

Abstract
Objective. To evaluate persistence with anti-tumor necrosis factor (TNF) therapy and predictors of discontinuation in patients with rheumatoid arthritis (RA).
Methods. This retrospective analysis used data from RADIUS 1, a 5-year observational registry of patients with RA, to determine time to first- and second-course discontinuation of etanercept, infliximab, and adalimumab. First-course therapy was defined as first exposure to anti-TNF therapy, and second-course therapy was defined as exposure to anti-TNF therapy after the first discontinuation. Kaplan-Meier survival analysis was used to assess persistence, log-rank tests were used to compare therapies, and Cox proportional hazards models were used to assess potential predictors of treatment discontinuation.
Results. This analysis included 2418 patients. Mean persistence rates were similar among treatments [first-course: etanercept, 51%; infliximab, 48%; adalimumab, 48% (followup was 54 weeks for etanercept and infliximab and 42 weeks for adalimumab); second-course: 56%, 50%, 46%, respectively (followup was 36 weeks for etanercept and infliximab and 30 weeks for adalimumab)]. Discontinuations of first-course therapy due to ineffectiveness were similar among treatments (etanercept, 19%; infliximab, 19%; adalimumab, 20%) and discontinuations due to adverse events were significantly (p = 0.0006) lower for etanercept than for infliximab (etanercept, 14%; infliximab, 22%; adalimumab, 17%). Predictors from univariable analysis of first- or second-course therapy discontinuation included increased comorbidities (etanercept), female sex (infliximab), Clinical Disease Activity Index > 22 (infliximab), and a Stanford Health Assessment Questionnaire score > 0.5 (adalimumab).
Conclusion. In this population, first- and second-course persistence was similar among anti-TNF therapies. First-course discontinuation due to adverse events was lower with etanercept compared with infliximab.
The availability of anti-tumor necrosis factor (TNF) agents has improved the management of rheumatoid arthritis (RA). The efficacy and safety of the anti-TNF agents etanercept, infliximab, and adalimumab have been widely investigated in RA. Key studies of etanercept, infliximab, and adalimumab have shown that these therapies are generally well tolerated, are associated with improvements in RA symptoms, and slow joint damage either alone or in combination with the disease-modifying antirheumatic drug (DMARD) methotrexate (MTX)1,2,3,4,5,6,7,8,9,10,11,12,13. Recently, 2 additional anti-TNF therapies, golimumab and certolizumab pegol, have been introduced for the treatment of RA14,15,16,17,18. Newly published observational studies of treatment trends from a US registry of patients with RA show that use of anti-TNF drugs is increasing in patients with both early and established RA and that physician preference is a significant determinant in choice of RA biologic therapy19,20.
Only limited information is available on the persistence of anti-TNF agents among patients with RA. Recent studies have examined persistence and reasons for discontinuation among real-world patients with RA treated with anti-TNF agents such as etanercept, infliximab, and adalimumab21,22,23,24. However, these studies vary greatly in design and disease characteristics. Two of the studies utilized US veterans or insurance claims databases to carry out retrospective analyses21,23, whereas 2 were observational studies derived from registries of European patients with RA22,24. Among these studies, patients varied in baseline demographic characteristics, including disease severity, comorbidities, and health insurance coverage. Ultimately, data from controlled clinical trials might not be optimal in an assessment of persistence because of inherent biases in clinical trials regarding baseline characteristics of included patients (e.g., lower rates of comorbidities), restrictive entry requirements, and short duration of therapy; thus, clinical trial data do not represent real-world practice.
The Rheumatoid Arthritis Disease-Modifying Anti-Rheumatic Drug Intervention and Utilization Study (RADIUS) was a 5-year multicenter observational registry that assessed the use patterns, efficacy, and safety of DMARD and biologics among patients with RA in real-world clinical practice25,26. The RADIUS registries represent 2 cohorts: RADIUS 1 evaluated patients with RA who initiated a new DMARD or biologic (addition or switch) at enrollment, and RADIUS 2 evaluated patients with RA who initiated etanercept at enrollment. The objective of this retrospective analysis was to evaluate longterm persistence and potential predictors of drug discontinuation with first- and second-course anti-TNF therapies among patients in RADIUS 1.
