
Abstract
Objective. The objective of this cost-of-illness study was to assess the use of direct medical resources, excluding drug costs, by patients with rheumatoid arthritis (RA) in France, and to construct cost estimates according to level of disease activity.
Methods. Three categories of RA disease activity were defined according to Disease Activity Score 28-joint count (DAS28) thresholds: remission (DAS28 < 2.6), low disease activity state (LDAS; i.e., DAS28 ≤ 3.2), and moderate to high disease activity (MHDAS; i.e., DAS28 > 3.2). Eight resource utilization items were defined: medical visits, laboratory tests, hospitalization, imaging, physiotherapy, nursing, adaptive aids, and transportation. Resource utilization and unit costs from the national-payer perspective were estimated through expert opinion and simulated using distribution ranges for each item. Cost distributions were computed by Monte-Carlo simulations estimating overall costs per 6 months over a 2-year period.
Results. For patients achieving remission, costs were estimated at a mean of €771 (SD 199) for the first 6 months and at €511 (SD 162) for each subsequent 6-month period. For patients achieving LDAS, costs were estimated at €905 (SD 263) for the first 6 months and €696 (SD 240) for each subsequent 6-month period. For patients in MHDAS, costs were estimated at €1215 per 6 months (SD 405).
Conclusion. This cost-of-illness assessment provided current estimates of direct medical costs for RA according to disease activity in France. The findings suggest that achieving remission or LDAS is associated with substantially lower medical costs for RA versus being in MHDAS.
- COST OF ILLNESS
- RHEUMATOID ARTHRITIS
- DISEASE ACTIVITY SCORE
- MODELING
- FRANCE
Evaluating the economic impact of rheumatoid arthritis (RA) for patients and the healthcare system is an important prerequisite for allocating resources and managing the disease. Such evaluation requires considering the complex epidemiology of the disease and estimating the spread of the disorder in the general population. Taking epidemiological data into account, the total annual economic cost of RA is estimated at €42 billion in Western Europe (2006)1. In France alone, the total costs of RA were estimated at $5.7 to 7.1 billion US in 19982. These estimates appear high because they include different types of costs associated with managing RA: the cost-of-illness framework includes direct costs, indirect costs, and intangible costs3. Indirect costs represent resources lost due to patients’ inactivity, such as production losses due to disability, unemployment, and premature death. In addition, any chronic disease negatively affects one’s quality of life, considered by some investigators as “intangible costs”4. Since quality of life should be measured using only generic or specific questionnaires, it is difficult to estimate intangible costs in monetary value, especially for a disease such as RA that includes high levels of chronic pain. Total RA cost analyses vary in the average per-patient cost estimates due to a high cost discrepancy between patients who require hospitalization during the evaluated period and those who do not5,6.
In this report, we focus on direct costs associated with managing RA in France from the public-payer perspective. Given that biological therapeutic strategies can be compared using robust cost-effectiveness studies7,8, we decided to focus on non-drug-related medical management resources in this study9.
MATERIALS AND METHODS
As this study aimed at estimating RA treatment costs per disease activity states, a standard costing approach was chosen for this purpose given the existence of specific medical guidelines and local “standard practices” to provide health resource utilization estimates based on “real life.” Each resource item was allocated to each disease activity state according to clinical guidelines and existing evidence8,10,11. Then health resource utilization variability was expressed by expert opinion in defining 95% confidence intervals for each item between a minimum value and a maximum value. Direct medical costs were estimated per 6 months, calculated from the 8 resource utilization items of RA medical management in France. 95% confidence intervals of each item were derived from frequency ranges for each Disease Activity Score (DAS)-based category (i.e., the disease activity state: remission, low disease activity, and moderate to high disease activity). Costs for each item (e.g., radiograph costs or nurse visit costs) were expressed considering a minimum to a maximum value, according to 2008 tariff ranges in the French healthcare system, using a uniform distribution. Similarly, frequency of each item (e.g., number of radiographs in 6 months, or number of nurse visits in 6 months) was expressed using a minimum and maximum value (based on medical practice variability in France) and a uniform distribution (except for hospitalization, which, in agreement with clinical experts, was programmed using a triangular distribution, i.e., using 3 variables: minimum, most likely value, and maximum). Using a national-payer perspective, unit costs were derived from published national tariffs (for drug costs: Journal Officiel de la République Française 2008; for other costs: tariffs from the French national illness funds).
