.
RESULTS
MBL genotypes in patients with SLE and controls
A total of 125 unrelated patients with pediatric-onset SLE (110 girls and 15 boys) and 137 control subjects (118 girls and 19 boys) were included in this longitudinal analysis for evaluating MBL genotypes. The mean age (± SD) at SLE diagnosis was 12.56 ± 2.70 years and the followup duration was 6.95 ± 3.35 years. Exon 1 codon 52 and codon 57 variants were not detected in any of the study subjects. The frequencies of codon 54, promoter −550, −221 variants, and allele B among patients with SLE did not differ significantly from those of the controls (data not shown).
As shown in Table 1, the distributions of the extended MBL expression genotypes among the 125 patients with SLE were as follows: 51 (40.8%) YA/YA haplotype, 31 (24.8%) YA/XA haplotype, 8 (6.4%) XA/XA haplotype, 28 (22.4%) YA/O haplotype, 6 (4.8%) XA/O haplotype, and 1 (0.8%) O/O haplotype. These MBL expression genotype distributions were not significantly different between the SLE and control groups (p = 0.236).
Frequencies of extended mannose-binding lectin expression genotypes among patients with pediatric-onset systemic lupus erythematosus (SLE) and unrelated healthy controls. Values are number (%).
Associations between MBL expression genotypes and SLE clinical features
Table 2 shows the clinical characteristics of these patients with pediatric-onset SLE. When patients were categorized according to their MBL expression genotypes, there were no significant differences among the different MBL expression genotype groups for the occurrences of mucocutaneous lesions, arthritis, serositis, or hematologic and neuropsychiatric disorders.
Clinical presentations and MBL expression genotype distributions in children with SLE.
There were 81 children with SLE who underwent renal biopsies; most of them had WHO class IV nephritis (47 patients) that required aggressive immunosuppressive treatment. Biopsy findings among the others showed that 12 had class II nephritis, 9 had class III nephritis, and 4 had class V nephritis. For the 9 children with normal renal biopsy findings, they did not meet the renal involvement criteria of the ACR during the later followup period. A total of 72 children with SLE had renal disorders in this cohort.
Patients with the high MBL expression genotype had renal disorders more frequently than patients in the group with medium and low MBL expression genotypes (65.9% vs 41.9%; p = 0.013). After adjusting for age, sex, age at SLE diagnosis, disease duration, and disease-related laboratory measurements, patients with the high MBL expression genotype had an OR of 2.49 (95% CI 1.15–5.39, p = 0.021) for a renal disorder when compared to patients in the medium- and low-expression genotype groups. There were no significant differences between these genotype groups for sex, age at SLE diagnosis, followup duration, or the presence of different autoantibodies (data not shown).
Associations between MBL expression genotypes and infections
There were 42 patients (33.6%) with confirmed SBI and 21 patients (16.8%) with painful herpes zoster infection that required parenteral antibiotics or antiviral agent treatments (Table 3). Any episode of SBI or herpes zoster infection was recorded for 50 patients (40%). A total of 59 episodes of SBI were identified among these 42 patients; 13 patients had recurrent SBI. Most patients presented with a UTI (n = 20), followed by bacteremia (n = 18), pneumonia (n = 10), musculoskeletal infections (n = 6), cellulites (n = 4), and 1 with bacterial meningitis.
Associations of MBL expression genotypes with major infections in children with SLE.
