
Abstract
Objective. Since chronic kidney disease (CKD) is closely associated with cardiovascular disease and mortality as well as endstage renal disease, prediction of progressive CKD is a clinically important issue. We investigated the independent risk factors for the development of CKD in patients with lupus nephritis (LN).
Methods. The cohort included 322 Korean patients diagnosed with LN between 1985 and 2010. We retrospectively analyzed the clinical and laboratory indices, treatment response, the final renal function, and the biopsy findings. The timing and cumulative risk of developing CKD were identified by Kaplan-Meier methods. The independent risk factors for developing CKD were examined by univariate and multivariate Cox proportional hazards regression analyses.
Results. The median followup time after the diagnosis of LN was 84 months. CKD occurs in 22% of the patients within 10 years after the diagnosis of LN. The probability of developing CKD was significantly associated with the onset time of LN (delayed-onset LN vs initial-onset LN; HR 2.904, p = 0.003), deteriorated renal function [an estimated glomerular filtration rate (eGFR) < 60 ml/min/1.73 m2 body surface area] at the onset of LN (HR 7.458, p < 0.001), relapse of LN after achieving remission (HR 2.806, p = 0.029), and resistance to induction therapy (HR 8.120, p < 0.001).
Conclusion. Our results demonstrate that delayed-onset LN, a decreased eGFR at the time of LN onset, and the failure to achieve a sustained remission are predictors for the development of CKD in Korean patients with LN.
- CHRONIC KIDNEY DISEASE
- KOREA
- LUPUS NEPHRITIS
- RISK FACTORS
Systemic lupus erythematosus (SLE) is a chronic systemic autoimmune disease that is characterized by the production of diverse autoantibodies to components of the nucleus. It mainly affects women. Around 50%–80% of patients with SLE also have lupus nephritis (LN)1. Renal involvement, which is one of the most serious organ involvements, is clinically heterogeneous, but it is the strongest predictor of a poor outcome for patients with SLE. The study of LN has traditionally emphasized the occurrence of renal failure and the achievement of remission2,3,4, and less attention has been paid to the development of chronic kidney disease (CKD). CKD is recognized as a global public health problem, and CKD is associated with mortality and cardiovascular disease as well as the development of endstage renal disease (ESRD)5. As the renal function declines, uremic phenotypes including inflammation, insulin resistance, anemia, and endothelial dysfunction increase, although renal replacement therapies are not yet needed6.
Various kinds of drugs have recently emerged to control life-threatening disease flares such as LN. Since these efforts have contributed to improved survival of patients with SLE, identification of the risk factors for cardiovascular diseases such as CKD could improve clinical outcome in patients with SLE.
Various clinical and demographic factors have been reported to be associated with ESRD in patients with LN, such as the World Health Organization (WHO) class of nephritis, the presence of hypertension, treatment response, and the ethnicity of patients3,7. However, there are few studies to determine risk factors for development of CKD in patients with LN. Given that one of the major causes of death in patients with SLE is cardiovascular disease, predicting the risk factors for developing CKD in patients with LN is important.
We conducted a case-control study of 322 Korean patients with LN. We examined the cumulative incidence of CKD in patients with LN and their clinical and laboratory characteristics. Finally, we identified the independent predictors of developing CKD in Korean patients with LN.
MATERIALS AND METHODS
Subjects
Between January 1985 and December 2010, 438 patients with LN were identified from the SLE cohort at Seoul St. Mary’s Hospital, which is a tertiary care university hospital and referral center. All patients met the classification criteria for SLE as defined by the American College of Rheumatology (ACR)8. Subjects were excluded if they had < 6 months of followup after the diagnosis of LN, diabetes as a comorbid condition, or if they lacked clinical data. Patients who underwent quantitative examination for proteinuria at the onset of LN and whose results met the ACR renal disorder criteria9 were recruited. A total of 322 patients were enrolled. The study received approval by the Institutional Review Board of Seoul St. Mary’s Hospital (clinical trial no. KC11RISI0090).
