

To the Editor:
The complexity of surgical and medical problems associated with reimplantation of a loose hip prosthesis does not always render this procedure acceptable. In addition, certain drugs may enhance the quality of bone around the prosthesis1,2. We treated a patient with teriparatide following loosening of his hip prosthesis, which was implanted for the second time; further surgery was no longer an option.
The patient had osteoarthritis and had an uncemented prosthesis when he was 56 years of age; by the age of 61 years he required a reimplant, as a result of aseptic loosening. At the age of 74 years, he began to develop increasing pain and progressive loss of power. He had a history of dilated cardiomyopathy, and in view of this a surgical solution was ruled out. By the age of 77 years, he was treated with clodronate (100 mg intramuscularly weekly) and oral calcium (1.5 g daily) for 1 year. At age 78, radiographic imaging showed extensive loosening of the bone around the cup and a marked reduction in cortical thickness. Although he was already using a cane, he was advised to use 2 canes to allow partial weight-bearing. He was subsequently prescribed teriparatide (20 μg daily for 7 months). Prior to this treatment (Time 0) he underwent the following investigations: (1) Conventional radiography; computed tomography (CT) of the pelvis and left hip with assessment of bone mineral density (BMD) in the sacral promontory (S1); analysis of the bone region surrounding the prosthetic cup; analysis of the thickness of the femoral cortex in the calcar region and immediately below the calcar; and analysis of the cortex in the region adjacent to the tip of the prosthesis. (2) Clinical test: the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)3, used to measure pain, stiffness, and function in activities of daily living (ADL). (3) Laboratory tests: calcium, phosphorus, total alkaline phosphatase (ALP), bone ALP, osteocalcin, parathyroid hormone, collagen cross-linked C-telopeptide-I.
