

Abstract
Objective. Patients with rheumatoid arthritis (RA), a chronic inflammatory disease, have increased cardiovascular morbidity and mortality. We investigated whether early markers of RA inflammatory disease activity could predict later increased levels of pulse-wave velocity (PWV) and augmentation index (AIx), 2 measures of arterial stiffness.
Methods. In total 238 patients with early RA were followed longitudinally and 108 were available for the 15-year followup examination. Comprehensive baseline clinical and radiographic data were collected in 1992. Arterial stiffness, measured as AIx and PWV (Sphygmocor apparatus), was recorded at the 15-year followup. Adjusted logistic univariate and multivariate analyses were performed with levels of AIx and PWV as the dependent variables, and variables reflecting baseline RA disease activity as possible predictors. The validity of the final models was examined in linear regression analyses.
Results. Baseline C-reactive protein (CRP) above the median predicted increased AIx (OR 3.52, 95% CI 1.04–11.90) and PWV (OR 4.84, 95% CI 1.39–16.83) at the 15-year assessment in multivariate models. Patients with elevated baseline CRP had significantly higher AIx (ß = 2.67, 95% CI 0.06–5.31, p = 0.045) and lnPWV (ß = 0.08, 95% CI 0.01–0.14, p = 0.02) after 15 years, after adjustments for age, sex, heart rate (AIx only) and mean arterial pressure.
Conclusion. Inflammation early in the RA disease course was associated with increased AIx and PWV after 15 years. These findings support the importance of early control of the inflammatory process in patients with RA.
- RHEUMATOID ARTHRITIS
- AUGMENTATION INDEX
- PULSE-WAVE VELOCITY
- CARDIOVASCULAR DISEASE
- C-REACTIVE PROTEIN
- INFLAMMATION
Nontraditional risk factors such as inflammation are associated with premature cardiovascular disease (CVD)1,2,3. Rheumatoid arthritis (RA) is a chronic, inflammatory disease of progressive joint destruction, and patients with RA exhibit a substantially increased cardiovascular mortality and morbidity4,5.
Measurements of arterial stiffness provide an established independent risk factor of CV mortality and morbidity6,7. The augmentation index (AIx) and pulse-wave velocity (PWV) are both derived from pulse-wave analyses, a reproducible method of estimation of arterial stiffness8. AIx9,10,11,12,13,14,15 and PWV16 have been shown to be increased in patients with RA. However, little is known of the effects of early RA disease activity on later levels of arterial stiffness.
We took advantage of the comprehensive data collection in the Euridiss cohort17,18 to examine the potential longitudinal influence of early inflammatory RA disease activity on AIx and PWV.
MATERIALS AND METHODS
Patients
We have longitudinally followed 238 patients with RA, diagnosed according to the 1987 American College of Rheumatology criteria19 and with < 4 years’ disease duration at inclusion in 1992. The mean age at baseline was 51.9 years (SD 13.0), 73.5% were female, mean disease duration was 2.3 years (SD 1.1), 60.5% were anti-cyclic citrullinated peptide (anti-CCP)-positive (concentration of antibody against CCP ≥ 25 U/ml), and 47.9% were IgM rheumatoid factor (RF)-positive (levels ≥ 25 U/ml)18. The patients were included after giving written informed consent. By the 15-year followup, 56 patients were deceased. One hundred eight patients participated at the 15-year followup (of whom 107 completed the questionnaires), and 74 patients declined to participate.
Baseline variables. Soluble biomarkers of disease activity
Erythrocyte sedimentation rate (ESR) was analyzed by Westergren method at the time of examination, whereas high sensitivity C-reactive protein (CRP) was analyzed from frozen sera samples (phyCardioPhase, nefelometri; Dade Behring, Deerfield, IL, USA). Anti-CCP and IgM RF, both strong prognostic markers in RA, were also analyzed from frozen sera using the ELISA method (Inova Diagnostics, San Diego, CA, USA and in-house method, respectively) as reported18.