Definition
CKD was defined according to the Kidney Disease: Improving Global Outcome definition [glomerular filtration rate (GFR) < 60 ml/min/1.73 m2 of body surface area for 3 months or more]10. The response criteria were defined according to the ACR 2006 clinical trial criteria11. Complete remission (CR) was defined as (1) normal GFR ≥ 90 ml/min/1.73 m2 or > 25% increase from baseline; (2) urine protein-to-creatinine ratio < 0.2 or a dipstick test of 0 to trace; (3) < 5 red blood cells/high power field (HPF); and (4) no cellular casts in the urine. Partial remission (PR) was defined as meeting the ACR 2006 clinical trial criteria for remission with the exception of a urine protein-to-creatinine ratio between 0.2 and 2. If patients met at least 2 measures but were missing information on the other criteria, then they were labeled as partial responders. Patients were defined as nonresponders if they failed to meet any of the criteria for remission. Disease relapse was characterized as a > 25% decline in the GFR, a 50% or more increase in proteinuria, or active urine sediment characterized by > 5 erythrocytes per HPF and/or cellular casts. Nephrotic proteinuria was defined as proteinuria > 3.5 g/24 h or a urinary protein:urinary creatinine ratio > 3. Hypertension (HTN) was defined as a supine systolic blood pressure (SBP) ≥ 140 mm Hg or a diastolic blood pressure (DBP) ≥ 90 mm Hg. Initial-onset LN (I-LN) was defined as LN diagnosed at the time of SLE onset. Delayed-onset LN (D-LN) was defined as newly developed LN after the onset of SLE.
Collection of clinical, laboratory, and histological data
Demographic and clinical data were obtained from the medical records, including sex, age at time of onset of SLE or LN, disease duration, and duration of followup after the onset of LN. The clinical data were the kind of treatment used as induction or maintenance therapy, body mass index (BMI) and blood pressure at the time of LN diagnosis, autoantibody profiles measured at the time of renal presentation [anti-dsDNA, antinuclear, antiribonucleoprotein (RNP), anti-Ro/La, and anticardiolipin antibodies, and lupus anticoagulants (LAC)], and biochemical measures [hemoglobin (Hb), presence or absence of thrombocytopenia (defined as < 100,000/mm3), serum creatinine, serum albumin, complement (C3, C4) levels, 24-h urinary protein excretion, absence or presence of hematuria (> 5 erythrocytes/HPF), and estimated GFR (eGFR)] at baseline, 6, and 12 months after the diagnosis of LN. The onset of SLE or LN was taken as the date at which the diagnosis of SLE or LN was made. GFR was calculated by the Modification of Diet in Renal Disease study equation:
Treatment regimen
This is a retrospective, observational study and consequently the therapeutic regimens were not standardized. Despite this limitation, data on the immunosuppressive regimen used for the induction and maintenance therapy of LN were available in the majority of cases. We also had access to information on cumulative cyclophosphamide (CYC) doses, renal remission rates, and/or the number of relapses experienced by patients during followup.
Statistical analysis
Statistical analysis was performed using SPSS statistical software (standard version 16.0; SPSS, Chicago, IL, USA). When comparing the 2 groups, the Mann-Whitney U test was used for continuous variables and the chi-squared test for categorical variables. Correlations between each variable were evaluated using Spearman’s correlation test. Cox’s proportional hazards model was used to estimate the hazard ratio and 95% CI was used to identify the predictive factors for the development of CKD. The variables with variance inflation factor > 10 were considered to have a multicollinearity problem. The starting date for these analyses was the date of diagnosing LN. The timing and cumulative risk of CKD development were studied by Kaplan-Meier methods and compared using the log-rank test. Results are reported as mean ± SD. All p values were 2-tailed and p values < 0.05 were considered significant.
RESULTS
Baseline demographic, clinical, and laboratory profiles
We identified 61 patients who developed CKD during followup from our 322 cohort patients. The median duration of followup was 84 months.