Four months after the start of the study (Time 1) the clinical and laboratory tests were repeated; 8 months later (Time 2), all tests were repeated. On followup at Time 1, the WOMAC showed a reduction in pain walking on flat ground and less dependence in ADL (Table 1). The stiffness had not changed. Laboratory tests (Table 2) showed activation of the markers referable to osteoblasts and inhibition of bone reabsorption.
WOMAC test results show changes in scores of absolute data (percentage differences) at baseline (T0), after 4 months (T1), and after 8 months of treatment (T2).
Markers of bone metabolism show changes in the main indices of bone metabolism: absolute (percentage differences) at baseline (T0), after 4 months (T1), and after 8 months (T2).
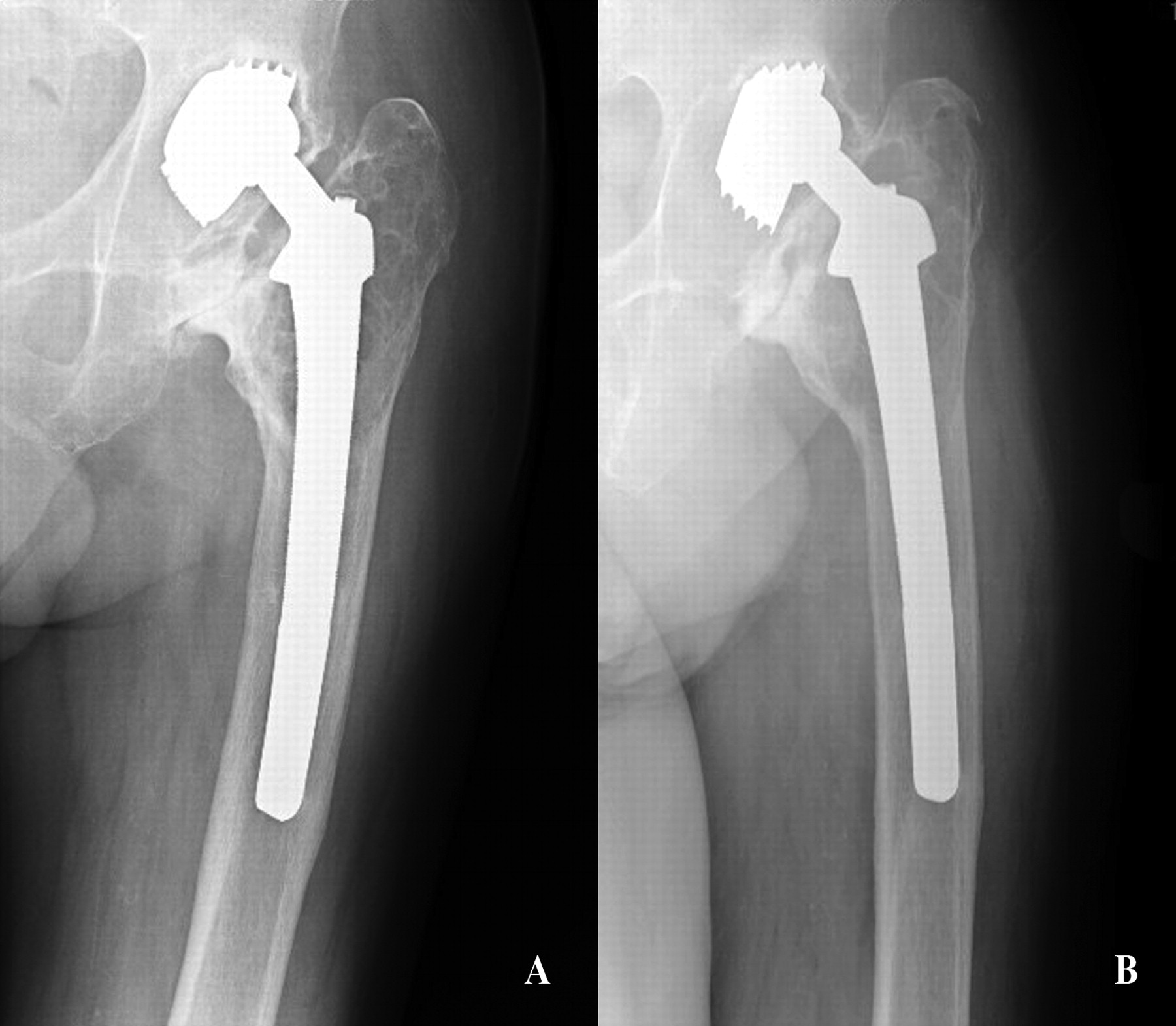
On followup at Time 2, radiography showed improvement of the bone stock in the calcar region (Figure 1). The CT (Table 3) showed the following results: (1) at S1 a change in BMD of +77.7% between T0 and T2; (2) in the region corresponding to the prosthetic cup, a slight increase of bone of the quadrilateral lamina (0.7 mm); (3) in the region of the femoral calcar and immediately beneath the calcar, the cortex appeared discontinuous at T0 with numerous areas of interruption; at T2 the CT showed reconstitution of the cortex (Figure 2): in the 2 areas where there had previously been an interruption of the cortical outline, the thickness was 2 mm and 3.3 mm, respectively; (4) at the tip of the stem, the cortex at T0 appeared intact but markedly osteopenic; at T2 the thickness was increased by 1.5 mm.
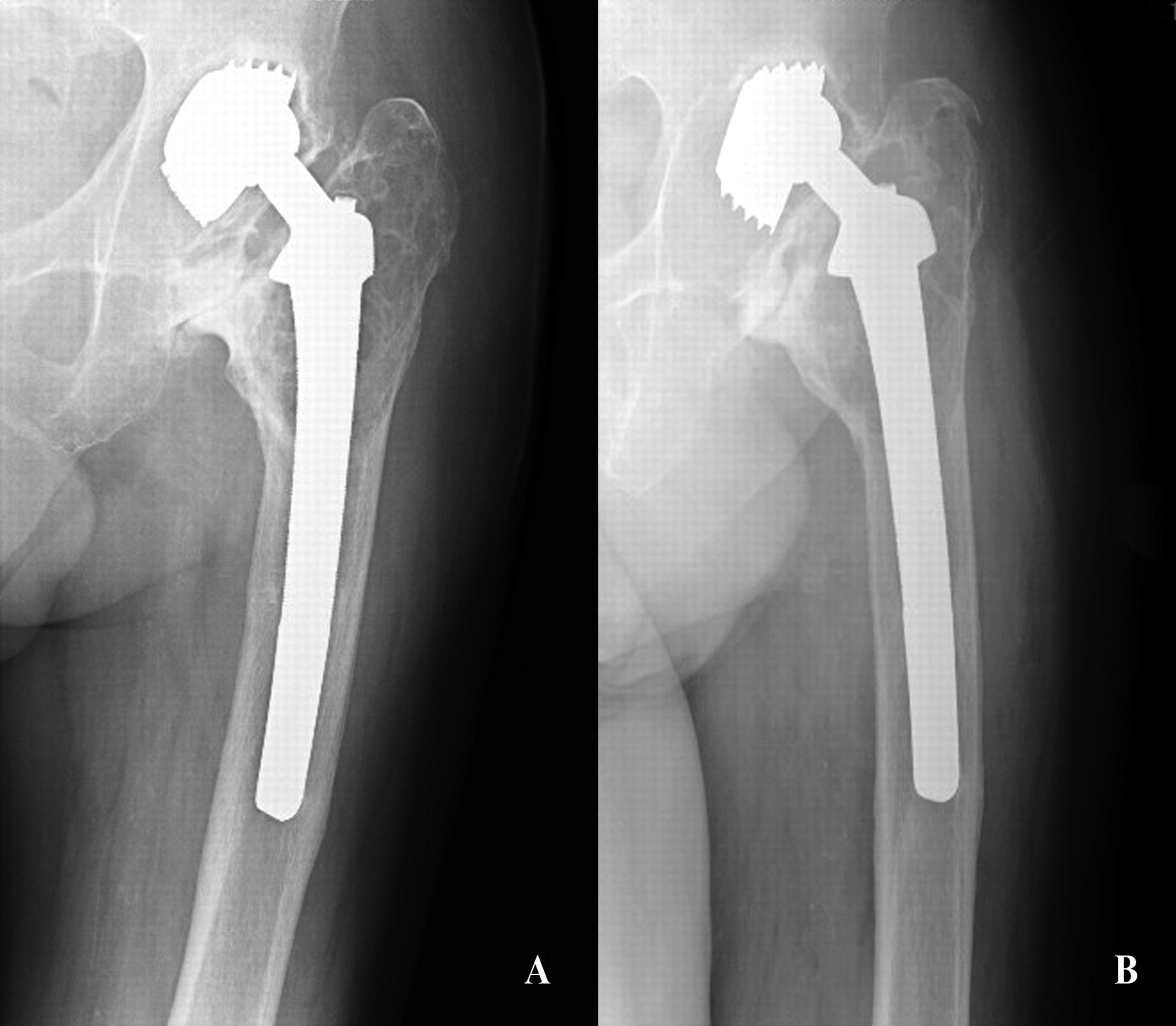
Conventional radiographs of calcar region of the femur show marked improvement of periprosthetic bone from baseline (A) and after 8 months of therapy (B).

Computed tomography of periprosthetic tissue at the level of the femoral calcar at baseline (A) and after 8 months of therapy (B). A. Discontinuity in the anterior region of the femoral diaphysis at T0. B. Reconstitution of the diaphysis after 8 months, at T2.