MATERIALS AND METHODS
Patients
The complete inclusion and exclusion criteria for RADIUS 1 were described previously25. Briefly, eligible patients (age ≥ 18 years) had RA as classified by the 1987 American Rheumatism Association criteria27 and required a new DMARD or biologic (addition or switch) at enrollment. All patients provided written informed consent, and the study was approved by the institutional review board of each participating site.
Study design
RADIUS 1 was a prospective, multicenter, observational registry conducted at 387 sites in the United States that included 4968 patients. Patients who initiated first-course etanercept, infliximab, or adalimumab during the study were included in this analysis. First-course therapy was defined as the first exposure to an anti-TNF agent at any time during the study. The study population included patients who were biologic-naive and patients previously treated with a biologic agent; prior exposure to biologic agents was not factored into the analysis. Second-course therapy was defined as initiation of any anti-TNF agent following the first discontinuation. Data were collected from baseline until discontinuation of treatment (up to 5 years) and were summarized for each of the 3 anti-TNF agents.
The main endpoints of the study were time to the first and second discontinuation of therapy. Discontinuations analyzed included those attributed to ineffectiveness and adverse events (AE). In addition, risk factors for first- and second-course anti-TNF therapy discontinuations (including first-course discontinuations attributed to ineffectiveness and AE) were assessed.
Assessments
Demographic assessments at baseline included age, sex, and race. Patient-reported baseline data included highest education level achieved, employment status, insurance coverage, and prescription payers. Physician-reported data at baseline included estimates of disease severity according to Clinical Disease Activity Index (CDAI) scores for mild (> 2.8 to ≤ 10), moderate (> 10 to ≤ 22), and severe (> 22) disease, disease duration, reason for treatment change, prednisone use at baseline, concomitant DMARD, use of anti-TNF therapy, and history of comorbidities.
Clinical assessments included tender and swollen joint counts (28 joints were assessed), Stanford Health Assessment Questionnaire (HAQ) score, physician and patient global assessments, pain visual analog scale score, and laboratory values including presence of rheumatoid factor (RF). The CDAI was calculated, and the incidences of serious AE and certain AE of interest were recorded. The time to first- and second-course anti-TNF therapy discontinuations was estimated.
Statistical analysis
Patient demographics and disease characteristics were summarized using descriptive statistics. Persistence on anti-TNF therapy (defined as the time from initiation to discontinuation) was assessed by Kaplan-Meier analysis. A log-rank test was used to compare persistence rates between anti-TNF agents. Kaplan-Meier analysis was used to estimate the survival function of time to discontinuation of anti-TNF therapy due to ineffectiveness and AE.
Univariable and multivariable Cox proportional hazards models were used to assess potential predictors of discontinuation of anti-TNF therapy, including first-course discontinuations attributed to ineffectiveness and AE. The following covariates were examined in the models: age (continuous, in years), sex (female vs male), race (white vs non-white), number of comorbid conditions, disease severity (based on CDAI score > 22 vs ≤ 22 prior to initiation of anti-TNF therapy), disease duration (continuous, in years), Medicare (yes vs no), employment status (employed vs unemployed), RF-positive (yes vs no), prednisone use at baseline (yes vs no), and HAQ score (continuous, prior to initiation of anti-TNF therapy). Data were presented as hazard ratios with 95% confidence intervals. All statistical calculations were performed using SAS software version 9.1 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Patients
A total of 4968 patients were enrolled in RADIUS 1 between October 2001 and January 2003. This analysis included 2418 patients; of these, 694 (29%) started etanercept, 1427 (59%) started infliximab, and 297 (12%) started adalimumab. Mean (SD) followup times were 3.2 (1.5) years for etanercept, 3.4 (1.5) years for infliximab, and 2.6 (1.2) years for adalimumab. Patient demographics and disease characteristics are shown in Table 1. Patients in the infliximab group were older; had longer disease duration; had more severe disease as shown by CDAI, HAQ, joint counts and global assessment; and had more concomitant DMARD use than patients in the etanercept and adalimumab groups (Table 1). About three-quarters of patients in each group had severe RA (defined as CDAI > 22), and approximately 80% of patients in each group were RF-positive.