There were 22 patients with SLE in the high MBL expression genotype group who had SBI and 20 patients in the medium and low MBL expression genotype group (26.8% vs 46.5%; p = 0.030), a difference that was significant. Patients with the high MBL expression genotype were less often infected by herpes zoster than patients in the medium and low MBL expression genotype groups (13.4% vs 23.3%; p = 0.208), although this difference was not significant. No statistically significant differences were found for the current prednisolone dose at the time of infection, the mean daily prednisolone dosage during the 3 months prior to infection, or the use of immunosuppressants between the patients with SLE who had high MBL expression genotypes versus patients with medium and low MBL expression genotypes. After adjustment for age, sex, age at SLE diagnosis, disease followup duration, SLE clinical manifestations, and disease-related immunosuppressant therapy, logistic regression analysis revealed that there was a protective effect against SBI among patients with the high MBL expression genotype when compared to patients with the medium and low MBL expression genotypes (OR 0.29, 95% CI 0.12–0.71, p = 0.007). The high MBL expression genotype also showed a protective effect against herpes zoster infections when compared to patients with the medium and low MBL expression genotypes (OR 0.30, 95% CI 0.10–0.95, p = 0.041). Thirty of the 42 patients with SLE who had SBI had their serum MBL levels checked when they acquired an SBI; their serum MBL level was 0.74 ± 0.51 μg/ml. It seemed that patients with SBI had lower MBL levels compared to those patients without SBI (data shown below), although this was not statistically significant owing to the small number of cases.
Relationships between MBL levels and MBL genotypes and SLE disease activity
There were 45 patients with SLE (38 girls and 7 boys) who were recruited for longitudinal MBL measurements. Their mean age (± SD) at SLE diagnosis was 11.60 ± 2.70 years and their followup duration was 2.49 ± 3.76 years. In the SLE active stage, the mean SLEDAI score was significantly higher than in the SLE inactive stage (22.50 ± 10.43 vs 2.50 ± 0.93; p = 0.011). In the SLE active stage, most patients (n = 44; 97.8%) were treated with high-dose prednisolone (> 0.2 mg/kg/day), while 23 (51.1%) received immunosuppressants. The percentage of patients taking prednisolone or immunosuppressants decreased significantly when these patients were in the inactive stage. Laboratory results during the SLE followup period showed significantly increased complement (C3, C4) levels, hemoglobin and albumin levels, reduced proteinuria, and decreased anti-dsDNA antibody levels (data not shown). In the active stage, the MBL concentrations of these patients with SLE were significantly higher than in the inactive stage (1.56 ± 0.55 μg/ml vs 1.08 ± 0.65 μg/ml; p = 0.001). Among these 45 patients with SLE, there were 27 patients who had renal disorders and 18 who did not. The serum MBL level in patients with renal disorders was 1.81 ± 0.74 μg/ml, and the level was 1.18 ± 0.28 μg/ml in patients without renal disorders (p = 0.562) when SLE was diagnosed. Serum MBL levels were not significantly different between patients with and without neuropsychiatric disorders or other SLE clinical manifestations.
Among these 45 patients with pediatric-onset SLE, 35 (77.8%) had the high-expression genotype, 9 (20%) had the medium-expression genotype, and 1 (2.2%) had the low-expression genotype. Among 30 healthy controls, 18 (60%) had the high-expression genotype, and the remaining 12 (40%) had the medium-expression genotype. No control had the low-expression genotype. The MBL levels (mean ± SD) are shown in Figure 1. For patients with SLE who were in the high MBL expression genotype, MBL serum levels in the active stage were higher than in the inactive stage (1.70 ± 0.48 μg/ml vs 1.25 ± 0.70 μg/ml; p = 0.022), and both of these levels were higher than for the controls with the same genotype (0.73 ± 0.35 μg/ml; p = 0.026). For those with the medium and low MBL expression genotypes, the mean MBL level was also higher in the active stage than in the inactive stage (1.25 ± 0.62 μg/ml vs 0.68 ± 0.27 μg/ml; p = 0.049), and both of these levels were higher than for controls with these genotypes (0.05 ± 0.03 μg/ml; p = 0.004). When study subjects bearing the high MBL expression genotype were compared to those with the medium and low MBL expression genotypes, the MBL levels remained significantly higher regardless of whether SLE activity was in the active or the inactive stage, even in the control group (p = 0.039, p = 0.030, and p = 0.003, respectively). Finally, serum MBL levels were positively correlated with the anti-dsDNA antibody levels (r = 0.239, p = 0.047) and SLEDAI scores (r = 0.342, p = 0.042) during the followup period. MBL levels were not significantly correlated with complement (C3, C4) levels.