As shown in Table 1, there was no difference in the baseline demographic characteristics between the LN patients with progressive CKD and those with a preserved GFR. All study subjects were Korean. Disease duration at the time of LN onset was longer in patients who had progressed to CKD than in those with preserved renal function. Variables not associated with the development of CKD were BMI, newly developed HTN, presence of thrombocytopenia, positivity of 3 antibodies (for antinuclear, anti-La, and anti-dsDNA), C3 and C4 levels, presence of hematuria, and serum albumin level at LN onset. Although the incidence of newly diagnosed HTN was not different between the 2 groups, SBP and DBP at the time of LN onset were significantly higher in patients with CKD than in the non-CKD patients (p = 0.014 and p = 0.012, respectively). The proportion of patients with Hb ≤ 10 g/dl at baseline was greater for the patients with CKD. Our data show that anti-Ro antibody positivity was correlated with a better prognosis on the development of CKD. The same pattern was also present for anti-RNP antibody (p = 0.022). The proportions of LAC or anticardiolipin antibody positivity were not different between the groups (data not shown). Interestingly, the rate of I-LN was significantly higher in the non-CKD group compared to that of the CKD group (p = 0.011). Renal function at the time of LN onset, represented by serum creatinine and eGFR, were significantly decreased in patients with CKD (p < 0.001 and p < 0.001, respectively). The rate of nephrotic proteinuria was not different between the groups.
Clinical characteristics and renal functions measured at the onset of lupus nephritis. Values are mean ± SD and n (%).
Renal biopsy findings and clinicopathological correlation
Table 2 shows the histopathological comparison of our cohort patients. About 70% of all patients underwent renal biopsy and the portion of patients who underwent renal biopsy within 1 month after LN onset was not significantly different between the 2 groups. We failed to find any difference in the WHO classification between the 2 groups. Chronic tubulointerstitial changes, including tubular atrophy and interstitial fibrosis, were found more frequently in the patients with progressive CKD (p = 0.020 and p = 0.023, respectively). Glomerular sclerosis was found more frequently in patients with CKD than in patients with preserved renal function, although this was statistically insignificant (p = 0.108). Among the findings of crescent formation, cellular crescent was correlated only with the development of CKD (p = 0.011). The mean values of the AI and CI were higher in the group of patients with progressive CKD. Therefore we determined the relationship between the clinical measures at the onset of nephritis and the AI or CI, which were significantly different between the 2 groups.
Comparison of renal biopsy findings in 226 patients with lupus nephritis (LN). Values are mean ± SD and n (%).
To avoid the error of the time interval between onset of LN and renal biopsy, we used only the histological data obtained within 1 month after LN onset. After exclusion, 180 cases were finally included in the analysis. As shown in Table 3, significant correlations were found between the AI and serum creatinine, the eGFR, the serum albumin level, the SBP, the DBP, and the Hb level. Only serum creatinine, eGFR, and SBP were significantly correlated with the CI.
Clinicopathological correlation at the time of onset of lupus nephritis. All renal biopsies were performed within 1 month after onset. N = 180.
Renal response following induction and maintenance therapy
Table 4 shows the initial medications given as induction therapy for each group of patients. Most patients in both groups had been given CYC as induction and maintenance therapy. The majority of patients who progressed to CKD in the end had also been treated with CYC as primary induction treatment. Among the 181 patients with LN who had been treated with CYC as induction therapy, 45 (24.8%) eventually progressed to CKD during the followup period. Mean cumulative doses of CYC were not different between the 2 groups (9.4 vs 5.8 g in non-CKD and CKD, respectively; p = 0.217). Table 4 shows that the maintenance treatment regimens were not different between the groups either. According to the remission criteria, we classified the cohort patients into 4 groups by treatment response at 6 and 12 months following induction therapy. While about half the patients in the preserved GFR group reached CR and PR at 6 months, most patients (86.8%) with progressive CKD failed to achieve the remission criteria. The 12-month evaluation showed similar results (Table 4). Among patients who had ever met the CR criteria regardless of the period, we compared the time required to achieve the CR criteria between the groups. The period to reach CR was longer in the CKD group than that of the preserved GFR group (44.3 vs 22.0 months, respectively; p = 0.015). Because we could access the final renal outcome during followup, we could also analyze the final renal responses. A rate of sustained remission (CR and PR) until the time of the last followup was higher in the preserved GFR group than in the CKD group (55.5% and 18.3%, respectively). Of the patients with progressive CKD, 58.3% never achieved CR or PR during followup.
Differences in treatment strategy and treatment response in patients with lupus nephritis. Values are n (%).