Any potential variabilities around these standards were defined and validated by an expert rheumatology panel. In this study, a panel of 3 expert clinicians (LG, AS, and PG) advised on the variability of each resource utilization item and achieved clinical consensus according to current medical practices in France. Three categories of disease activity were defined according to DAS28 (DAS 28-joint count) thresholds: remission state, defined as DAS28 < 2.6; low disease activity state (LDAS), defined as DAS28 ≤ 3.2; and moderate to high disease activity state (MHDAS) defined as DAS28 > 3.2. Eight significant RA resource utilization items of medical management have been selected: medical visits, laboratory tests, hospitalization, imaging, physiotherapy, nursing, adaptive aids, and transportation. Distribution of each item was derived from frequency ranges according to French clinical guidelines for each disease activity category (remission, LDAS, MHDAS). Unit costs were expressed in euros (2008 values) calculated according to the French national-payer perspective from national tariffs (French national illness funds; Table 1)12,13. Differences in medical resource utilizations between the first and the following 6-month periods have been taken into account. Unit costs from the national-payer perspective were collected and simulated using distribution ranges for each item.
Resource utilization costs, given in euros.
Uncertainty was optimally managed considering the distributions for each variable in the context of a probabilistic sensitivity analysis, which uses Monte Carlo simulation modeling using random numbers to account for the effects of uncertainty. Consequently, for each random sample of the variables, average total costs are recalculated, and cost distribution per disease activity categories can be displayed. Using 5000 Monte Carlo simulations, each possible value of variable distributions was randomly taken into account in the calculations, allowing full screening of all potential probabilities and the construction of robust distribution shapes to express the results.
RESULTS
For patients achieving remission, the number of rheumatologist visits and biologic tests was estimated between 1 and 6 during the first 6-month period and 1 to 3 during the following 6-month periods. The number of radiographs (hands and feet) was estimated at between 1 and 4 over 2 years. About 30% to 60% of patients in remission needed 2 to 6 nurse visits over the first 6-month period, followed by 1 to 3 afterwards. Five percent to 10% of patients in remission have been estimated to need adapted shoes, and 15% to 60% adapted soles every 2 years. It was estimated that 2% of patients walked with canes and would need to change them every 5 years. Ninety percent of patients in remission benefit from reimbursed transportation for medical visits, and 10% were estimated to need medical transportation by ambulance. Between 0% and 10% of patients in remission were estimated to be hospitalized between 0 and 20 days over 6 months, but most likely only for 1 day. Sixty percent to 70% of patients in remission were estimated to have up to 1 other specialist visits per year.
For patients achieving LDAS, the number of rheumatologist visits was estimated to be from 1 to 6 during the first 6-month period and 1 to 4 in the subsequent 6-month periods. The number of biologic tests was estimated from 2 to 6 during the first 6-month period and 1 to 4 during the following 6-month periods. The number of radiographs (hands and feet) was estimated at between 1 and 2 over 2 years during the first 6-month period and 1 to 4 in the following 6-month periods. Between 30% and 60% of patients in LDAS were estimated to need 2–6 nurse visits over the first 6-month period and 1–4 afterward. Five percent to 10% of patients in LDAS were estimated to need adapted shoes and 20%–60% adapted soles every 2 years. Five percent of patients in LDAS were estimated to need hand orthoses every 2 years and 0.5% needed one wheelchair every 10 years. Three percent of patients were estimated to need canes every 10 years. Fifty-five percent to 85% of patients in LDAS were estimated to benefit from reimbursed transportation for medical visits (90% by car and 10% by ambulance). Up to 15% of patients in LDAS were estimated to be hospitalized between 0 and 20 days over 6 months, but most likely for only 1 day. Sixty percent to 70% of patients in LDAS were estimated to have up to one other specialist visit per year.
For patients in MHDAS, the number of rheumatologist visits was estimated to be from 1 to 6 over 6 months, with 2 to 6 biologic tests. The number of hand and foot radiographs was estimated between 1 and 2 over 6 months and 1 per year for the main joints. Between 30% and 60% of patients in MHDAS were estimated to need 2 to 6 nurse visits over 6 months. Ten percent of patients were estimated to have an average of 12 physiotherapist visits. Five percent to 10% of patients were estimated to need adapted shoes, and 30%–60% adapted soles every 2 years. Ten percent of patients were estimated to need hand orthoses and 5% need a cervical collar every 2 years. One percent of patients were estimated to need a wheelchair in 10 years and 5% would need canes every 10 years. Sixty percent to 90% of patients in MHDAS were estimated to benefit from reimbursed transportation for medical visits (90% by car and 10% by ambulance). Five percent to 25% of patients were estimated to be hospitalized between 0 and 20 days over 6 months, but most likely for only 1 day. Sixty percent to 70% of patients in LDAS were estimated to have up to 3 other specialist visits per year.
