

Abstract
Objective. To determine the benefits and harm of surgery for shoulder osteoarthritis (OA).
Methods. We performed a Cochrane Systematic Review of clinical trials of adults with shoulder OA, comparing surgical techniques [total shoulder arthroplasty (TSA), hemiarthroplasty, implant types, and fixation] to placebo, sham surgery, nonsurgical modalities, and no treatment. We also reviewed trials that compared various surgical techniques, reporting patient-reported outcomes (pain, function, quality of life, etc.) or revision rates. We calculated the risk ratio for categorical outcomes and mean differences for continuous outcomes with 95% CI.
Results. There were no controlled trials of surgery versus placebo or nonsurgical interventions. Seven studies with 238 patients were included. Two studies compared TSA to hemiarthroplasty (n = 88). Significantly worse scores on the 0–100 American Shoulder and Elbow Surgeons scale (mean difference, −10.05 at 24–34 mo; 95% CI −18.97 to −1.13; p = 0.03) and a nonsignificant trend toward higher revision rate in hemiarthroplasty compared to TSA (relative risk 6.18; 95% CI 0.77 to 49.52; p = 0.09) were noted. With 1 study providing data (n = 41), no differences were noted between groups for pain scores (mean difference 7.8; 95% CI −5.33 to 20.93), quality of life on Medical Outcomes Study Short-Form 36 physical component summary (mean difference 0.80; 95% CI −6.63 to −8.23), and adverse events (relative risk 1.2; 95% CI 0.4 to 3.8).
Conclusion. TSA was associated with better shoulder function, with no other demonstrable clinical benefits compared to hemiarthroplasty. More studies are needed to compare clinical outcomes between them and comparing shoulder surgery to sham, placebo, and other nonsurgical treatment options.
Shoulder osteoarthritis (OA), characterized by narrowing of the glenohumeral joint, presents with shoulder pain, limitation of shoulder function, and disability. Shoulder pain affects 5%–21% of adults in the United States and Western countries1,2,3,4,5,6 and is associated with significant disability3,7,8, disability claims9, and increased healthcare use10. Among the most common causes of shoulder pain are rotator cuff tendinitis, adhesive capsulitis, and shoulder OA11. A spectrum of rotator cuff disease accompanies shoulder OA, ranging from incidental findings of small rotator cuff tears in the setting of primarily OA-related symptoms to massive rotator cuff tears seen with rotator cuff arthropathy. Thus, shoulder OA is associated with significant morbidity, especially in the aging population.
Current nonsurgical treatment options for chronic shoulder pain due to shoulder OA are limited and may be associated with significant adverse outcomes, especially in the elderly. Nonsteroidal antiinflammatory drugs may cause renal insufficiency and/or peptic ulcer disease12,13. Intraarticular corticosteroid injections and physiotherapy may provide benefits, as they do for other shoulder conditions14,15, but their benefits in shoulder OA have not been proven. Intraarticular hyaluronic acid injections have been investigated for treatment of persistent shoulder pain in patients with shoulder OA16 and others, but their benefit over placebo is still debated.
The surgical treatment options for shoulder OA that were the focus of this Cochrane Systematic Review are usually done on patients who have failed conservative management and have disabling pain and limitation of shoulder function. These options included total shoulder arthroplasty (TSA)17, hemiarthroplasty18, arthroscopic debridement19, interpositional arthroplasty, and cartilage repair/implant. TSA is the surgical replacement of both the glenoid and the humeral head with implants; while hemiarthroplasty is the surgical replacement of only the humeral head with an implant. Patients with glenohumeral arthritis and an intact or reparable rotator cuff typically have a total shoulder arthroplasty. Patients with glenohumeral arthritis and an irreparable rotator cuff tear traditionally have a hemiarthroplasty. Surgical treatment of shoulder OA appears to be associated with a significant improvement in pain, function, and quality of life20. Recently, the American Academy of Orthopedic Surgeons published its guidelines on the treatment of glenohumeral OA, addressing surgery among other treatment options21. The objective of this systematic review was to assess the benefit and harm of surgical approaches, as compared to placebo, other conservative options, or to each other.