Table 5 shows the difference of the clinical variables presented at 6 and 12 months following induction treatment. In light of a previous study13, which showed that the average decline in the GFR was normally 0.96 ml/min/yr or about 10 ml/min/decade, the relatively rapid decline of renal function in the patients who developed CKD was a clinically important finding. The mean values of the ΔeGFR at 6 months (defined as eGFR at 6 months – eGFR at LN onset) of the non-CKD and CKD groups were 9.6 and −4.3 ml/min/1.73 m2, respectively. Values calculated at 12 months were also significantly different between the 2 groups. These results suggest that the eGFR at 6 months and 12 months could be an easily obtained predictor of a poor renal outcome. Renal function of the patients with progressive CKD tended to decrease continuously for at least 1 year following induction therapy. By contrast, the eGFR of patients with preserved renal function showed an increasing pattern. As shown in Table 1, the baseline mean Hb level of patients with a preserved GFR was higher than that of patients with CKD (10.7 g/dl vs 9.6 g/dl, respectively). The difference of Hb level between the groups became larger (about 2 g/dl) at 6 months following induction treatment. The mean Hb level of both groups had increased, but to a lesser extent in the patients with CKD.
The difference in clinical measures representing treatment responses in patients with lupus nephritis. Values are mean ± SD.
Predictors of developing CKD in patients with LN
From our data, Kaplan-Meier methods demonstrated that CKD occurs in 22% of all patients within 10 years after diagnosis of LN. Univariate and multivariate Cox regression analyses were performed to assess the effects of variables on CKD development, in which the potential confounders (the features that differed between groups) were included (Table 6). Conditional stepwise analysis was used with adjustment for the effect of age and sex. There were statistically significant detrimental effects of the clinicopathological and laboratory features on development of CKD. On univariate analysis, various factors seemed to be risk factors for development of CKD. They included D-LN, the baseline SBP increment, a low Hb level at LN onset, impaired baseline renal function (eGFR at LN < 60 ml/min/1.73 m2), treatment resistance (estimated at 6 and 12 months), failure to sustain remission, a high histological index (the AI and CI), and chronic lesion on renal biopsies. On the other hand, the absences of anti-RNP and anti-Ro antibodies were not prognostic factors (HR 2.687, 95% CI 0.976–7.396, p = 0.056; and HR 1.917, 95% CI 0.839–4.380, p = 0.123, respectively). The variables of p < 0.05 in the univariate analysis were included in the multivariate models. Only 1 variable was selected among those involved in multicollinearity. We excluded the histological findings in multivariate analysis, because histological findings and renal function were found to have correlation in many studies14,15. On multivariate analysis, 3 factors remained significantly associated with the development of CKD: D-LN (HR 2.904, 95% CI 1.430–5.894), deteriorated renal function (eGFR < 60 ml/min/1.73 m2) at LN onset (HR 7.458, 95% CI 3.823–14.546), and failure to sustain remission (HR 2.806, 95% CI 1.109–7.098 for relapse; HR 8.120, 95% CI 3.508–18.796 for resistance to induction therapy). Figure 1 shows the cumulative incidence of developing CKD in patients with LN according to these 3 risk factors using Kaplan-Meier curves.


Proportion of patients who develop chronic kidney disease based on time of renal manifestation (A), renal function at onset of lupus nephritis (B), and treatment response (C). Log rank: (A) p = 0.004; (B) and (C) p < 0.001.
Univariate and multivariate Cox proportional hazards regression analyses of the predictors of chronic kidney disease in patients with lupus nephritis (LN), Conditional stepwise analysis adjusted for the effects of age and sex.