Patient demographics and baseline disease characteristics. Values are mean (SD) unless otherwise specified.
Persistence with first-course anti-TNF therapy
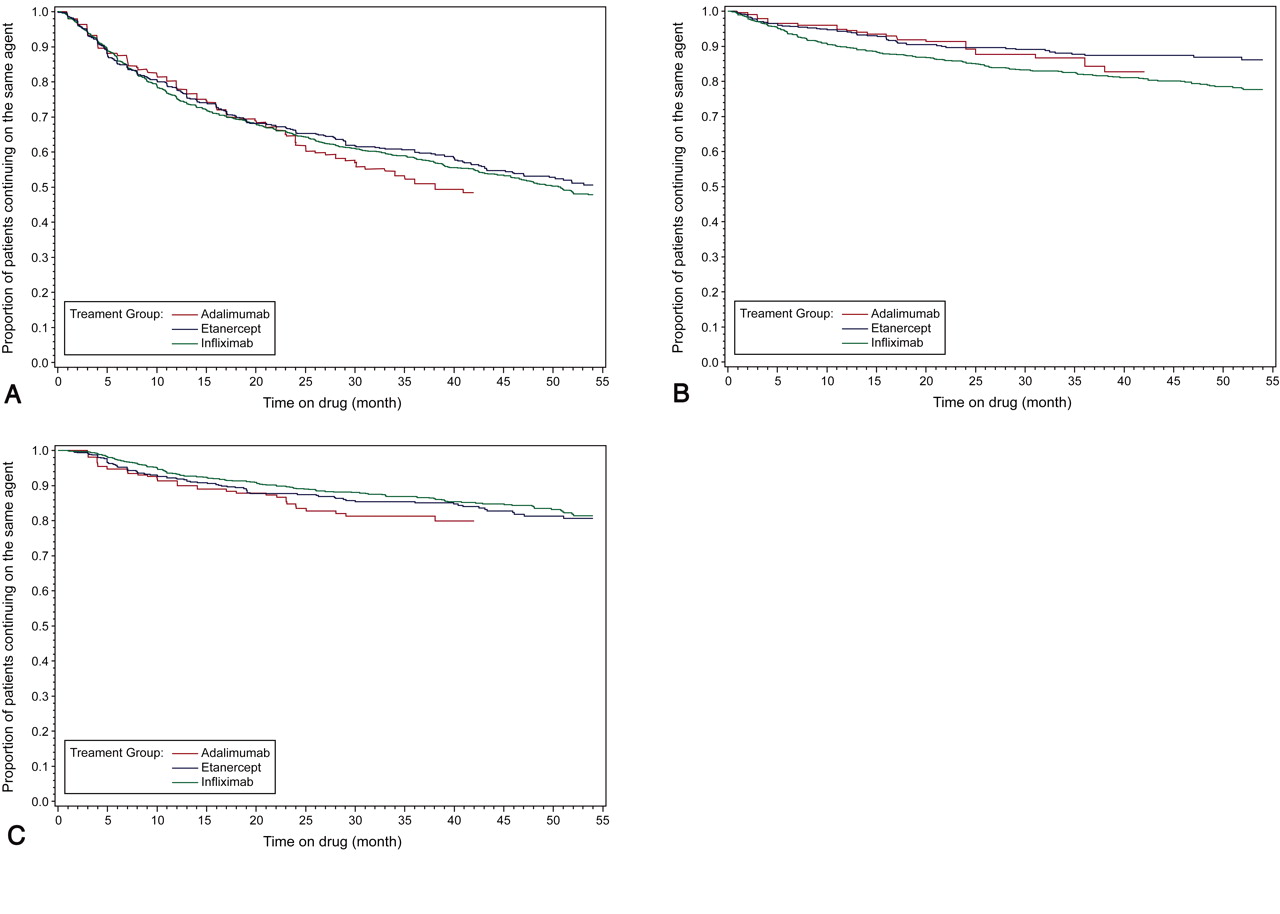
The rates of persistence and discontinuation due to AE or ineffectiveness during first-course anti-TNF therapy are shown in Table 2, and a Kaplan-Meier plot of time to discontinuation of each first-course anti-TNF therapy is shown in Figure 1A. Among patients who received etanercept and infliximab, persistence rates decreased similarly, reaching 51% and 48%, respectively, at 54 months. The persistence rate among patients who received adalimumab was 48% at 42 months. The percentage of patients who discontinued as a result of AE was significantly lower (p = 0.0006, log-rank test) for patients who received etanercept (14% at 54 months) compared with those who received infliximab (22% at 54 months; Table 2, Figure 1B). In the adalimumab group, 17% of patients discontinued at 42 months as a result of AE. The percentage of patients who discontinued as a result of ineffectiveness was similar among the 3 groups; patients who received etanercept and infliximab had discontinuation rates due to ineffectiveness of 19% each at 54 months, and patients who received adalimumab had a discontinuation rate due to ineffectiveness of 20% at 42 months (Table 2, Figure 1C).

A. Kaplan-Meier plot shows time to discontinuation of each first-course anti-TNF therapy. B. Percentage of patients who discontinued as a result of adverse events was significantly lower (p = 0.0006, log-rank test) for patients who received etanercept compared with those who received infliximab. C. Patients who received etanercept and infliximab had discontinuation rates due to ineffectiveness of 19% each at 54 months, and patients who received adalimumab had a discontinuation rate due to ineffectiveness of 20% at 42 months.
Persistence with first-course and second-course anti-tumor necrosis factor therapy.