MATERIALS AND METHODS
Inclusion and exclusion criteria and search methodology
We considered all published randomized clinical trials (RCT) or controlled clinical trials (methods of allocating participants to a treatment that are not strictly random, e.g., date of birth, hospital record number, or allocation of alternate patients for study. We included studies of adults (age > 18 years) with shoulder joint OA, and excluded those of adults undergoing surgery for benign or malignant tumors, adhesive capsulitis, shoulder instability, or fractures. We included studies comparing any shoulder surgery (e.g., TSA, hemiarthroplasty, arthroscopy with debridement, interpositional arthroplasty, or cartilage repair/grafting) with placebo or sham surgery, nonsurgical modalities (e.g., intraarticular corticosteroid injections, physical therapy, or acupuncture), no treatment, or comparing different types of surgery.
We searched the following databases: (1) The Cochrane Central Register of Controlled Trials (CENTRAL), through The Cochrane Library, Wiley InterScience (www.thecochranelibrary.com), 3rd issue; (2) OVID Medline, 1966–September 11, 2009; (3) CINAHL (through EBSCOHost), 1982–September 11, 2009; (4) OVID SPORTdiscus, 1949–September 11, 2009; (5) Embase 1980–September 11, 2010; and (6) Science Citation Index (Web of Science) 1945–September 11, 2009.
Data collection and analysis
Following identification of potential trials for inclusion, 2 review authors independently extracted data from the included studies, including source of funding, study population, number of centers, number of surgeons, duration of operation, intervention, analyses, and outcomes, using standardized data extraction forms. We extracted raw data for outcomes of interest (means and SD for continuous outcomes and number of events for dichotomous outcomes), when available in the published reports. When possible, we extracted numbers based on intention-to-treat analysis.
Assessment of risk of bias in included studies
Two review authors independently assessed the risk of bias of each included trial22, checking for random sequence generation; allocation concealment; blinding of participants, personnel and outcomes; incomplete outcome data; selective outcome reporting; and other sources of bias, such as pharmaceutical funding and patients crossing over to other treatment groups. Each of these criteria was explicitly judged as yes (low risk of bias); no (high risk of bias); or unclear (either lack of information or uncertainty over the potential for bias).
Outcome measures
For primary outcomes, we examined all a priori specified outcomes at the latest followup in each study. The co-primary benefit outcomes were pain and disability, and primary harm outcomes included (1) pain, on visual analog scale, numeric rating scale, or semiquantitative descriptive scales such as the short-form McGill pain scale (range 0–45; higher denotes worse pain)23 or other instruments; (2) disability/function measured using common shoulder-specific instruments such as Constant score24, University of California at Los Angeles Shoulder Scale25, American Shoulder and Elbow Surgeons Shoulder Score (ASES)26, Neer rating27, disability of the arm, shoulder and hand questionnaire28, or the Western Ontario Osteoarthritis of the Shoulder Index (WOOS)29; and (3) adverse events — total, serious, and specific (local such as shoulder stiffness, instability, infection, nerve damage, and systemic such as thromboembolism, other pulmonary, cardiac, gastrointestinal, and others), and number of withdrawals and deaths.
Secondary outcomes included (1) quality of life, assessed by generic instruments, such as the Medical Outcomes Study Short-Form 36 (SF-36; 0–100; higher scores are better) and other similar instruments; (2) patient-evaluated or physician-evaluated success of treatment, including patient satisfaction; (3) function as assessed by range of motion (active and passive), strength, recurrence of symptoms, return to work and sport; and (4) revision/reoperation.