Clinical biomarkers of disease activity
Disease activity was assessed by joint tenderness and the Ritchie score was calculated by summation of the number of tender joints according to the Ritchie protocol20. Joint destruction was measured by radiographic damage of the hands and scored according to the van der Heijde modified Sharp (vdHSS) criteria21. Baseline radio graphs were available for 84 of the 108 patients who participated in the 15-year followup. Radiographs not available had been damaged in storage and were missing at random.
Covariates and outcome measures. Demographics, clinical variables, and biomarkers
Details of known risk factors for CVD such as cholesterol, education level, and smoking status were recorded at the 15-year followup. Height and weight were measured and the body mass index (BMI) was calculated. Comorbidities were recorded by a trained study nurse at the 15-year followup. Disease activity at the 15-year followup was assessed by Disease Activity Score 28-joint count (DAS28; that is, 0.56 √ tender joint count + 0.28 √ swollen joint count + 0.70 lnESR + 0.014 patient global). Serum samples were analyzed consecutively at the time of patient visit and CRP at followup was measured using the Cobas 6000 analyzer (range 1–250 mg/l)22.
Arterial stiffness
At the 15-year followup we performed pulse-wave analysis assessments of the AIx and PWV using the Sphygmocor apparatus (Atcor, Sydney, Australia), which utilizes applanation tonometry, equalizing the circumferential pressure by slightly flattening the artery, to obtain accurate pressure waveforms. The central aortic waveform and the AIx are derived by applying a validated transfer system to recordings of the arterial pressure waves at the radial artery. AIx is defined as the change in pressure between the second and first systolic peaks as a percentage of the pulse pressure8. PWV is derived from the time recorded for the pulse wave to travel between 2 sites, where the distance between the sites is known. We chose to measure the carotid-femoral PWV between sites where the pulse was most strongly palpated on the carotid and femoral artery. The recordings of the foot of the pressure wave at the carotid and femoral artery were gated to an electrocardiogram (ECG) of cardiac activity23. Patients with atrial fibrillations were excluded from the analysis. Based on previous studies, patients were requested to abstain from food, drinks (except for water), and smoking for at least 3 hours prior to examination23. Several recordings were made in each patient, and the recordings considered to have the highest quality were selected for further analyses. For the AIx analysis our primary objective was to obtain recordings with an acceptable wave form, with sufficient pulse height and with minimal pulse-wave variation. For the PWV measurements we sought recordings where the pulse did not differ by more than 5 beats/minute between each examination site. Both these outcome variables were adjusted for mean arterial pressure, which was estimated from the peripheral waveform by the transfer function of the Sphygmocor and calibrated to peripheral pressures. Brachial blood pressure was measured in a standardized fashion using an Omron M7 after a 5-minute rest in a supine position. The measurement was repeated until 2 measurements had ≤ 5 mm Hg differences in both systolic and diastolic pressures and a difference in pulse ≤ 5, and a mean was calculated.
Statistical analysis
Baseline demographic variables were compared between participants and nonparticipants at the 15-year followup using chi-square test, Student t test, or Mann-Whitney U test as appropriate. Two-tailed p values are reported. PWV was log-transformed to achieve normality. We visualized values of AIx and lnPWV in cumulative probability plots, with separate lines according to elevated versus not elevated baseline CRP, and compared the groups using Student t tests. The plots depict values from each individual patient in order ranked from lowest to highest.
The association between baseline variables and later increased AIx and PWV, defined as values above the 75th percentile (dependent variables), were examined in parallel logistic regression procedures that were adjusted for age, sex, and mean arterial pressure. AIx was also adjusted for heart rate. Elevated ESR and CRP were defined at values above the median. Disease duration was entered as a dichotomous variable (< 2 vs ≥ 2 years’ disease duration), education was dichotomized as ≤ 12 versus > than 12 years, smoking was dichotomized as ever versus never having smoked, anti-CCP and IgM RF levels were categorized as < 25 U/ml versus ≥ 25 U/ml18. Variables that were significant at the p ≤ 0.1 level in these adjusted univariate analyses were entered into a multivariate logistic regression analysis and removed in a backward-step procedure until all variables (except sex) were significantly associated with the dependent variable. The validity of the final model was examined by entering the following possible confounders successively into the model: use of antihypertensive medication, presence of diabetes, current lnCRP, current total cholesterol, current lnBMI, and current DAS28 score. Previously excluded variables of baseline disease activity were also reexamined as possible confounders or effect modifiers. Finally, we applied the Hosmer-Lemeshow goodness-of-fit test.