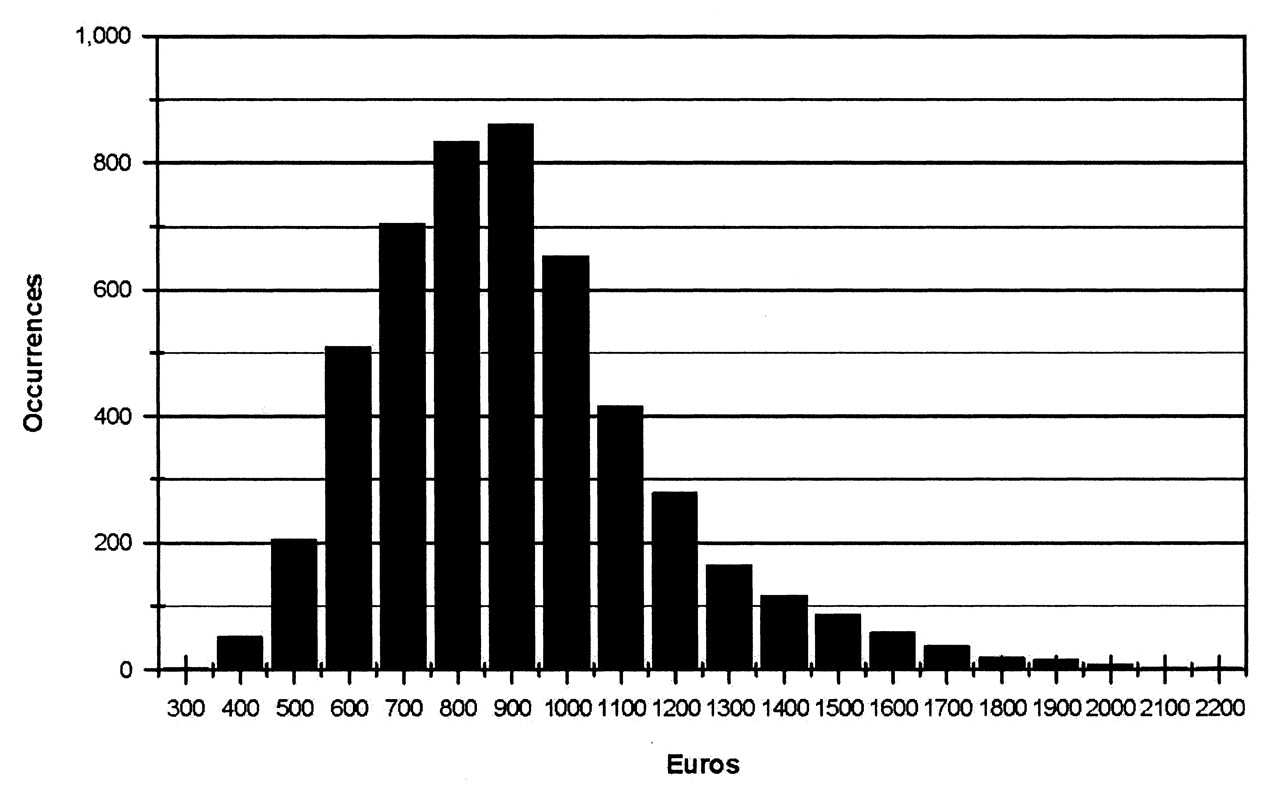
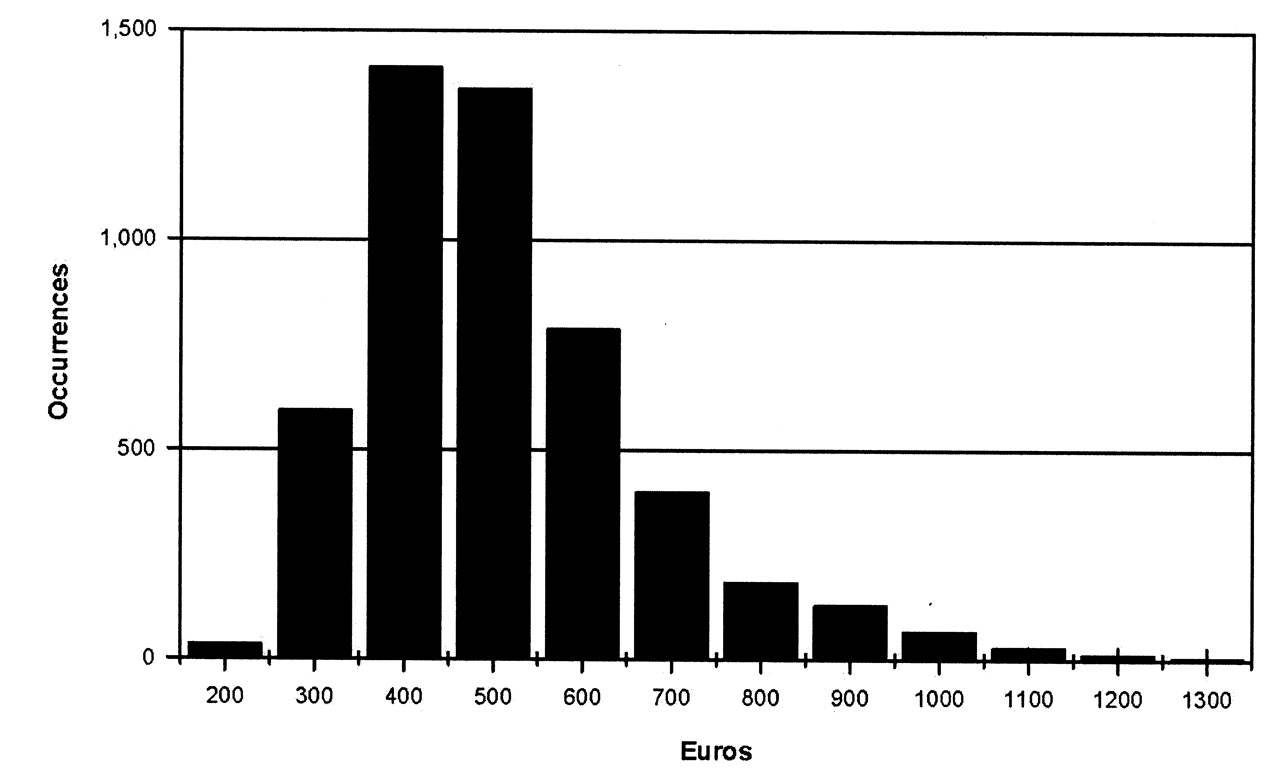
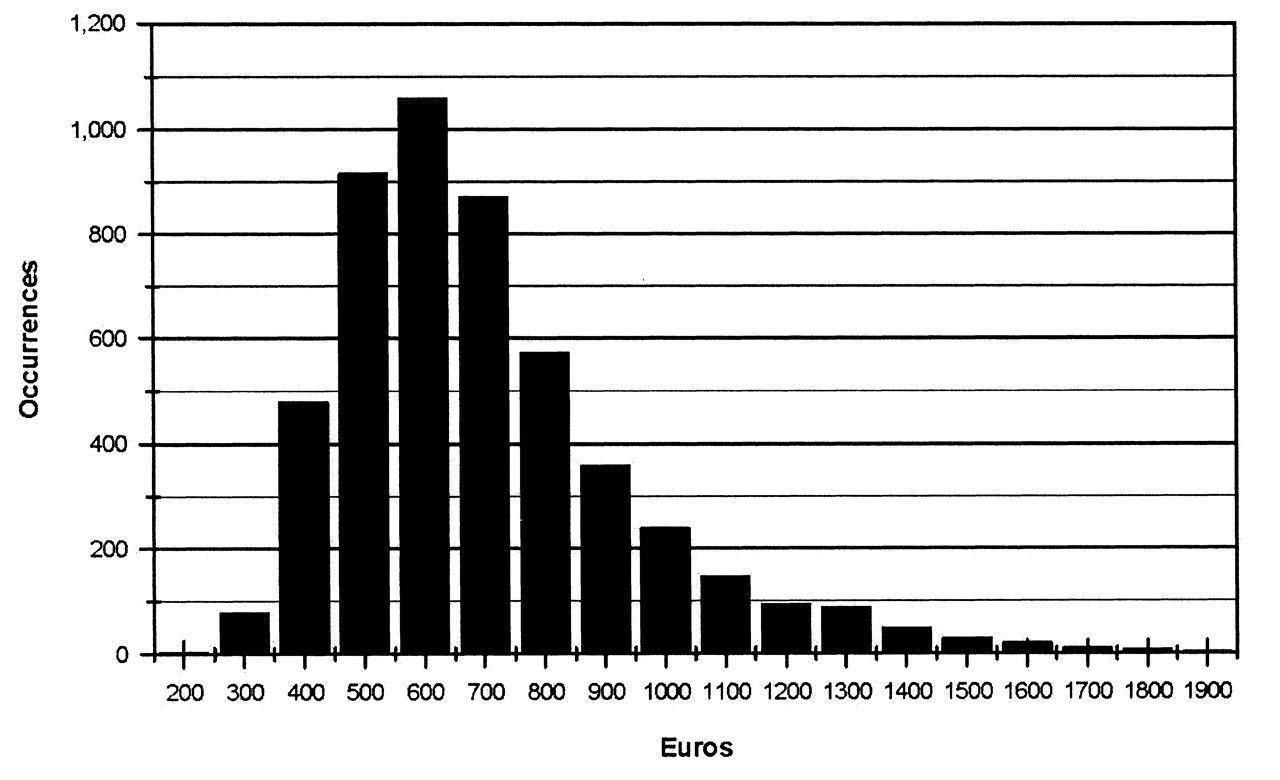
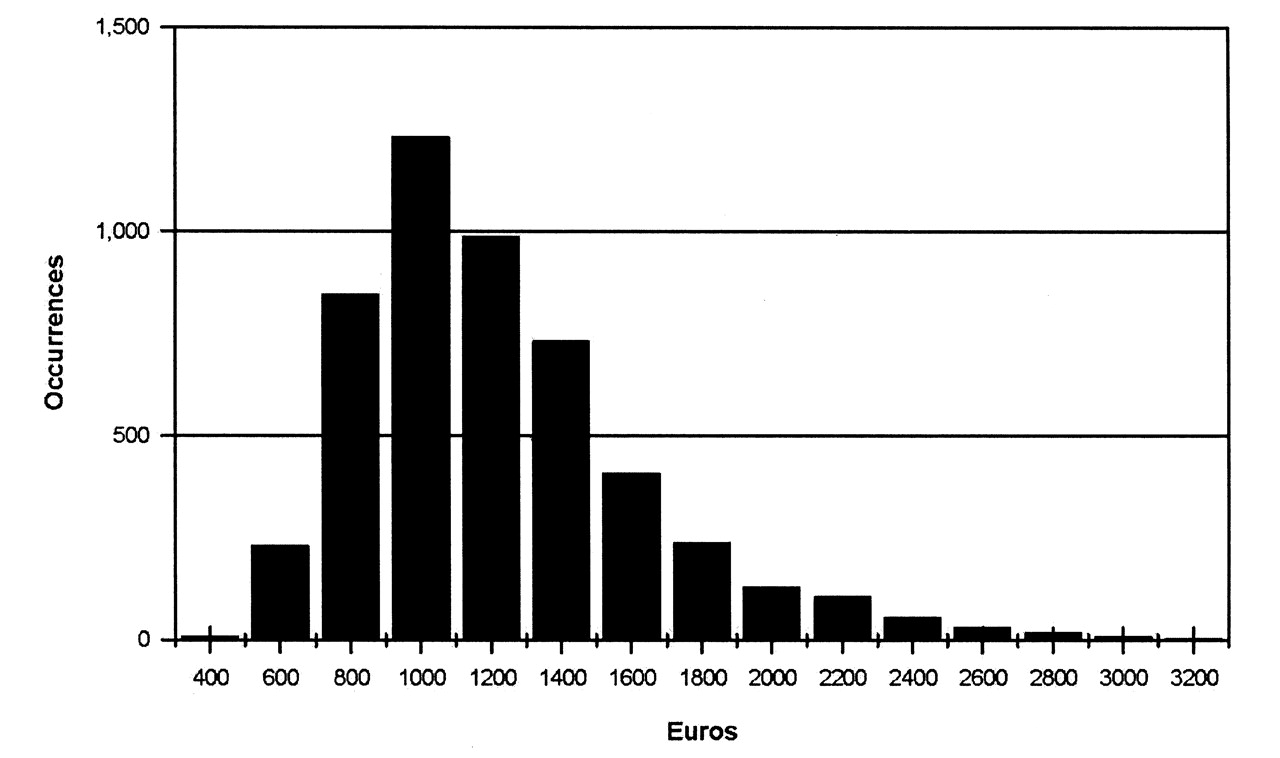