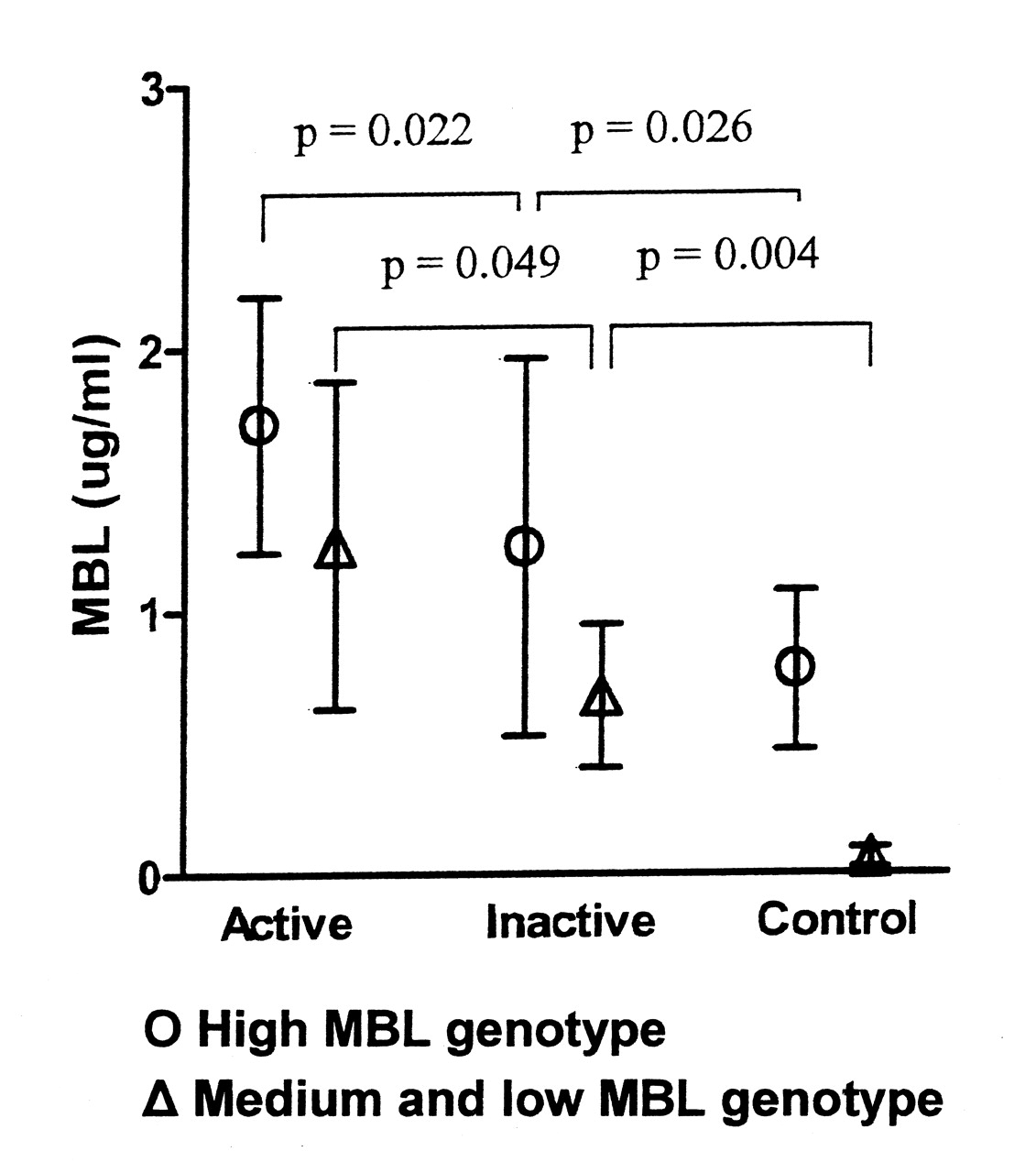
Patterns of mannose-binding lectin (MBL) level (mean ± SD) changes at different stages of SLE activity. In general, the MBL level remained higher for study subjects who had a high MBL expression genotype (SLE, n = 35; controls, n = 18) when compared to those with the medium and low MBL expression genotypes (SLE, n = 10; controls, n = 12). Patients with SLE in the active stage had significantly higher MBL levels compared with the inactive stage, and both these levels were higher than for controls.