The associations between (dichotomized) baseline elevated CRP and AIx and PWV at 15-year followup were also examined by linear regression, with AIx and lnPWV as dependent variables in separate models, levels of AIx and lnPWV were additionally compared across quartiles of baseline CRP by ANCOVA. All models were adjusted for age, sex, and mean arterial pressure, AIx was also adjusted for heart rate.
RESULTS
Descriptive data
Baseline demographic characteristics of the complete Euridiss cohort and of participants at the current 15-year followup are shown in Table 1. A comparison between participants and nonparticipants revealed that participants were significantly younger, had lower levels of inflammation, were less frequently IgM RF-positive, reported better function, and were more seldom users of glucocorticoids. At the 15-year followup 39 patients used antihypertensive medication, 7 reported diabetes, the mean CRP was 7.9 (SD 13.7), and mean BMI was 25.7 (SD 5.0).
Baseline variables for the complete Euridiss examination and for participants at the 15-year followup. Comparisons between participants and nonparticipants.
Prediction of arterial stiffness
One hundred two patients had acceptable recordings of AIx and 98 for PWV. The reasons for nonvalid readings of one or both variables were incomplete participation for 1 patient, atrial fibrillations or nonsinusoidal pulse in 4 patients, and poor quality readings in 5 patients. Separate cumulative probability plots illustrate the individual values of AIx and lnPWV across dichotomized baseline CRP values (Figure 1a, 1b, respectively).
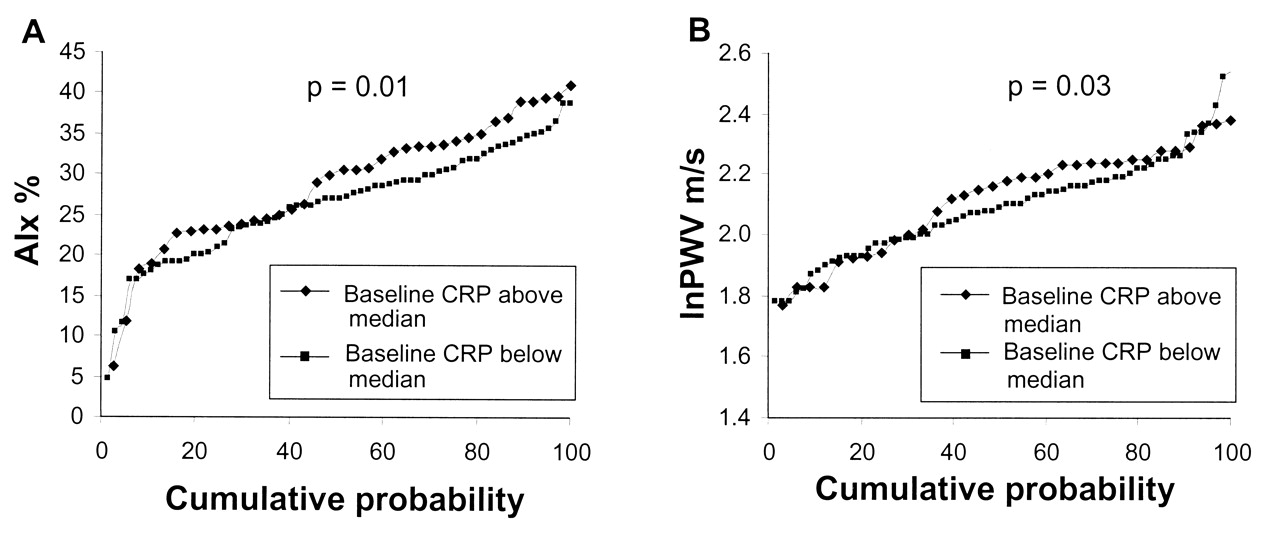
A. Cumulative probability plot of augmentation index (AIx) across dichotomized baseline CRP. Bivariate comparisons using Student t test (p = 0.01). B. Cumulative probability plot of pulse-wave velocity (PWV) across dichotomized baseline CRP. Bivariate comparisons using Student t test (p = 0.03).