The computation of resource utilization items using 5000 Monte Carlo simulations generated the overall distributions of direct total medical costs (without drug costs) per disease activity level (Figures 1–5).
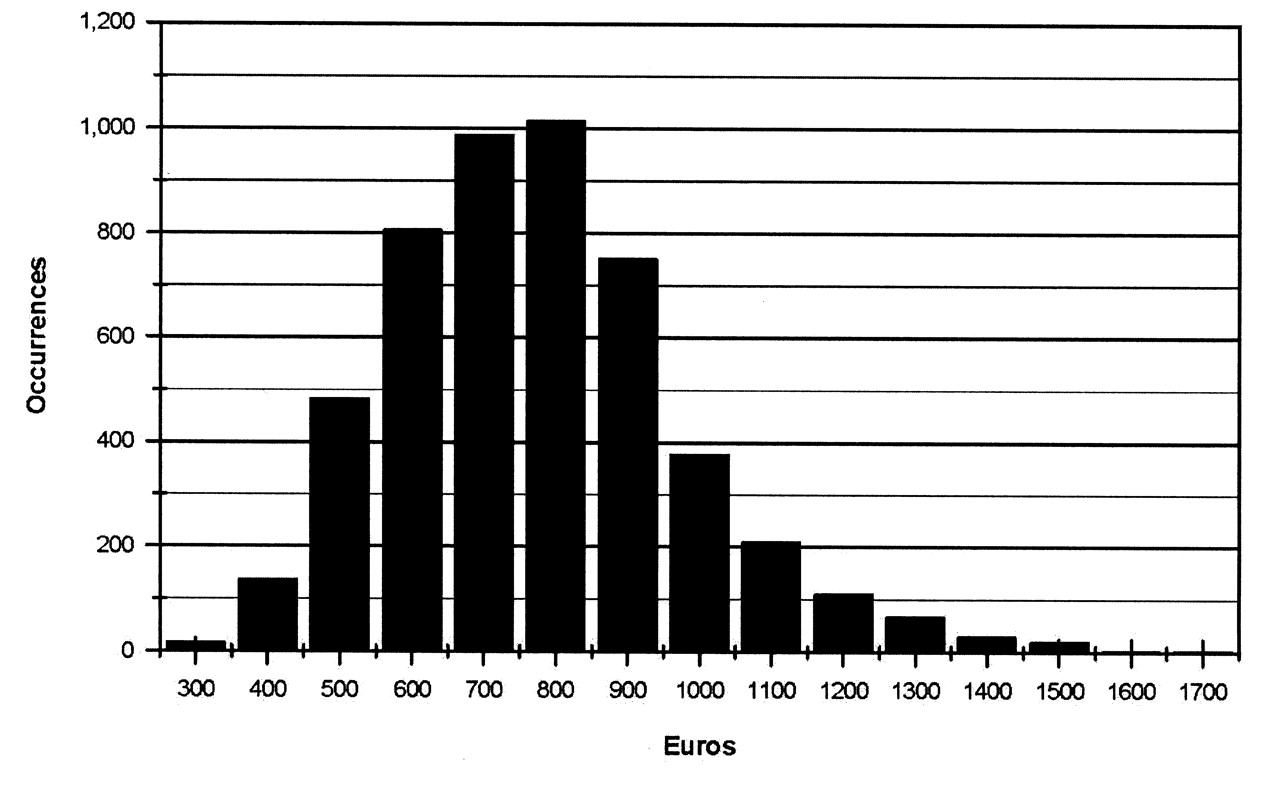
Direct medical costs of remission during the