

Abstract
Objective. To evaluate the performance of the Systemic Lupus Erythematosus (SLE) Responder Index (SRI) when the SLE Disease Activity Index 2000 (SLEDAI-2K) is substituted with SLEDAI-2K Responder Index-50 (SRI-50), a valid and reliable index of disease activity improvement. Also, to determine whether the SRI-50 will enhance the ability of SRI in detecting responders.
Methods. Our study was conducted on patients who attended the Lupus Clinic from September 2009 to September 2010. SLEDAI-2K, SRI-50, the British Isles Lupus Assessment Group measure, and the Physician’s Global Assessment were determined initially and at followup. SRI was determined at the followup visit according to its original definition using the SLEDAI-2K score and by substituting SLEDAI-2K with SRI-50.
Results. A total of 117 patients with SLEDAI-2K ≥ 4 at baseline were studied. Patients had 1 followup visit over a 3-month period. Twenty-nine percent of patients met the original definition of SRI and 35% of patients met the definition of SRI when SLEDAI-2K was substituted with SRI-50. The use of SRI-50 allowed determination of significant improvement in 7 additional patients. This improvement could not be discerned with the use of SLEDAI-2K as a component of SRI. At followup visits that showed improvement, SRI-50 scores decreased to a greater extent than SLEDAI-2K scores (p < 0.0001).
Conclusion. SRI-50 enhances the ability of SRI to identify patients with clinically important improvement in disease activity. SRI-50 was superior to SLEDAI-2K in detecting partial clinical improvement, ≥ 50%, between visits. These properties of the SRI-50 enable it to be used as an independent outcome measure of improvement or as a component of SRI in clinical trials.
- SYSTEMIC LUPUS ERYTHEMATOSUS DISEASE ACTIVITY INDEX 2000
- SRI-50
- SYSTEMIC LUPUS ERYTHEMATOSUS RESPONDER INDEX
- DISEASE ACTIVITY
- SYSTEMIC LUPUS ERYTHEMATOSUS
- OUTCOME MEASURES
With the advent of potential new therapies for systemic lupus erythematosus (SLE), there is a great need to refine the SLE Disease Activity Index 2000 (SLEDAI-2K) to be able to measure partial clinically important improvement, ≥ 50%, in disease activity in clinical trials. For this purpose the SLEDAI-2K Responder Index-50 (SRI-50) was developed in 20091. In 2010, the initial validation of SRI-50 was reported2. As a first effort toward validating SRI-50, we assessed its content validity, face validity, practical applicability including administration and scoring, and concurrent construct validity1,3. We studied 141 patients with SLE and showed that SRI-50 is a valid index that detects clinically significant improvements (≥ 50%) between visits in patients with SLE3. SRI-50 was able to measure improvement in both clinical disease manifestations and SLE-related laboratory abnormalities3. Further, SRI-50 detected partial improvement between visits in some patients who improved but in whom the SLEDAI-2K 30-day measure did not discern this improvement1,3,4,5,6. The SRI-50 Data Retrieval Form, developed and validated to standardize the documentation of the descriptors of SRI-50, ensures the optimal performance of SRI-503. More recently we have shown that SRI-50 has intrarater and interrater reliability and can be used by both rheumatologists and trainees, and performs equally well with rheumatologists familiar with the instrument and those not familiar with it7. To facilitate the introduction of SRI-50 for general use, an SRI-50 manual has been developed along with a dedicated Website for SRI-50, www.sri-50.com. The Website includes both training and examination modules that familiarize rheumatologists with the SRI-50 Definitions and the SRI-50 Data Retrieval Form and assess their success in mastering the instrument.
Evidence-based exploratory analysis of the B lymphocyte stimulating factor antagonist belimumab in a phase II SLE trial led to the development of a novel responder index for SLE, the SRI, able to define a clinically meaningful change in disease activity8,9. SRI is a composite outcome that incorporates the modification of SLEDAI that was developed for the Safety of Estrogens in Lupus Erythematosus: National Assessment trial (SELENA-SLEDAI), the British Isles Lupus Assessment Group (BILAG) activity index, and the Physician’s Global Assessment (PGA)6,10,11,12. As proposed by the authors of SRI, the SELENA-SLEDAI score was used to determine global improvement. The BILAG domain scores were used to ensure that no significant worsening in organ systems has occurred (no new “A” score or 2 new “B” scores). The PGA ensured that improvement in disease activity is not achieved at the expense of the patient’s overall condition8. The SRI was initially assessed in a subset of 321 serologically active patients in a phase II belimumab placebo-controlled clinical trial. In serologically active patients, the addition of belimumab to the standard of care therapy resulted in a statistically significant response in 46% of patients at Week 52 compared with 29% of the placebo patients8. More recently, a phase III study of the effect of belimumab used this novel 3-part outcome response measure and was able to show a statistically significant difference in response among patients taking the drug as compared to placebo13.