The effect of disease control on persistence was also assessed in an exploratory analysis. There was significant evidence of a difference in mean CDAI score between those who persisted and those who discontinued treatment (p < 0.001). Mean CDAI scores at treatment stop date were significantly higher in those who discontinued than in those who persisted for the etanercept and infliximab groups. Mean CDAI scores for those who discontinued and those who persisted, respectively, were 26.2 and 16.8 (p < 0.001) for etanercept, 28.4 and 19.0 (p < 0.001) for infliximab, and 26.9 and 17.0 (p = 0.0513) for adalimumab.
Predictors of discontinuation with first-course anti-TNF therapy
The results of a univariable analysis of predictors of first-course anti-TNF discontinuation are shown in Table 3. Overall, white race (HR 0.71, 95% CI 0.52–0.97, p = 0.033) was associated with significantly lower etanercept discontinuation, and increased number of comorbidities (HR 1.21, 95% CI 1.00–1.47, p = 0.045) was associated with significantly higher etanercept discontinuation. Increased age (HR 0.99, 95% CI 0.98–1.00, p = 0.002) was associated with significantly lower infliximab discontinuation, and female sex (HR 1.24, 95% CI 1.01–1.51, p = 0.040) and disease severity (CDAI > 22; HR 1.35, 95% CI 1.08–1.69, p = 0.009) were associated with significantly higher infliximab discontinuation. For discontinuations resulting from AE, female sex (HR 2.27, 95% CI 1.03–4.98, p = 0.041) was associated with significantly higher etanercept discontinuation, and increased number of comorbidities (HR 1.24, 95% CI 1.04–1.48, p = 0.017) was associated with significantly higher infliximab discontinuation. For discontinuations resulting from ineffectiveness, increased age (HR 0.98, 95% CI 0.96–0.99, p < 0.0001) and Medicare insurance (HR 0.71, 95% CI 0.51–1.00, p = 0.050) were associated with a significantly lower infliximab discontinuation, and disease severity (CDAI > 22; HR 1.82, 95% CI 1.12–2.94, p = 0.015) was associated with significantly higher infliximab discontinuation. None of the assessed variables were associated with first-course adalimumab discontinuation in univariable models.