Data analyses
The patient was the unit of analysis. We calculated mean differences for continuous outcomes and risk ratios with corresponding 95% CI for dichotomous outcomes. We calculated relative difference in the change from baseline as the absolute benefit divided by the baseline mean of the control (placebo) group. Number needed to treat to benefit or harm (NNT) was calculated using the Visual Rx NNT calculator for categorical outcomes30. For continuous outcomes, we calculated the NNT using the Wells calculator software available from the Cochrane Musculoskeletal Group.
For studies judged as clinically homogeneous, we used the I2 statistic to test statistical heterogeneity, interpreted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions31: 0–40%, not important heterogeneity; 30%–60%, moderate heterogeneity; 50%–90%, substantial heterogeneity; and 75%–100%, considerable heterogeneity. We used a random-effects model as the default option to be conservative, independent of the I2.
Summary-of-findings table
We present the main results of the review in summary-of-findings tables, with a priori chosen outcomes (pain, disability/function, total adverse events, number of withdrawals due to adverse events, serious adverse events, revision rate), as recommended by The Cochrane Collaboration32. The summary-of-findings table included an overall grading of the evidence related to each of the main outcomes, using the Grading of Recommendations Assessment, Development, and Evaluation working group approach33.
RESULTS
Description of studies
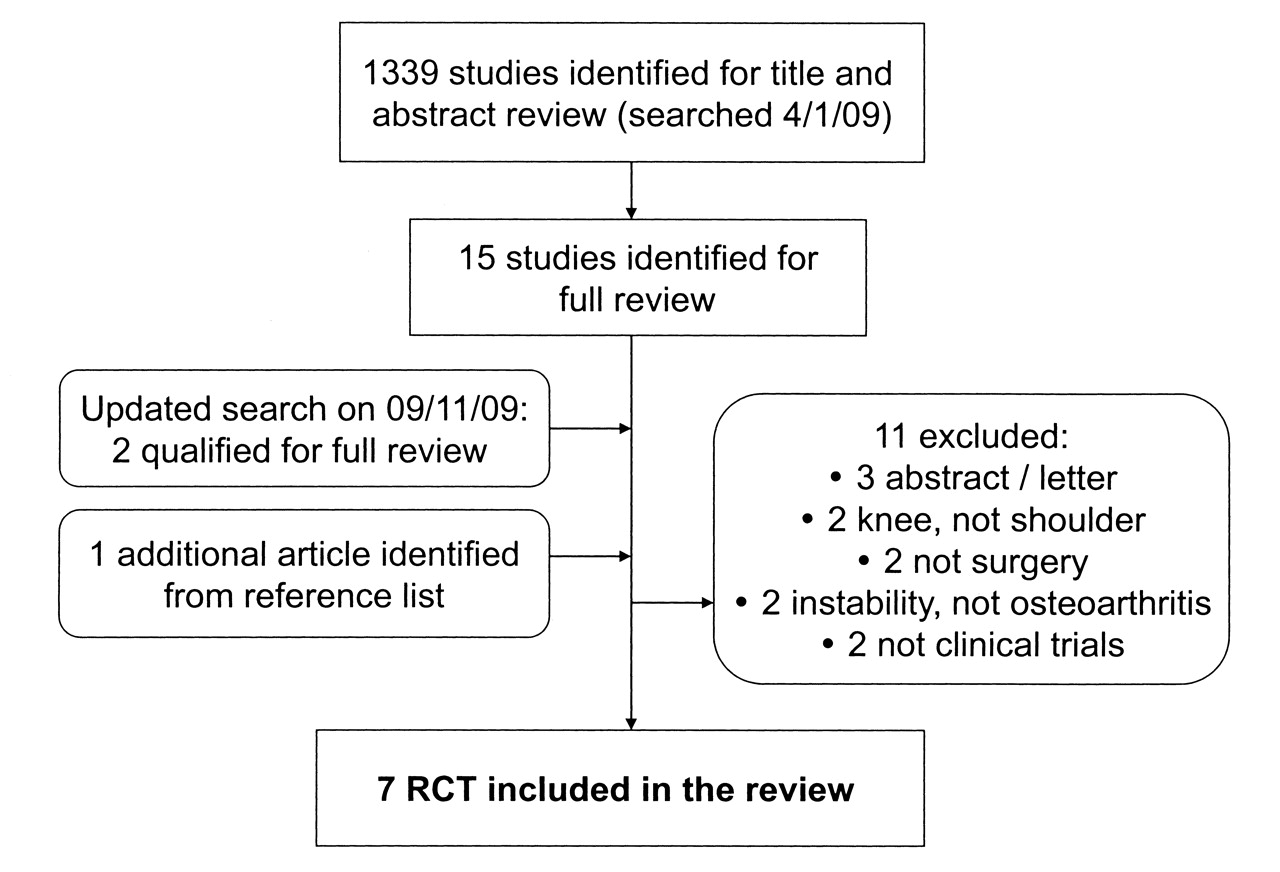
From the initial and updated searches of 1409 studies, 17 studies qualified for full review34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50, of which 7 RCT with 238 patients were included34,35,36,37,38,39,40 (Figure 1). One additional study found through references of included studies did not qualify for inclusion51.

Process of choosing studies for the review.
Sample sizes of included RCT ranged from 20 to 47 and followup ranged from 1.5 months38,40 to 36 months39 (Table 1). There were no trials comparing surgery to placebo or other nonsurgical options. Two trials (n = 47 and n = 41) compared TSA to hemiarthroplasty34,35 and both were of similar duration (24 to 36 months). Three trials compared keeled to pegged glenoid components (pegged design has 3 to 4 pegs to secure the glenoid and the keel has 1 central piece) with 2736, 2037, and 43 patients38; study duration was 1.5 months38 versus 24 months36,37. One trial compared the computerized navigation method for angulation of the glenoid component to conventional surgery with a followup at 1.5 months (n = 20)40. One trial compared outcomes of cemented all-polyethylene versus uncemented metal-backed glenoid component at 36 months (n = 40)39.