The purpose of our study was (1) to evaluate the performance of the SRI when the SLEDAI-2K is substituted with the SRI-50; and (2) to determine if the SRI-50 will enhance the ability of the SRI in detecting improvement in disease activity. We hypothesized that the substitution of SLEDAI-2K with SRI-50 in the SRI increases the ability to identify patients with clinically significant improvement3,7,8.
MATERIALS AND METHODS
Patient enrollment and selection
All patients attending the Lupus Clinic from September 2009 to September 2010 were enrolled in a prospective longitudinal study. All patients met the American College of Rheumatology classification criteria for SLE14. At each visit a complete history was taken including demographics, and a physical examination and laboratory tests were performed. Patients were studied who had active SLE at the baseline visit, with SLEDAI-2K 30 days ≥ 4, and had 1 followup visit 1–3 months later15.
Outcome measures
SLEDAI-2K is based on the presence of 24 descriptors in 9 organ systems over the patient’s past 30 days. The total score of SLEDAI-2K falls between 0 and 105, with higher scores representing increased disease activity4,5,6,15.
The SRI-50 comprises the same 24 descriptors, covering 9 organ systems, and reflects disease activity over the previous 30 days, as does SLEDAI-2K6. The SRI-50 data retrieval form standardizes the documentation of the descriptors and performed extremely well in all descriptors, which is especially relevant for multicenter studies that form the backbone of any therapeutic evaluation for SLE3. The SRI-50 score is evaluated at the followup visit and corresponds to the sum of each of the 24 descriptors’ scores found on the SRI-50 data retrieval form. The method of scoring is simple, cumulative, and intuitive, similar to the SLEDAI-2K. One of 3 situations can occur when a descriptor is present at the initial visit: (1) the descriptor has reached complete remission at followup and the score would be “0”; (2) the descriptor has not reached a minimum of 50% improvement at followup and the score would be identical to its corresponding SLEDAI-2K value; or (3) the descriptor has improved by ≥ 50% (according to the SRI-50 definition) but has not achieved complete remission, in which case the score is evaluated as half of the score that would be assigned for SLEDAI-2K. If a descriptor was not present at the initial visit, the value for SRI-50 at the followup visit will be the same as that for SLEDAI-2K. This process is repeated for each of the 24 descriptors. Finally the SRI-50 score at followup is evaluated as the sum of the 24 individual descriptors’ scores.
The revised BILAG index (BILAG 2004) has been developed from the original index, based on the principle of a physician’s intention to treat11,16. BILAG 2004 includes 9 systems. Based on physician’s intention to treat, the scoring of BILAG is categorized as follows: A = severe disease activity, B = moderate disease activity, C = mild disease activity, D = inactive disease but previously affected, and E = inactive with no previous involvement16. In BILAG 2004, index items that are improving are scored less severely than those that are new, worse, or the same. BILAG scores in this study were generated with the British Lupus Integrated Prospective System17.
During the baseline and followup visit, a PGA was determined on a visual analog scale (VAS) line of 100 mm, with anchors of 0 (no disease activity) and 10 (very active disease). Any increase on PGA from baseline was considered clinically significant worsening. Patients with worsening on PGA from baseline were defined as nonresponders to the SRI.
Patient assessment
At the baseline visit, SLEDAI-2K 30 days and BILAG scores were determined and the SRI-50 data retrieval form was completed11,15,16.
At the followup visit at 1–3 months, the SRI-50 data retrieval form was completed, and SLEDAI-2K and SRI-50 scores were determined3. BILAG scores and PGA were determined.
Patients were treated with standard of care as determined by the treating rheumatologist.
Study design
SRI was determined at the followup visit according to the original definition using SLEDAI-2K score8. SRI was defined as (1) ≥ 4-point reduction in SLEDAI-2K score, (2) no new BILAG A or no > 1 new BILAG B domain score, and (3) no deterioration from baseline in the PGA.
The SLE Responder Index was further evaluated in the same group of patients, but this time substituting SLEDAI-2K with SRI-503. Patients who showed worsening in disease activity on the followup visit (an increase in the SLEDAI-2K score) were excluded from the analysis.
Statistical analysis
Descriptive statistics were used for the characteristics of the patients and the results of the analysis (proportions and percentages). We determined the number of responders who met the SRI on the followup visit using SLEDAI-2K and SRI-50. We determined the mean change of SLEDAI-2K scores among all patients [Δ SLEDAI-2K = SLEDAI-2K (baseline to followup)] and the mean change of SRI-50 scores [Δ SRI-50 = SLEDAI-2K (baseline) to SRI-50 (followup)]. The paired t test was used to compare the mean Δ SLEDAI-2K and the mean Δ SRI-50 scores.