first 6-month period (in €).
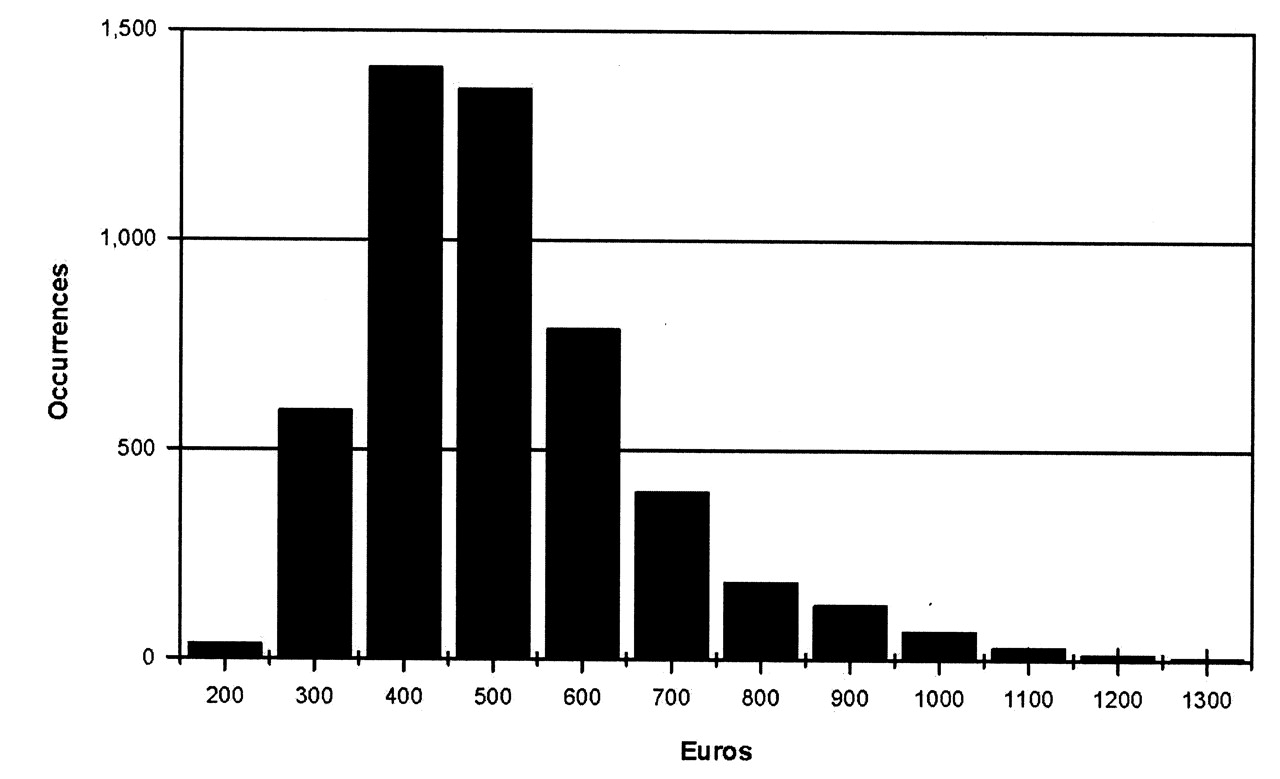
Direct medical costs of achieving remission during subsequent 6-month periods (in €).