Mortality of the progressive CKD group
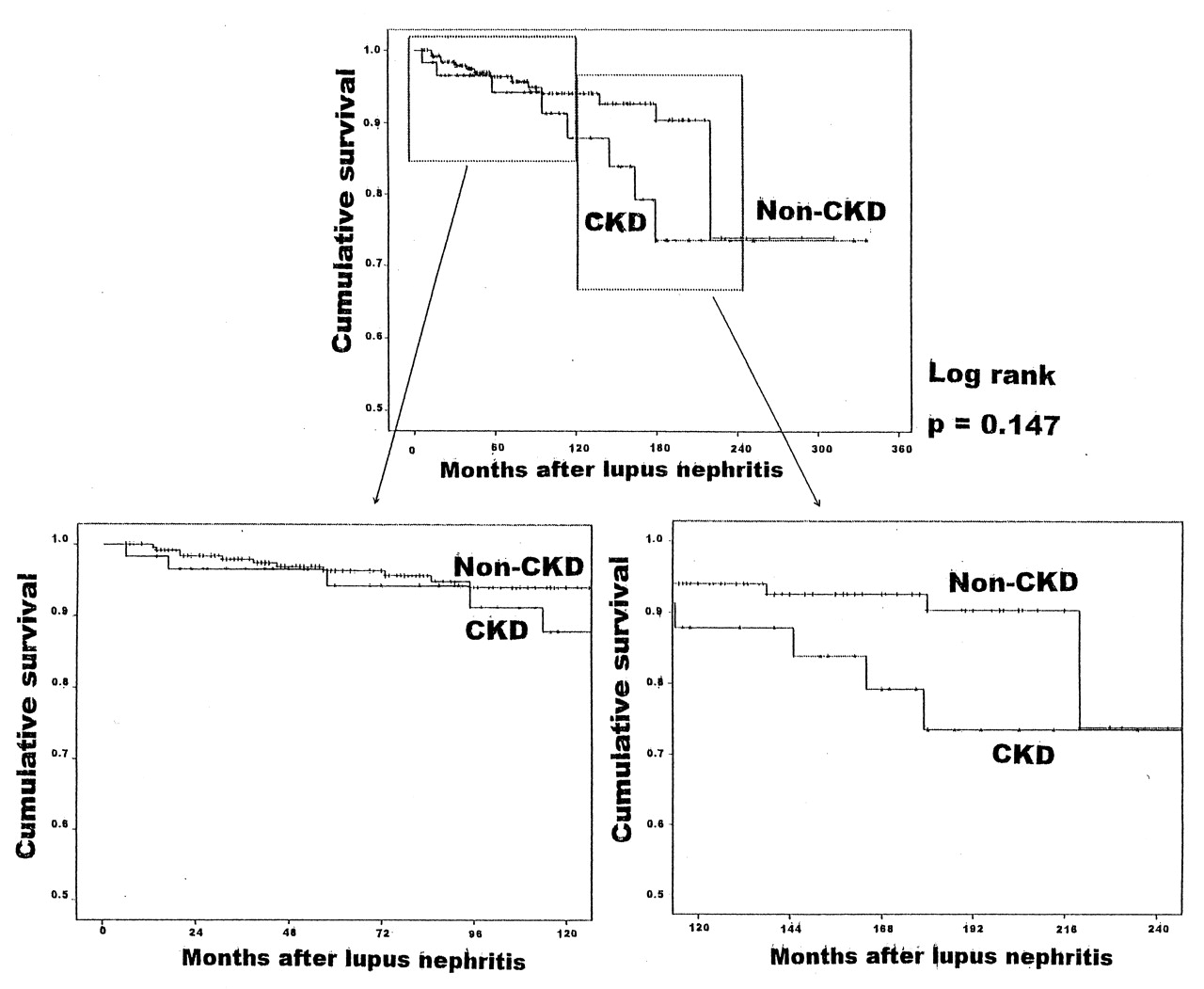
We found 23 cases of mortality during followup in our cohort: 15 cases from the non-CKD group and 8 from the CKD group. The majority of mortality (22 cases) resulted from noncardiovascular events. Only 1 patient died from heart failure of an unknown cause and the renal function of the patient was within the normal limits. Figure 2 shows the cumulative survival between groups. Although no difference was found between the groups as a whole (p = 0.147), it is interesting that the survival of patients with CKD seems to be lower starting from 10 years after the diagnosis of LN.
{kind=link}
{kind=link}
{kind=link}
Cumulative survival in patients with lupus nephritis according to the development of chronic kidney disease.
DISCUSSION
To our knowledge, this is the largest single-center, single ethnicity study that evaluated the predictors of developing CKD in patients with LN. In this cohort, we observed that a 22% cumulative incidence of CKD occurred within 10 years after onset of LN. We demonstrated that the onset time of nephritis (I-LN vs D-LN), deteriorated renal function (eGFR at the time of occurrence of nephritis < 60 ml/min/1.73 m2), and failure to sustain remission are the independent risk factors of developing CKD in patients with LN.