The cutoff at the 75th percentile (increased AIx and PWV) was 34 for AIx (mean 27.2, median 28.0, range 2.5–47.0) and 9.8 for PWV (mean 8.4, median 7.9, range 4.8–14.2). Table 2 presents logistic regression models for prediction of increased AIx and PWV. Elevated baseline CRP (defined as values above the median) predicted increased AIx and PWV at the 15-year assessment in both the univariate and multivariate models. Baseline use of corticosteroids, baseline vdHSS and current DAS28, and use of statins and antihypertensive medication were all confounders on baseline CRP, increasing the odds ratio for increased AIx, but did not contribute independently to the model. Baseline IgM RF and elevated ESR, current DAS28, and current CRP similarly increased the odds ratio for increased PWV for patients with elevated baseline CRP, without contributing independently to the model. Female sex was identified as a significant positive effect modifier of elevated baseline CRP in the prediction of increased PWV.
Logistic regression models showing significant baseline predictors of increased augmentation index (AIx) and pulse-wave velocity (PWV). Logistic regression; all models are adjusted for age and sex and central mean arterial pressure; AIx model also adjusted for heart rate.
In the linear regression analyses, patients with elevated baseline CRP had significantly higher AIx (ß = 2.67, 95% CI 0.06–5.31; p = 0.045) and lnPWV after 15 years (ß = 0.08, 95% CI 0.01–0.14; p = 0.02) after adjustments for age, sex, and mean arterial pressure. There was a trend of increasing AIx and lnPWV across quartiles of baseline CRP (Figure 2a, 2b, respectively). However, this trend was not significant for AIx (p = 0.31) or for lnPWV (p = 0.12).

A. Augmentation index (AIx) across quartiles of baseline CRP. Models adjusted for age, sex, mean arterial pressure; AIx also adjusted for heart rate. B. Pulse-wave velocity (PWV) across quartiles of baseline CRP. Models adjusted for age, sex, mean arterial pressure, AIx, and also for heart rate.
DISCUSSION
We report that elevated inflammation early in the RA disease course is independently associated with increased AIx and PWV after 15 years. Other variables that were significantly associated with increased AIx and PWV were age, sex (AIx only), and current central mean arterial pressure.
The AIx is an estimation of the augmentation of central pressure that is caused by wave reflection. AIx has been shown to predict cardiovascular events and death in populations of atherosclerotic patients24,25,26, and central pressure estimations in some studies26,27, but not all studies28, have been shown to be independent predictors of cardiovascular events, outperforming brachial pressures29,30. The interest in central pressure measurements acknowledges that progression in arterial stiffness will affect the heart by enhancing wave reflection, and thus increase pressure in the ascending aorta and ventricles. Indeed, central pressure measurements derived from sphygmomanometry have been found to correlate with invasively measured pressure in the ascending aorta31 and with ventricular hypertrophy32.
Aortic PWV (commonly the carotid-femoral PWV) is a measure of the velocity of the pulse wave in the aorta and is currently accepted as the “gold standard” measure of arterial stiffness. The PWV is an established independent predictor of all-cause and cardiovascular mortality in populations both with and without pathological conditions25,30,33,34,35,36,37,38.