RESULTS
Patient demographics
One hundred seventeen patients had baseline SLEDAI-2K ≥ 4 and a followup visit and were studied further. The patient profiles included 106 (90.6%) women and 11 (9.4%) men. Fifty-five percent were white, 19% black, 10% Asian, and 16% others. The age at baseline visit was 42.0 ± 14.0 years and disease duration at baseline was 13.0 ± 10.1 years. The time from baseline to followup visits was 3.0 ± 1.2 months (Table 1).
Characteristics of the patients.
Disease activity results
Mean SLEDAI-2K scores were 8.02 ± 4.53 at baseline visit and 5.82 ± 4.50 at followup visit, while mean SRI-50 scores were lower at 5.10 ± 3.95 at followup (p < 0.0001). The mean change of SLEDAI-2K scores (Δ SLEDAI-2K) among all patients was −2.20 ± 2.87 and the mean change of SRI-50 scores (Δ SRI-50) was −2.91 ± 3.03. The mean change Δ SLEDAI-2K and the mean change Δ SRI-50 scores at followup visits were statistically significantly different (p < 0.0001; Table 2 and Figure 1).
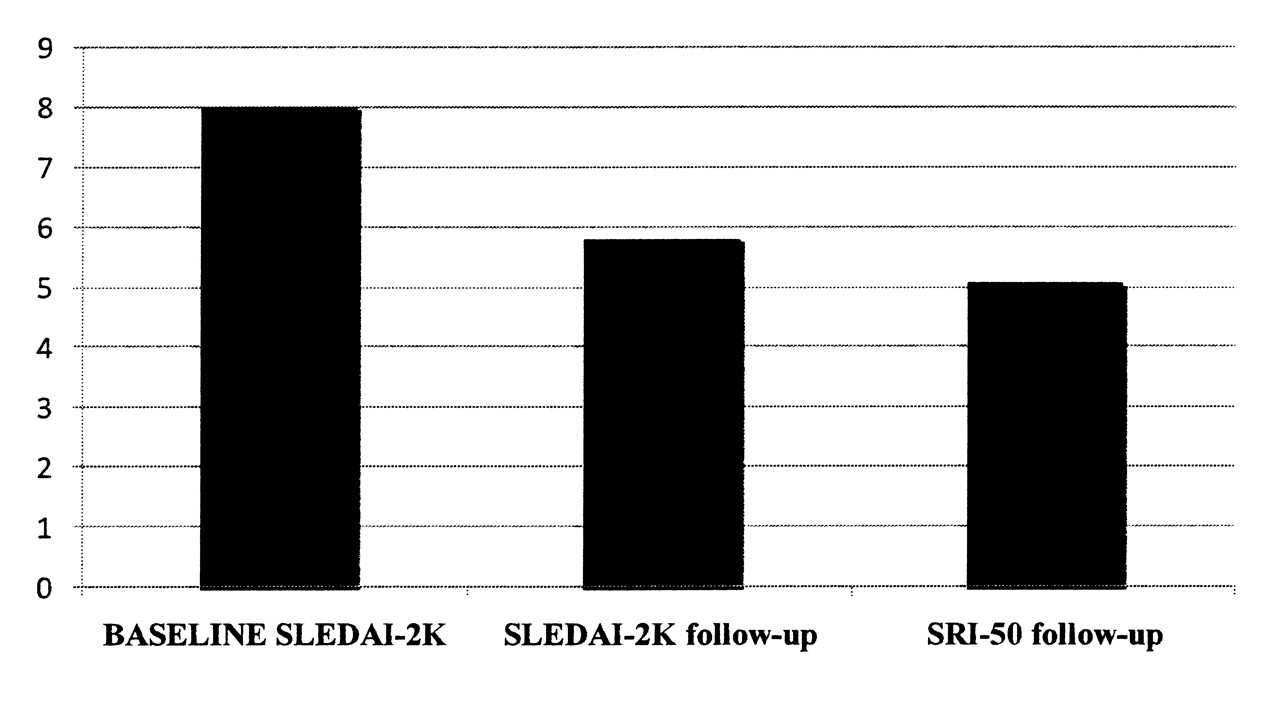
Disease activity scores at baseline and followup. SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; SRI: SLE Responder Index.
Disease activity results.
Thirty-four patients (29%) met the original definition of SRI. Forty-one patients (35%) met the definition of SLE Responder Index when SLEDAI-2K was substituted with SRI-50 score (Figure 2). The use of SRI-50 definitions allowed determination of a clinically significant improvement in 7 additional patients (Table 2 and Figure 2).

Percentage of patients who met SLE Responder Index definition. SLEDAI: Systemic Lupus Erythematosus Disease Activity Index; SRI: SLE Responder Index.