Although the WHO classification of LN is one factor used to determine prognosis16,17, this was not proven to be a critical factor in predicting development of CKD. Our results demonstrated that AI, CI, cellular crescent formation, and chronic tubulointerstitial changes were associated with the development of CKD in patients with LN, rather than the WHO classification. Previous studies also have reported the association of AI, CI, and chronic tubulointerstitial changes and the renal prognosis18,19,20 and treatment response21. We demonstrated that cellular crescents were correlated with the development of CKD (Table 2). This is not applicable to fibrous or fibrocellular crescents. In accord with our results, Austin, et al22 showed that the probability of doubling the serum creatinine was significantly associated with the histological presence of cellular crescents and that the cumulative probability of doubling the serum creatinine was about 70% at 90 months of followup.
As shown in Table 4, more patients with progressive CKD [49/58 (84.5%)] were administered a cytotoxic agent (CYC, mycophenolate mofetil) as induction therapy than those in the non-CKD group [164/257 (65.9%)]. These findings suggest that the response to induction therapy may be more important than the treatment regimen itself in light of the longterm renal function.
In our study, the time interval to renal manifestation after SLE onset was a strong predictive factor for development of CKD in patients with LN. We found that 28% of patients with D-LN progressed to CKD within 10 years after onset of LN. By contrast, CKD occurred in only 16% of patients with I-LN during the same period (data not shown). There has been only 1 report about the onset time of LN as a prognostic factor. Takahashi, et al23 reported that the response rate to therapy for LN was better in the I-LN group, although that study included a small number of patients. We demonstrated that D-LN is the independent risk factor for development of CKD, and it is worthy of further investigation.
Anti-Ro antibody, found in the sera from 30%–50% of patients with SLE, is also detected in patients with Sjögren’s syndrome, rheumatoid arthritis, and primary biliary cirrhosis. Previous reports have demonstrated that anti-Ro antibody was associated with subacute cutaneous lupus24, photosensitivity25, neonatal lupus heart block26, and valvular heart disease27. Actually, the effect of anti-Ro antibody positivity on renal manifestation in patients with SLE is not well known. One study28 showed that a lower anti-Ro antibody titer was correlated with occurrence of proteinuria in patients with SLE, and this suggests the effect of anti-Ro antibody on prevention of LN. It is interesting that the patients with a preserved GFR showed higher anti-Ro antibody positivity than those with CKD (Table 1). Only a few studies have been carried out to confirm the effect of anti-Ro antibody on the prognosis of renal function, and they have shown conflicting results. Contrary to our results, Korbet, et al demonstrated that presence of anti-Ro antibody was a poor prognostic factor of renal survival in severe LN29,30.
Anti-RNP antibody is considered to be highly sensitive for mixed connective tissue disease, but it is not specific. Although the role of anti-RNP antibody in the pathogenesis of SLE or LN has not been determined, our results show that anti-RNP antibody positivity and anti-Ro antibody positivity are correlated with a better prognosis of longterm renal function.
There were various causes of death in our study. In the non-CKD group, the causes were sepsis (3 patients), pulmonary hemorrhage (3), pneumonia (1), heart failure of unknown cause (1), thrombotic thrombocytopenic purpura (TTP; 2), neuropsychiatric lupus (2), intractable bleeding (2), and miliary pulmonary tuberculosis (1). In the CKD group, the causes of death were sepsis (4), intractable bleeding (1), TTP (1), pulmonary hemorrhage (1), and neuropsychiatric lupus (1). Because the number of deceased cases was limited, we were not able to determine the effect of CKD on cardiovascular mortality by comparing the 2 groups.
Our study was retrospective and based on medical chart reviews of the cohort cases. Therefore, the agreement of renal biopsy findings between different pathologists could not be guaranteed and treatment strategies were not standardized. Nevertheless, we included a large number of patients from a single center and we found several independent risk factors for developing CKD in patients with LN. Among them, recognition of D-LN as a risk factor for development of CKD is interesting and worth further study in other ethnic groups.
Our study showed that CKD occurred in 22% of Korean patients with LN within 10 years after the diagnosis of LN. Multivariate Cox regression analysis identified D-LN (nephritis manifested after SLE onset), baseline renal insufficiency (eGFR at LN onset < 60 ml/min/1.73 m2), and failure to sustain remission (relapse and resistance to induction therapy) as independent variables for the development of CKD, rather than the histological classification or the severity of proteinuria.
- Accepted for publication June 10, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.