DISCUSSION
In our longitudinal study, we investigated relationships for extended MBL expression genotypes among children with pediatric-onset SLE, as well as serum MBL levels during the disease course of SLE. The extended MBL expression genotypes have a pronounced influence on serum MBL levels5,6. We demonstrated that a high MBL expression genotype was a risk factor for renal disorders, while it had an apparent protective effect against serious bacterial infections.
Several studies have reported that SNP in the promoter or structural region of the MBL gene might be associated with SLE7,8, but there are limited data available regarding possible correlations of extended MBL expression genotypes with SLE. Moreover, no studies have investigated the extended MBL expression genotypes among patients with pediatric-onset SLE. In our previous study, we analyzed SNP in exon 1 of the MBL gene for patients with SLE, and found no significant findings for these single-variant genotypes with SLE clinical manifestations in a large cohort of patients with pediatric-onset SLE18. However, MBL expression phenotypes are not determined only by exon SNP, but rather are determined by the haplotypes of different promoter and exon SNP concomitantly. Therefore, in our present study, we further analyzed SNP in the promoter of the MBL gene and then analyzed the relationships between these children with SLE who had different MBL expression haplotypes. In our present study, we included 110 children with SLE from the previous SLE cohort18 and 15 children with SLE who were newly diagnosed after 2007. Our present and previous observations suggest that MBL gene polymorphisms, either in the structural region or in the promoter region, and the extended MBL expression genotypes are not associated with increased susceptibility to SLE among Chinese children.
The MBL expression genotypes did influence the clinical manifestations of SLE in our study. This finding is different from our previous study, which showed that single-variant genotypes in exon 1 of the MBL gene had no associations with SLE clinical manifestations. Our current results indicate that the high MBL expression genotype is associated with increased susceptibility to renal disorders in pediatric-onset SLE. Specifically, there was a 2.49-fold increased risk of a renal disorder in children with the high expression genotype compared to those with the medium and low MBL expression genotypes. The mechanisms underlying the involvement of MBL in the pathogenesis of renal disorders remain to be identified. Current evidence on the pathogenesis of diabetic nephropathy suggests that there is an association between developing renal complications and the presence of high-MBL-producing genotypes in patients who are diabetic26,27.
In children with SLE who have a high MBL expression genotype, enhanced gene transcription and the subsequent chronic increase in MBL production within the renal microvascular environment might result in excessive complement activation by the lectin pathway following local tissue damage. Accumulation of immune complexes, along with abnormal cellular and humoral responses, may lead to a cascade of events that are responsible for the development of a renal disorder. The clinical manifestations, immunological patterns, and outcomes vary greatly between patients with pediatric-onset and adult-onset SLE. Younger patients with SLE have more renal and neuropsychiatric involvements than do adult patients with SLE28,29,30. These findings suggest that the differences between pediatric-onset SLE and adult SLE may have a genetic foundation. Our study demonstrates that the high MBL expression genotype may contribute to an increased risk for a renal disorder in young patients with SLE.
Clinical features that predispose patients with SLE to infection are not well established15,31. We found that the low MBL expression genotype was a potential risk factor for infection in patients with pediatric-onset SLE. Bacterial infections are responsible for most infections in SLE and herpes zoster is the most common viral infection. Severe recurrent infections are one of the predominant causes of morbidity and mortality in children with SLE30,32. The infection rate was 40.0% in our study population, which was comparable to that of a previous case series study of children with SLE31. The prevalence of herpes zoster in our study was lower than that of a study of juvenile-onset SLE, but both studies found greater infection rates than for healthy children33. Several factors, either genetic (including complement deficiencies or mannose-binding lectin deficiency) or acquired (such as severe disease manifestations or immunosuppressant use), predispose patients with SLE to infections15,32,34.