Arterial stiffness is caused by arterial wall fibrosis, elastin fractures, and calcification, a process closely related to arteriosclerosis and nonatherosclerotic CV disease33,39. Increasing blood pressure and arterial stiffness are part of the natural process of aging and pathologically inflated levels of these markers can reflect premature aging. Population studies have found that 10 years’ aging corresponds to an increase in PWV of 0.48 m/s in a young adult male, and 1.36 m/s in an elderly male40. AIx has been found to be significantly higher in women than in men, both in healthy populations40 and in cohorts of patients with RA16. All logistic regression models were therefore also adjusted for age and sex (Table 2). A baseline CRP above the median predicted an increase in later PWV of 1.1 m/s in our study, a level of change that could potentially be clinically significant.
AIx9,10,11,12,13,14,15 and PWV16 have been found to be increased in patients with RA. Our study suggests that AIx and PWV may be determined partly by inflammation early in the disease course. An association between both early and cumulative inflammation and CV mortality has been identified in RA3,41,42,43. Interestingly, cumulative inflammation was also shown to correlate with future AIx in 2 small studies of patients with longstanding RA14,44, whereas PWV was found to be cross-sectionally related to CRP in other studies16. Figures 2a and 2b suggest a stepwise increase in AIx and PWV across quartiles of baseline CRP, and although the trend is not significant, there is a significant increase in PWV between the lowest and highest quartile of baseline CRP (p = 0.03). If this trend is confirmed and found to be significant in a larger cohort, it would suggest a progressive worsening in arterial stiffness across small changes in baseline CRP. CRP has been found to be a robust predictor of CVD, and even slight increases are considered to be significant in the general population45. Although the CRP pentamer has been suggested to have a deleterious effect on the vascular endothelium46, more recent studies found that genetic polymorphisms that determine CRP levels are not related to CVD mortality or PWV47,48, and CRP is thus usually considered a biomarker of CVD without a causal role.
If arterial stiffness in patients with a chronic inflammatory disease is partly determined by early and cumulative inflammation in the disease course, then early and aggressively targeted therapy could reduce future CV morbidity and mortality in these patients. There are several reports that tumor necrosis factor-α (TNF-α) inhibition will reduce PWV in patients with RA15,16,49 for a period of up to 56 weeks50, illustrating that a change in the level of inflammation can influence future arterial stiffness.
The strengths of our study are the prospective longitudinal design with clinical examinations, blood sampling, and health status recorded at baseline. The major limitation of the study is the lack of information concerning baseline cardiovascular risk factors, including arterial stiffness measurements, which prevented us adjusting for these potential confounders in our prediction models. CRP levels are not determined only by inflammation: cardiovascular risk factors such as obesity and lack of exercise also contribute to increased CRP within the general population, and in patients with chronic inflammatory disease51. We were not able to define pathological levels of the biomarkers measured in this study as we did not include community controls. It would clearly also have been interesting to investigate channeling bias as an explanatory factor for the association between use of statins and increased PWV, but this was not possible. Available data on intercurrent use of antirheumatic therapies were also insufficient to explore the effects of treatment on later arterial stiffness. However, we expect that the medication has contributed to a reduced link between early inflammation and later arterial stiffness, since the patients with inflammation most likely would receive the most potent treatment including TNF inhibitors, which have been shown to reduce arterial stiffness.
Baseline measures of disease activity that can predict an increased risk of developing CVD are of interest. Our study shows that inflammation early in the RA disease course is associated with increased AIx and PWV after 15 years. It is established that early use of disease modifying antirheumatic drugs may reduce bone damage and disability, and our results support that early, active disease management to control inflammation in patients with RA may also help to reduce the risk of later CVD.
Footnotes
-
Supported by grants from the Eastern Norway Regional Health Authority. The Euridiss data collection was supported by The Research Council of Norway, The Norwegian Rheumatism Association, The Norwegian Women’s Public Health Association, the Grethe Harbitz Legacy, and the Marie and Else Mustad’s Legacy.
- Accepted for publication November 23, 2010.








{kind=link}
{kind=link}