Characteristics of the included studies.
Risk of bias
In general, there was medium-high risk of bias across all the included studies because of small sample size and lack of blinding (Table 2). Most studies did not describe in detail how sequence generation occurred. The use of sealed envelopes was the only allocation concealment technique described in a few, but not all, studies. Only 1 study had low risk of bias for blinding36. Three studies did not report on participant withdrawals35,38,40.
Risk of bias of included studies. “Unclear” means that not enough information was available to make a determination regarding that criterion.
TSA versus hemiarthroplasty
Two of the 6 prespecified outcomes for the summary-of-findings table (serious adverse events and withdrawals due to adverse events) were not presented in any study (Table 3). For most outcomes, data were available from only 1 study and no heterogeneity was noted between study estimates for the few outcomes where 2 studies provided data. Compared to TSA, patients who underwent shoulder hemiarthroplasty had significantly worse ASES total scores, higher revision rates, and nonsignificantly worse pain and WOOS scores (Table 3). No significant differences in total adverse events were noted (Table 3). Additional outcomes are summarized in Table 4. No between-group differences were noted in SF-36 scores, infections, or intraoperative fractures.
Summary of findings (SOF) comparing TSA and hemiarthroplasty.
Comparison of other outcomes between hemiarthroplasty and TSA, keeled vs pegged glenoid component, cemented all-polyethylene vs metal-backed glenoid component, and intraoperative navigation vs conventional surgery.
Keeled versus pegged glenoid component
Three studies compared keeled to pegged glenoid components36,37,38. No significant differences were noted between groups in function on Constant and Murley score, patient-evaluated success of treatment, and reoperation rates (Table 4). Radiographic lucencies were significantly higher in keeled compared to pegged components; data were combined from 2 studies with wide variation in followup duration (6 weeks vs 24 months; Table 4).