Direct medical costs of achieving LDAS during the first 6-month period (in €).

Direct medical costs of achieving LDAS during subsequent 6-month periods (in €).

Direct medical costs of moderate to high disease activity (not achieving LDAS) over 6 months (in €).
For patients achieving remission, mean costs were estimated at €771 (SD 199) for the first 6 months and €511 (SD 162) for each subsequent 6-month period (p < 0.001). For patients not achieving remission, mean costs were estimated at €1159 per 6-month period (SD 339). For patients achieving LDAS, mean costs were estimated at €905 (SD 263) for the first 6 months and €696 (SD 240) for each subsequent 6-month period (p < 0.001). For patients in MHDAS, mean costs were estimated at €1215 per 6-month period (SD 405). Significant reasons for costs were medical visits, laboratory tests, and transportation.
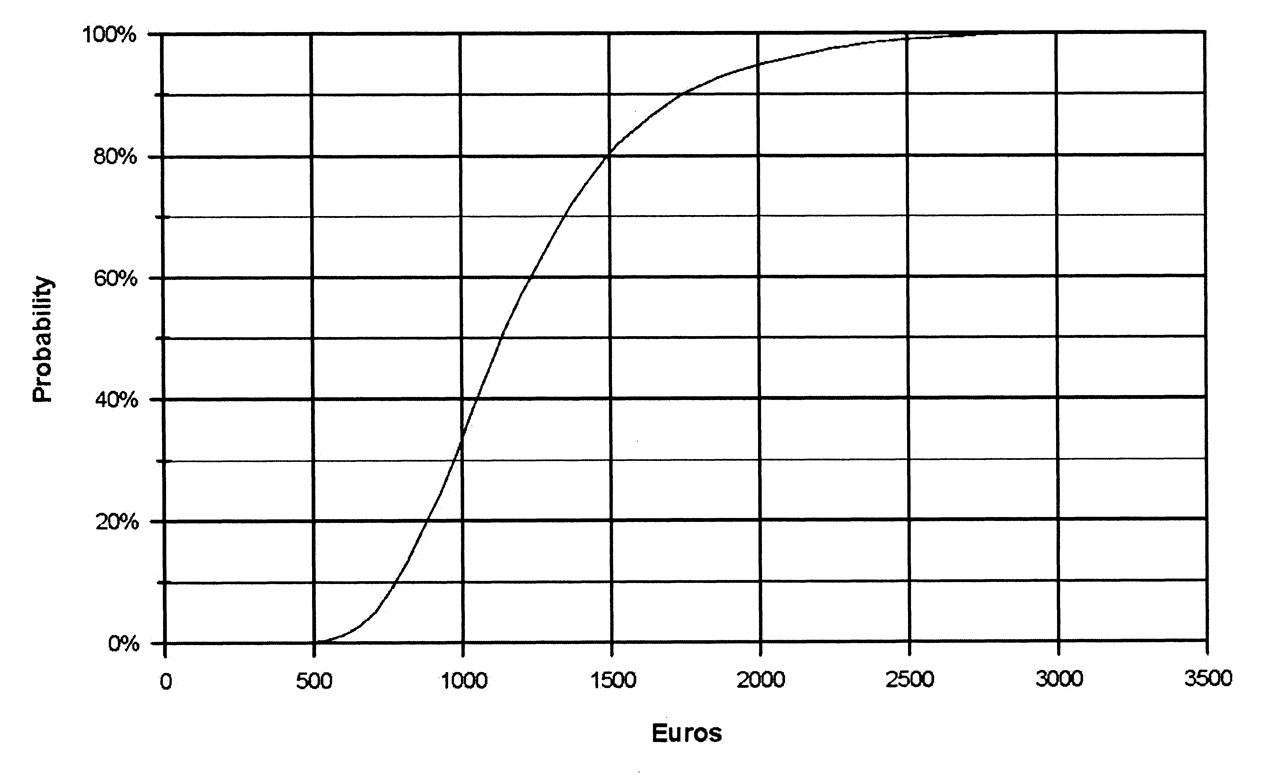
Our methodological approach using data from standard medical practices and simulation models allows construction of cumulative probabilistic curves such as the one given in Figure 6. For example, Figure 6 shows that approximately 80% of patients in MHDAS had associated direct costs less than €1500 over 6 months. One important result of Monte Carlo simulation models is generation of cumulative probabilistic curves, which are very informative when comparing cost distributions for heterogeneous patients versus presenting only mean costs.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Probabilistic cumulative costs of achieving moderate to high disease activity state over 6 months (in €).