Despite this awareness, it remains challenging for pediatric rheumatologists to make an early diagnosis and prescribe prompt treatments for infections in patients with SLE, as the clinical findings of bacterial infections and the flaring of SLE disease activity are very similar. Identifying which patients are at higher risk for severe bacterial infections and using preventive strategies are warranted in order to reduce the rate of infections and thus minimize the morbidity and mortality among children with SLE. We found that patients with SLE who had the medium and low MBL expression genotypes had an independent risk factor for SBI, while the high MBL expression genotype provided a protective effect against SBI. This is similar to findings by Garred, et al that indicated that patients with SLE who were homozygous for MBL variant alleles had a 4-fold increase in the incidence of infections that required hospitalization16. Additionally, Mok, et al found that low serum MBL levels predisposed Chinese patients with SLE to more major infections17.
MBL is produced in the liver and is a key molecule in innate immunity. It is also an acute-phase protein, and its expression is increased in inflammatory states8. Serum MBL concentrations are genetically determined by a series of extended MBL expression genotypes, and there is a low probability that medications can influence serum MBL levels. We found that the significantly elevated serum MBL levels during different SLE stages, as compared with healthy controls, were not limited to any particular MBL expression genotype. MBL appears to be an inflammatory marker. We observed significant reductions in serum MBL levels among patients with SLE who had achieved clinical improvements, suggesting an association of this protein with clinical disease activity and inflammatory status. Evidence supporting that MBL has an important role in modifying inflammatory responses has also been described in several different disease scenarios in children35,36.
Associations between serum MBL levels and the disease course of SLE have been previously reported37,38. Takahashi, et al found that serum MBL concentrations fluctuated during the SLE disease course, as MBL levels appeared to reflect disease activity only in some patients37. In addition to serum MBL concentrations, Seelen, et al also investigated functional MBL activities in patients with SLE38. Their study indicated that SLE disease activity was not significantly different between patients with MBL wild-type or variant alleles, between patients with high or low MBL concentrations, or between patients with high or low MBL complex activities. In our study, different SLE activity stages were reflected by significantly different serum MBL levels, and even in the SLE inactive stage, serum MBL levels were still significantly higher than those in the control group, independent of the MBL genotype. A possible explanation may be that, although clinical improvements had been achieved, reflected by the significant declines in SLEDAI scores and reductions in the prescribed medications, some types of inflammatory process continued insidiously in patients with SLE during the inactive stage. The value of serum MBL monitoring in clinical practice needs to be repeated on a larger scale and with different ethnic groups to determine if these findings can be generalized.
Limitations of our study are that only serum MBL levels, but not functional MBL activities, were examined and only a small number of patients were included for serial serum MBL measurements. Because there was typically a time lag between the initial presentations to the final diagnosis of SLE, and over a quarter of this study population had been referred from other hospitals to our tertiary medical center, the definitive time of SLE onset for most of the patients in this cohort could not be clearly documented. In order to check the MBL level only at the SLE onset stage, and to exclude the influence of infections on MBL changes, only 45 patients were enrolled for serum MBL measurements. In the future, more children newly diagnosed with SLE with clear SLE onset times should be recruited, and MBL activity assays should be included.
The extended MBL expression genotypes are not associated with susceptibility to SLE in children. In pediatric-onset SLE, the MBL expression genotype appears to play a dual role. For one, children with a high MBL expression genotype are at increased risk to develop a renal disorder. In contrast, a high MBL expression genotype has a protective effect against infection. Further investigations should be made of serum MBL concentrations in clinical SLE activity.
Acknowledgment
We thank Assistant Professor Chia-Hao Chang, Chang Gung Institute of Technology in Chia-Yi, for expert advice on statistical analysis; Susan Liao for data collection; and Ju-Hui Cheng, Hsiu-Li Chou, and Bi-Shuang Chu for collecting and processing specimens and for their technical assistance.
Footnotes
-
Supported by a Chang Gung Medical Research Progress Grant (CMRPG 460031) and National Science Council Grants (NSC 95-2314-B-182A-172-MY3 and NSC 98-2314-B-182-002-MY3).
- Accepted for publication February 10, 2011.








{kind=link}