Navigation versus conventional surgery
With 1 study (n = 20) providing data40, the retroversion angle was significantly smaller and operating time significantly longer for navigation compared to the conventional surgery (Table 4). No patient in either group had any intraoperative or postoperative complications.
DISCUSSION
There were no randomized trials that compared surgery to nonsurgical treatment for OA in the shoulder; therefore, the benefits and harms of surgery for shoulder OA as compared to nonsurgical therapies or usual care are unknown. Based on this analysis of published RCT data, it is not known whether surgery for OA shoulder provides benefits over usual care and/or nonsurgical treatment. This implies that research needs to be done in this area. Studies should examine patients with shoulder OA with and without rotator cuff tendinitis separately, since outcomes may differ based on the presence of rotator cuff tendinitis.
Our findings agree with corresponding findings from the American Academy of Orthopedic Surgeons (AAOS) guidelines for treatment of glenohumeral OA21. It is reassuring that independent systematic reviews found the same randomized trials. Similar to our review, the AAOS group found (1) no level 1 evidence (high-quality RCT) comparing surgical options with sham/placebo or nonsurgical options for treatment of shoulder OA; (2) that level 2 evidence (2 RCT with small sample sizes) supported TSA over hemiarthroplasty for glenohumeral joint OA; and (3) that level 2 evidence (low-quality RCT) supported the use of keeled or pegged glenoid components. It is interesting that inclusion of non-RCT data in the AAOS guidelines did not lead to difference in their interpretation compared to our conclusions based on clinical trial data alone. We also reviewed evidence on intraoperative versus conventional surgery and cemented all-polyethylene versus uncemented metal-backed glenoid components, not presented in the AAOS guidelines.
All included studies in this systematic review compared surgeries (TSA vs hemiarthroplasty), glenoid components (keeled vs pegged), surgical techniques (navigation vs standard procedure), and implantation (cemented all-polyethylene vs metal-backed). Studies consisted of small samples and, therefore, were liable to type II error, i.e., missing a significant difference when one actually exists. Sample sizes of 20–40 patients are unlikely to provide any meaningful clinical answers for patients and/or providers. Future studies need to be adequately powered to detect meaningful differences between groups.
Several findings from the studies deserve further discussion. In the TSA versus hemiarthroplasty comparison, the main findings were that ASES total score (disability/function and pain composite) improved more in the TSA compared to the hemiarthroplasty group; this difference exceeded the clinically meaningful change of 6.4 points and minimum detectable change of 9.6 points, as reported previously52. Differences in all other outcomes, including pain, revision rate, and range of motion, although favoring TSA, were not statistically significant. The revision rate was slightly higher in the hemiarthroplasty group than in the TSA group, although this did not reach statistical significance (p = 0.09). Thus, based on results from 2 studies including a small number of patients, TSA seemed to lead to significantly greater improvement in disability compared to hemiarthroplasty. We speculate that the main reason for discrepant findings regarding disability and pain/quality of life outcomes is that a very small number of patients were available for analyses and, except for a very few outcomes (for which 2 studies were available), data were only available from 1 study. Most patients with shoulder OA and irreparable rotator cuff disease have hemiarthroplasty compared to those with intact rotator, who are likely to have TSA, a selection bias that may partially explain the difference in postoperative function between groups. Different levels of technical skills required for different approaches/implants may be partially responsible for the few differences we found.
In the keeled versus pegged glenoid component comparison group, the main findings were that there were no significant differences in any of the primary or secondary outcomes. Disability/function, patient-evaluated success of treatment, and revision rate did not differ by type of glenoid component. The proportion of participants with radiographic lucency was significantly higher in the keeled glenoid component group than in the pegged glenoid component group, which may imply that longterm loosening rates may differ between keeled versus pegged components. However, this analysis combined 2 studies with varying lengths of followup (6 weeks vs 24 months). Therefore, these results should be interpreted with caution.