Univariable analysis of first-course anti-tumor necrosis factor therapy discontinuation. Values are hazard ratio (95% CI).
An ad hoc univariable analysis adjusting for concomitant MTX was conducted (Table 4). The results were similar to those without the adjustment for concomitant MTX (Table 3). The number of comorbidities and white race for any discontinuation with etanercept and Medicare use for discontinuation for ineffectiveness with infliximab were not statistically significant. Additionally, age (any discontinuation) and disease duration (discontinuation for ineffectiveness) assume statistical significance for infliximab.
Univariable analysis of first-course anti-tumor necrosis factor therapy discontinuation adjusted for concomitant methotrexate use. Values are hazard ratio (95% CI).
Because patients in the infliximab group were older at baseline compared with the other groups, an ad hoc univariable analysis was performed on the infliximab group that excluded patients enrolled in Medicare at baseline. Disease duration was associated with minimally higher discontinuation due to AE (HR 1.02, 95% CI 1.00–1.04, p = 0.027), and increased age (HR 0.98, 95% CI 0.96–0.99, p = 0.003) and disease duration (HR 0.96, 95% CI 0.93–0.99, p = 0.007) were associated with significantly lower discontinuation for ineffectiveness. These results are largely similar to those seen in the full analysis.
Overall, white race (HR 0.68, 95% CI 0.49–0.95, p = 0.022) was associated with significantly lower etanercept discontinuation (multivariable analysis data not shown). Increased age (HR 0.99, 95% CI 0.98–0.99, p = 0.0002) was associated with significantly lower infliximab discontinuation, and disease severity (CDAI > 22; HR 1.33, 95% CI 1.06–1.68, p = 0.016) was associated with significantly higher infliximab discontinuation. For discontinuations resulting from AE, female sex (HR 2.62, 95% CI 1.13–6.11, p = 0.025) was associated with significantly higher etanercept discontinuation, and increased number of comorbidities (HR 1.22, 95% CI 1.01–1.47, p = 0.041) was associated with significantly higher infliximab discontinuation. For discontinuations resulting from ineffectiveness, increased age (HR 0.97, 95% CI 0.96–0.98, p < 0.0001) was associated with significantly lower infliximab discontinuation, whereas disease severity (CDAI > 22; HR 1.75, 95% CI 1.08–2.85, p = 0.024) was associated with significantly higher infliximab discontinuation. None of the assessed variables were associated with first-course adalimumab discontinuation in multivariable models.
Results from an ad hoc multivariable analysis (data not shown) adjusting for concomitant MTX were similar to those without the adjustment. An ad hoc multivariable analysis was conducted for the infliximab group excluding patients enrolled in Medicare as described above for the univariable analysis. Younger age remained a significant predictor of persistence overall (HR 0.98, 95% CI 0.97–0.99, p = 0.0007), and increased disease duration (HR 1.02, 95% CI 1.01–1.04, p = 0.013) and employment status (employed; HR 1.53, 95% CI 1.03–2.28, p = 0.034) were significant predictors of discontinuation due to AE; and age (HR 0.97, 95% CI 0.96–0.99, p = 0.004) and disease duration (HR 0.97, 95% CI 0.94–1.00, p = 0.025) were significant predictors of discontinuation due to ineffectiveness.