DISCUSSION
The use of resource utilization questionnaires in a prospective descriptive study is a classic method to assess cost of illness. However, this approach would suggest analyzing a very large number of subjects in order to be as representative as possible for the overall patient population. On the other hand, for chronic diseases for which management is well established and is informed by specific treatment guidelines, such as for RA, using a standard costing approach represents another method for conducting cost-of-illness studies. In particular, the use of new biologic agents in RA has led to international and national medical consensus, treatment guidelines, and recommendations from scientific societies that are now commonly accepted in many countries, such as in France11.
The modeling approach is one attempt to achieve a systematic cost-of-illness analysis while circumscribing various problems inherent in purely descriptive cost-of-illness analyses. It establishes relevant but flexible evaluation criteria, including cost categories, and accounts for local medical practices and, importantly, for different levels of disease severity. In our analysis, we systematically clustered direct medical costs by disease severity category (remission, LDAS, and HDAS), an approach that allows estimation of costs more precisely for individual patients as well as the healthcare system as a whole.
Our study establishes that patients with high RA disease activity represent a significant economic burden to the health system compared to patients in the remission state or LDAS. From the payer’s perspective, this suggests that specific patient groups should be treated with the most effective therapeutic options in order to reduce costs. Some European studies found similar evidence14 of higher disease activity rates being associated with higher expenditures. Such an approach may result in significant reduction of RA severity in the long term and thus lower the burden of illness for the healthcare system. The original contribution of our study was to determine the distribution of direct medical costs by disease activity levels. Our results clearly established the positive relation between medical resources used and disease activity. During the first 6-month period patients were estimated to cost an average of €771 in the remission state, €905 in LDAS, and €1215 in the moderate to high disease activity state. These findings suggest that it is important to take into account the influence of direct medical resources used when assessing new therapeutic strategies14. Indirect costs are difficult to estimate consistently across studies and hence the proportion of direct and indirect costs in RA management varies significantly. For example, Guillemin and colleagues evaluated physicians’ data in 148 French hospitals and found that direct costs represented 59% of the total costs for patients with active RA, and 57% for patients with severe RA. Social costs represented 41% of the total costs on average15. A pan-European study found the proportion of direct versus indirect costs of RA to be 35% versus 65%, respectively1. A review article of 13 cost-of-illness studies in RA found the direct and indirect costs to be equal16, while other studies estimated indirect costs to be 2 to 3 times as high as direct costs2,6,17.
To date, there has been only one substantial effort to calculate direct and indirect costs of RA for the French healthcare system: a cross-sectional study among rheumatologists in 148 hospitals that resulted in data for direct and social RA costs for a 12-month period for 1109 patients with RA15. The direct annual cost per patient was estimated to exceed €4000 (with hospitalization costs contributing to 60% of the expenditures). The French context is informative because RA costs are reimbursed fully as soon as the diagnosis is confirmed, and the prevalence of the disease is estimated to be in the middle of the European range for RA (less than in northern Europe and more than in southern Europe).
Therefore, data generated by cost-of-illness models should be considered the first stage for further research on cost analyses for RA, such as large real-life prospective surveys using a resource utilization questionnaire that will address real-life medical practices. Regardless, medical resource utilization should be considered when evaluating the influence of new therapeutic regimens in RA8. However, real-life cost estimates have significant methodological and logistical limitations: they often focus on patients’ estimates of disease-related payments, which can be subject to memory errors14,18; they include an inventory of associated costs rather than direct cost estimates; or they deduce healthcare expenditures from hospital stays from a relatively limited sample15. In addition, the chronic course of RA results in different rates of expenditure at different periods of disease progression, and current cost-of-illness studies include cross-sectional rather than longitudinal data14.
Our results demonstrate that patients with high RA disease activity impose a substantial economic burden for the French healthcare system compared to patients in the remission state or LDAS, suggesting that these patient groups should be treated with the most effective drugs as early as possible, in an attempt to achieve remission or a state of low disease activity. By reducing the severity of the disease, its progression, and its important longterm medical and economic consequences, this approach would contribute to reducing the burden of RA on patients and on healthcare systems. Considering the overall economic influences on direct and indirect costs, this would also benefit society as a whole.
With the introduction of promising new biological drug therapies for RA, it is especially important to compare the financial burden of these new, expensive options to traditional regimens9. However, due to their relatively high costs compared to synthetic disease-modifying antirheumatic drugs, reimbursement authorities in Europe tend to restrict access to this class of drugs. As a comparison, the use of these drugs in the US is about 3 times higher than in Western Europe1. Evaluating how introduction of these effective but costly drugs may reduce the overall costs of RA may facilitate their widespread use. This is the advantage of cost-effectiveness modeling that allows comparison of new agents and complex therapeutic strategies. On the other hand, cost-of-illness studies are not drug-oriented but disease-oriented. Not only are cost-of-illness studies the foundation of sophisticated cost-effectiveness models, they also generate novel information about managing various patient categories within a given healthcare system.
Footnotes
-
Supported by an unrestricted grant from Bristol-Myers Squibb.
- Accepted for publication October 14, 2010.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.