DISCUSSION
In light of the complexity and heterogeneity of SLE manifestations, it has become clear that a reliable, valid responder index is required to accurately detect and verify the efficacy of new therapeutic strategies in clinical trials. We have recently described the development and validation of SRI-503. The newly developed SRI-50 is a reliable and valid index to reflect partial important improvement (≥ 50%) in disease activity between visits in response to treatment.
We compared the performance of SRI on 117 patients with active disease treated with standard of care and followed up after 3 months. The advantage of using SRI-50 instead of SLEDAI-2K as a component of SRI was demonstrated by increasing the percentage of responders from 29% to 35%. This degree of improvement could not be discerned with the use of SLEDAI-2K as a component of SRI. In our previous study, we used SRI-50 in 141 patients and showed that the decrease in SRI-50 scores was clinically significant, meeting the accepted definition of improvement of a decrease in SLEDAI-2K of ≥ 4. This improvement was not achieved with SLEDAI-2K scores on followup visits3. Indeed, this reflected the ability of SRI-50 to detect partial and important improvement between visits in patients who improved, while the SLEDAI-2K did not discern this improvement. In our current study, we showed that on followup visits, SRI-50 scores in studied patients decreased to a greater extent compared to SLEDAI-2K scores, and this was statistically significant (p < 0.0001). This difference between SRI-50 and SLEDAI-2K scores resulted from the ability of SRI-50 to pick up partial improvement in the descriptors that meet the SRI-50 definitions of improvement. The results of the previous and current studies encourage the use of SRI-50 as an independent outcome measure of disease activity improvement in current trials3.
It is important to note that the original SLE Responder Index used in the belimumab trials required for response “no more than 0.3 units increase in the PGA using the point scoring on the SELENA-SLEDAI PGA.” In our study no worsening was allowed in the PGA using the VAS of 100 mm. The SELENA trial proposed a new modification of SLEDAI. In the SELENA-SLEDAI, several descriptors were modified in particular: visual disturbance, pleurisy and pericarditis, arthritis, and others. For instance, SLEDAI and its new version SLEDAI-2K mandate the presence of subjective (pleuritic or pericardial pain) and objective (rub, effusion, electrocardiogram or echocardiogram confirmation, or pleural thickening) findings for pleurisy and pericarditis to be scored as present. In the SELENA-SLEDAI, researchers accepted the presence of either the objective or subjective findings to score the descriptor as present. Despite the modifications in some of the descriptors, SELENA-SLEDAI acts similarly to SLEDAI-2K. It is important to highlight that there has been no validation of all of the modifications introduced in SELENA-SLEDAI. Thus the SELENA-SLEDAI version lacks the stringent validation steps that are essential before a measure can be used in clinical trials or research settings. SLEDAI-2K was validated against SLEDAI using the entire cohort of the University of Toronto Lupus Clinic. In our research center we have used the SLEDAI-2K and not the SELENA-SLEDAI. We have also used SLEDAI-2K to assess the patients in our current study. Thus the first component of the SRI was determined using SLEDAI-2K. The modification of PGA and SELENA-SLEDAI in the SRI definition would be unlikely to change the outcome of our study. Nevertheless, it does require clarification that this protocol is not identical to the original PGA component and SLEDAI component of the SRI and should be referred to as a modified SRI.
Retrospective application of the SRI to data from a phase II randomized controlled trial of belimumab in patients with active SLE demonstrated that belimumab treatment resulted in a statistically larger percentage of responders than treatment with placebo8. More recently, SRI was used as the primary outcome measure in a multicenter phase 3 study at Week 52. The results showed that belimumab with standard of care resulted in a significantly higher response rate than did placebo with standard of care at Week 52. Belimumab 10 mg/kg resulted in a significantly greater response than did placebo in all 3 SRI components, while belimumab 1 mg/kg resulted in a greater response than did placebo in 2 components (SELENA-SLEDAI and PGA)13. It is likely that the percentage of responders in this trial would have been higher and still be clinically significant had SRI-50 been used rather than SELENA-SLEDAI.
The results of our study showed that SRI-50 detects partial but clinically important improvement (≥ 50%) in disease activity between visits in response to treatment. The substitution of SRI-50 for SLEDAI-2K in the SRI increases its ability to identify responders. This validation of the SRI-50 enables it to be used as an outcome measure in clinical trials.
Footnotes
-
The Lupus Clinic is supported by The Lupus Flare Foundation, the Arthritis and Autoimmune Centre Foundation, and the Toronto General-Toronto Western Hospital Foundation Smythe Foundation. Dr. Touma is a recipient of the Lupus Ontario Geoff Carr Fellowship and the University of Toronto Arthritis Centre of Excellence Fellowship.
- Accepted for publication June 16, 2011.








{kind=link}
{kind=link}