CT results: assessment of bone mineral density (BMD) in Hounsfield units (HU) at the sacral promontory (S1) in an area of 566 mm2. Measurement of periprosthetic bone thickness (in mm) at the apex of the acetabular convexity, the calcar, below the calcar, and at the apex of the stem; absolute and percentage differences between baseline (T0) and after 8 months (T2).
The WOMAC showed further improvement: walking on flat ground was no longer a source of pain and the patient was able to carry out ADL. In addition, joint stiffness had improved slightly. The laboratory tests showed a drop of resorptive activity at T2 compared with T1.
Our clinical case shows how it is possible to manage a loosened hip prosthesis with pharmacological therapy. The analgesic action of teriparatide has been described4,5; however, the level of independence achieved was similar to that often obtained after repeated implants.
CT scans confirmed the possibility of increasing BMD of both cancellous and cortical bone with teriparatide6,7. The increase in the cancellous bone achieved in just 8 months was striking. However, contrasting findings were observed at the acetabular level, where significant changes in the bone tissue were not recorded. In fact, at T0 the area surrounding the prosthetic cup was the site of extensive loosening and this may have altered the microenvironment required for effective osteogenesis. It is plausible that the use of a stabilizing support for the hip might improve the result. At the femoral diaphysis, however, we found reconstitution of cortical continuity at all levels that were examined; the patient’s greater stability and increased independence are probably due to this improvement. Finally, the laboratory results emphasized the metabolic action of the drug, according to a well known sequence of events8. We visited the patient several times following his treatment; the last time, 2 years after T0, the clinical picture was the same, the patient did not feel pain, and the level of autonomy was unchanged. The use of teriparatide for treatment of loosened and inoperable prostheses therefore seems rational9,10,11 and is a valid alternative to surgery; certainly, further clinical studies are advisable to complement these findings.








{kind=link}
{kind=link}