

Neuropsychiatric systemic lupus erythematosus (NPSLE) is a serious and potentially life-threatening manifestation of SLE that occurs in 37%–95% of cases and is associated with an increased risk of death1. Cerebral atrophy (i.e., cortical atrophy and ventricular dilation) determined by magnetic resonance imaging (MRI) was prevalent in 18% of patients with newly diagnosed SLE and was the most frequent abnormal finding by MRI2. MRI was more sensitive than brain histopathology for the presence of cerebral atrophy in NPSLE3.
A 30-year-old woman with a 5-year history of SLE had a flare with fever and disturbed consciousness. The initial MRI scan with fluid-attenuated inversion-recovery revealed multiple high-intensity areas in the deep white matter (Figure 1A). Stroke and infection were excluded following investigation. Accordingly, we diagnosed an acute confusional state (delirium) caused by SLE. Despite aggressive treatment, including steroid pulse therapy and pulsed intravenous cyclophosphamide, the patient’s consciousness rapidly deteriorated into coma. Four months later, we noted significant cerebral atrophy, characterized by a loss of brain volume, along with multiple continuous high-intensity areas (Figure 1B). She never recovered from coma and was transferred to another hospital.
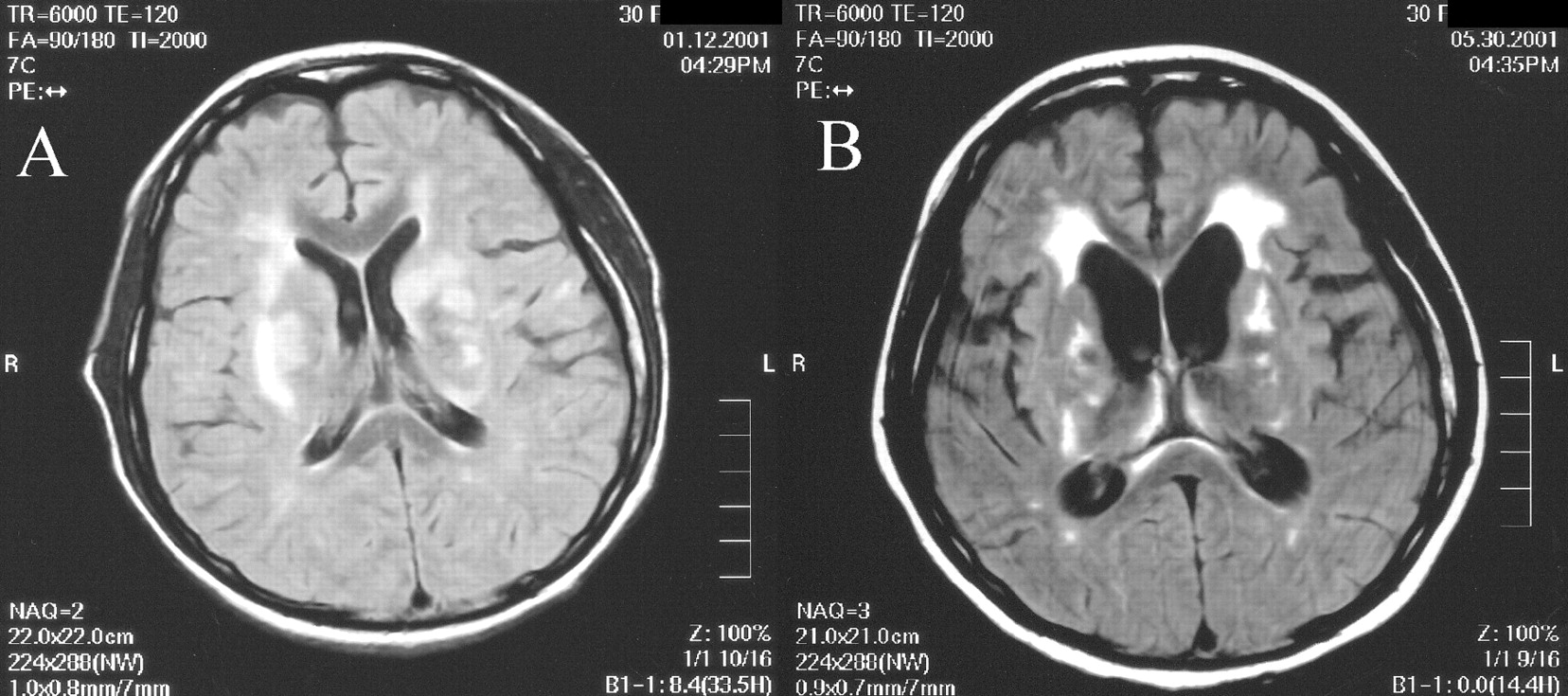
A. The initial MRI scan with fluid-attenuated inversion-recovery reveals multiple high-intensity areas in the deep white matter. B. Four months later, there is significant cerebral atrophy, characterized by a loss of brain volume, along with multiple continuous high-intensity areas.
Although mild brain atrophy on MRI is a common abnormal finding in NPSLE, rapidly progressing moderate to severe brain atrophy, as in this patient, has seldom been reported4. The MRI findings reflect the severe clinical outcome.
Footnotes
-
Supported by a grant from the Japanese Ministry of Health, Labor, and Welfare (Grant for Intractable Diseases).








{kind=link}