Persistence with second-course anti-TNF therapy
Rates of persistence and discontinuation during second-course anti-TNF therapy are shown in Table 2, and a Kaplan-Meier plot of time to discontinuation of second-course therapy in Figure 2. In all cases there was an observed decrease in second-course versus first-course persistence rates. The largest decrease was for adalimumab (52% vs 65% at 24 mo), followed by infliximab (50% vs 58% at 36 mo) and etanercept (56% vs 61% at 36 mo).

Kaplan-Meier plot shows time to discontinuation of second-course therapy.
It is important to note that the number of evaluable patients for etanercept and infliximab during second-course anti-TNF therapy was smaller than the group analyzed for first-course anti-TNF therapy [etanercept, n = 248 for second-course therapy vs n = 694 for first-course therapy; infliximab, n = 130 for second-course therapy vs n = 1427 for first-course therapy; the number of evaluable patients for adalimumab was similar for second- and first-course therapy (n = 277 vs 297)]. Thus, defining predictors of discontinuation in second-course anti-TNF therapy was less powered due to the small number of patients for the second course. An increased number of comorbidities was associated with significantly increased discontinuation of second-course etanercept by both univariable (HR 1.40, 95% CI 1.08–1.82, p = 0.011) and multivariable (HR 1.43, 95% CI 1.10–1.87, p = 0.008) analyses (data not shown). In addition, by both univariable (HR 2.13, 95% CI 1.20–3.79, p = 0.010) and multivariable (HR 2.48, 95% CI 1.31–4.68, p = 0.005) analyses, a HAQ score > 0.5 was significantly associated with increased second-course adalimumab discontinuation.
DISCUSSION
This longterm retrospective study of anti-TNF persistence in the treatment of RA in the US showed that overall, first-course persistence was similar between etanercept, infliximab, and adalimumab groups. Second-course therapy persistence was also broadly similar among therapies. The percentages of patients discontinuing first-course therapy as a result of ineffectiveness were similar in the etanercept, infliximab, and adalimumab groups; however, discontinuation due to adverse events was significantly lower in the etanercept group compared with the infliximab group. First-course drug discontinuation was predicted by an increased number of comorbidities (etanercept group), female sex (infliximab group), and disease severity (CDAI > 22, infliximab group), whereas treatment persistence was predicted by white race (etanercept group) and increased age (infliximab group). An exploratory analysis showed that CDAI scores in the infliximab and etanercept groups at discontinuation were significantly higher in those who discontinued than in those who persisted, providing further support that disease control is an important aspect of treatment persistence. An ad hoc analysis showed that these results were similar after adjustment for concomitant MTX use. No adjustment was made for multiple testing in this exploratory analysis. Second-course drug discontinuation rates were significantly higher among patients with an increased number of comorbidities (etanercept group) and those with a HAQ score > 0.5 (adalimumab group).
Previous studies analyzed persistence rates and predictors of drug discontinuation in patients with RA treated with anti-TNF therapies with variable results. In a Swiss observational cohort of patients with RA (N = 2364) treated with at least 1 course of anti-TNF therapy from 1997 to 2006, discontinuation rate was significantly higher among patients treated with infliximab compared with those treated with etanercept or adalimumab22. The rate of discontinuation due to an AE (especially infusion reaction or systemic allergic reaction) was significantly higher with infliximab compared with etanercept or adalimumab, and largely accounted for difference in overall discontinuation rates between the 3 drugs. In contrast with the results from the Swiss observational cohort, a retrospective analysis of data from US insurance claims databases of patients with RA (N = 9074) initiating first-course anti-TNF therapy from 2000 to 2005 found that persistence was greater with infliximab treatment compared with that of etanercept and adalimumab21. In a retrospective analysis of US Department of Veterans Affairs (VA) medical records from 1999 to 2007, 47% of the 212 RA patients identified had switched or stopped their first anti-TNF therapy23. Similar to our results, disease activity scores including 28-joint count and HAQ scores were significant predictors of anti-TNF discontinuation or switching in the VA study23. Results from a retrospective analysis of records from patients from 2 Dutch RA registries (1997–2006 and 2003–2007) who discontinued first-course anti-TNF therapy as a result of inefficacy or AE suggested that second-course anti-TNF therapy may still demonstrate efficacy independently of prior discontinuations24.