Intraoperative navigation was associated with significantly better glenoid positioning as measured by the retroversion angle and took longer than the conventional surgery. Intraoperative and postoperative complications were not noted in any patients in either group. None of our primary or secondary outcomes were assessed in this study. In the cemented versus uncemented glenoid component group, the main finding was that there was no difference in revision rate between the 2 groups.
Our study has several strengths. We performed a Cochrane Systematic Review with predefined outcomes and published protocol, assessed outcomes of relevance to patients and surgeons, and performed duplicate data abstraction. The risk that bias was introduced by the methods used is low, as all authors strictly followed the protocol outlined in this review. However, our review has several limitations, including a lack of relevant available trials, high risk of bias in included studies, and the lack of sufficient data to make firm conclusions regarding the benefit and harms of surgery for shoulder OA. Many trials did not assess the outcomes outlined in the review, or there was only a single trial with relevant data and therefore, the evidence gathered did not answer important questions. Our primary question, whether surgical versus nonsurgical treatments for shoulder OA differ in outcomes, could not be addressed because of a lack of studies in that area.
Our results were similar to those found in Bryant, et al53, a systematic review and metaanalysis comparing outcomes after TSA and hemiarthroplasty in patients with shoulder OA using data from RCT. That review included both published and unpublished data, including both studies included in our study (unpublished version of Lo, et al) and 2 other unpublished studies. Bryant, et al concluded that TSA provided better functional outcomes than hemiarthroplasty, but no significant differences were found between groups for range of motion, pain, and strength. Our results were similar in that we found better improvement in function in the TSA group than in the hemiarthroplasty group, but did not find differences between groups for pain, quality of life, or range of motion. It is unclear to us why the other unpublished RCT included in the earlier review have not been published.
Based upon the results of 2 trials, TSA may provide better functional outcomes than hemiarthroplasty, although other outcomes were similar. For other comparisons, sample sizes were small and findings need to be confirmed with larger studies. Our study does not help us answer important questions, such as who might be an appropriate candidate to undergo TSA, when surgery should be considered, and how much better are TSA and other surgical options compared to ongoing usual care and/or nonsurgical treatment options. There is a need for more research comparing the benefit and safety of surgery and nonsurgical treatment options for OA of the shoulder. There are several unique challenges to conducting RCT for surgical interventions. Because of the initial learning curve among surgeons, rapid improvement in technology leading to changes in implant designs, changes in surgical techniques over the duration of a short-intermediate term study, and need for large sample sizes due to ceiling effects in quality of life and function scores are some of the challenges in the conduct of randomized controlled trials in arthroplasty. The need for a long followup to observe meaningful differences may be cost-prohibitive. However, similar sample size and cost issues exist in large safety trials of pharmaceutical agents, requiring trials of 10,000–15,000 patients for 1–4 years. Such trials have been performed in recent years by requirement of the U.S. Food and Drug Administration. In the absence of such large trials in patients undergoing arthroplasty, prospective observational studies, with the creation of regional and/or national shoulder arthroplasty registries, may provide answers to many important questions.
Acknowledgment
We thank Louise Falzon and Renea Johnston of the Cochrane Musculoskeletal Group for their help in performing the searches and for suggestions regarding the protocol.
Footnotes
-
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the U.S. Department of Veterans Affairs.
-
This is a reformatted version of a Cochrane Review, which is available in The Cochrane Library, Issue 7, 2010. Cochrane Reviews are regularly updated as new evidence emerges and in response to feedback, and The Cochrane Library should be consulted for the most recent version of the Review.
-
Supported by the National Institutes of Health Clinical Translational Science Award 1 KL2 RR024151-01 (Mayo Clinic Center for Clinical and Translational Research) and from the resources and facilities at the Birmingham VA Medical Center. Dr. Buchbinder is supported in part by an Australian National Health and Medical Research Practitioner Fellowship.
- Accepted for publication October 29, 2010.








{kind=link}