Our study showed some differences in discontinuation and predictors of discontinuation among the anti-TNF treatments etanercept, infliximab, and adalimumab. One potential explanation for these differences is that time on RA treatment (and toxicity and efficacy associated with treatment) could vary before enrollment; these differences in previous RA therapy could affect response and discontinuation rates of treatments during this study. In addition, in a US insurance claims database analysis, higher out-of-pocket cost of treatment was associated with discontinuation of therapy during the first year of newly initiated treatment with etanercept and adalimumab in patients with RA28. Further, an analysis of claims from a US managed-health-care plan for the year 2005 showed slightly higher discontinuation among RA patients who received adalimumab (n = 1292) compared to those taking etanercept (n = 2537)29. The authors suggested that patients receiving etanercept were more likely to adhere to their medication regimen compared with patients receiving adalimumab because pharmacy- and RA-related costs were significantly lower among patients who received etanercept29. Thus, differences in patient baseline characteristics and costs related to individual treatments at the time of this study could help explain the variations in discontinuation rates and predictors of discontinuation among anti-TNF agents observed in this study.
Although clinical trials can reveal the safety and efficacy of a drug, they generally do so using a rigorously defined group of patients with low rates of comorbidities who respond well to treatment over a limited length of time. Our study was a large patient cohort representative of the general population that reflected real-world persistence with anti-TNF treatments for RA. Patients in this study included those with varying comorbidities and disease severity as well as patients who were naive to anti-TNF therapy, patients initiating their second anti-TNF agent, and patients treated with other DMARD. Other strengths of the RADIUS study were its longterm (5-year) followup and the generalizability of the results. Potential limitations of this study include a lack of randomization and patient groups that were not balanced with respect to sample size, both of which could influence the significance of the statistical tests. For example, patients in the infliximab group tended to be older and have more severe disease (options were limited for older patients because Medicare reimbursement was favorable for infliximab infusions over subcutaneous self-administration of etanercept or adalimumab), which might account for the higher discontinuations due to AE in this group. However, analyses excluding Medicare patients from the infliximab group were generally consistent with those observed in analyses without this adjustment. In addition, large sample sizes in this study result in statistical significance of comparisons, but the clinical relevance of these comparisons is less clear. Additional limitations are potential selection biases due to enrollment of patients in need of new therapy, which by definition excludes patients with successful management of RA, and biases due to availability of biologics. At the beginning of the study, supplies of etanercept were low and adalimumab had not yet been approved for the treatment of RA by the US Food and Drug Administration.
This analysis demonstrated that the overall treatment persistence with first- and second-course anti-TNF therapies was similar for patients receiving etanercept, infliximab, and adalimumab. In agreement with other studies, adverse events and inefficacy were prominent reasons for discontinuation. Rates of discontinuation as a result of AE were significantly lower among patients treated with etanercept compared with infliximab but were similar between patients treated with etanercept and adalimumab. Patients in the infliximab group may have been at higher risk for AE because they were older, had longer disease duration, received more concomitant DMARD, and had higher disease activity at baseline compared with patients in the other groups. Our results suggest that an increased number of comorbidities (etanercept group), female sex (infliximab group), and increased disease severity (infliximab group) could predict discontinuation during first-course treatment, whereas second-course treatment discontinuation was predicted by an increased number of comorbidities (etanercept group) and a HAQ score > 0.5 (adalimumab group) in patients with RA.
Acknowledgment
The authors thank Rick Davis, MS, RPh, whose work was funded by Amgen Inc., for assistance in drafting this report.
Footnotes
-
Supported by Immunex Corporation, a subsidiary of Amgen Inc., and by Wyeth.
- Accepted for publication February 25, 2011.








{kind=link}
{kind=link}