

Abstract
Objective. In a cohort of systemic lupus erythematosus (SLE) patients with endstage renal failure, to evaluate whether continuing rheumatology followup visits and immunosuppressive therapy after starting renal replacement were associated with increased survival.
Methods. We identified all SLE patients over 21 years old who started renal replacement therapy between 2005 and 2011 at an urban tertiary care center. Mortality data were obtained using in-hospital records and the US Social Security Death Index database.
Results. We identified 80 SLE patients undergoing renal replacement therapy. Twenty-two patients (28%) were followed in rheumatology clinics frequently (2 or more visits per year) after starting renal replacement therapy, and 58 patients (72%) were followed infrequently (fewer than 2 visits per year). Survival rates were significantly higher in transplant patients compared with dialysis patients. Patients with SLE followed frequently after starting dialysis had significantly higher 4-year survival rates compared with patients followed infrequently after starting dialysis (log-rank p = 0.03). In the Cox proportional hazards model, treatment with prednisone alone or with no medication was associated with a hazard ratio (HR) of death = 6.1 (95% CI 1.1, 34; p = 0.04) and HR = 13 (95% CI 1.5, 106; p = 0.02), respectively, compared with patients treated with a combination of immunosuppressive therapy with or without prednisone, adjusted for age at SLE diagnosis, sex, transplant status, and the frequency of rheumatology visits after the development of endstage renal failure.
Conclusion. Active disease in patients with SLE undergoing renal replacement therapy may be underrecognized and undertreated, leading to increased mortality.
Renal disease associated with systemic lupus erythematosus (SLE) is one of the leading causes of morbidity and mortality in these patients1,2,3, with 20% to 30% of patients with lupus nephritis progressing to endstage renal failure (ESRF) over time4. Although the availability of renal replacement therapy (RRT), including dialysis and kidney transplant, has improved the overall survival of SLE patients with ESRF, mortality rates remain high and essentially unchanged over time5,6,7. Therefore, it is important to identify modifiable risk factors for unfavorable outcomes in patients with SLE who are undergoing RRT3. While several studies have compared mortality rates in SLE-related ESRF and non-SLE-related ESRF, factors associated with mortality in SLE patients with ESRF on RRT have not been well studied8,9,10,11,12. Further, it is not known whether improved survival in renal transplant patients with SLE compared with dialysis patients with SLE is due in part to better control of SLE disease activity by immunosuppressive therapy.
Studies have shown that SLE becomes inactive once ESRF develops and patients are started on RRT5,13,14. As their disease is believed to be clinically quiescent, these patients are maintained on fewer immunosuppressive medications13 and are less likely to visit their rheumatologists. Thus, it is possible that these patients may be underrepresented in observational cohort studies reported in the rheumatology literature. More recent studies, however, have suggested that SLE can indeed remain active after starting dialysis, especially in the first few years, and even after kidney transplant15,16,17,18,19,20. Thus, underrecognition and undertreatment of active SLE in these patients may be contributing to higher rates of complications and mortality.
The objectives of our study were to evaluate whether continued monitoring by rheumatologists, and/or the use of immunosuppressive treatments after starting RRT, are associated with improved survival among SLE patients with ESRF.
MATERIALS AND METHODS
Patients
We identified all patients over 21 years of age with International Classification of Diseases, 9th ed, diagnoses of SLE (710.0, 695.4) and at least 1 of the following conditions: chronic kidney disease stage V (585.5); endstage renal disease (585.6); complications of kidney transplant (996.81); kidney transplant status (V42); encounter for dialysis (V56); or admit for renal dialysis (V56.0). Patients were followed between January 2006 and February 2011 at Montefiore Medical Center (MMC), the university hospital for the Albert Einstein College of Medicine, a large urban tertiary care center in Bronx, NY. Patients were identified in the Montefiore electronic record system using Clinical Looking Glass, a software application developed at MMC, which allows clinicians and researchers to identify populations of interest, laboratory data, medications, and demographics from the MMC database21.
Because of the retrospective design of the study, we did not obtain informed consent from the patients, as no identifying information was stored or used in the data analysis. This project was approved by the Institutional Review Board at Albert Einstein College of Medicine/Montefiore Medical Center.
All electronic charts were reviewed by at least 2 physicians, neither of whom was aware of the outcomes prior to reviewing the charts. Although all the charts were reviewed for American College of Rheumatology (ACR) criteria, due to the retrospective design of the study the diagnosis of SLE was established based on the physician’s assessment documented in the charts. We were unable to establish the exact day/month of SLE diagnosis and onset of ESRF, and we therefore used the year of SLE diagnosis and ESRF onset in our time-dependent analysis.
The number of rheumatology visits post-ESRF was categorized as 2 or more visits per year (“frequent”) or fewer than 2 visits per year (“infrequent”). Time to event was defined as the number of years from the onset of ESRF to the last followup date or to the date of death.
Immunosuppressive therapy included at least 1 of the following: azathioprine, mycophenolate mofetil, tacrolimus, rituximab, or intravenous immunoglobulin (IVIG). Prednisone (Pred) and hydroxychloroquine (HCQ) use was entered and analyzed as separate variables. All patients were receiving a daily dose of prednisone ≤ 10 mg, the most common daily dose being 5 mg. Medication categories were as follows: no medications; Pred alone; Pred and HCQ in combination; and immunosuppressive medications with or without Pred or HCQ.
Data analysis
Statistical analysis was performed using Stata 10.0 software (StataCorp LP, College Station, TX, USA). We used the Student t test (or its nonparametric alternative, the Wilcoxon rank-sum test) and the chi-square test to evaluate bivariate relationships between continuous and categorical variables, respectively, in the “frequent” followup and “infrequent” followup groups.
We used Kaplan-Meier survival analysis and Cox proportional hazards models to evaluate all-cause mortality from the time of ESRF onset to the time of death or last followup at MMC.
RESULTS
Of the 134 patients identified, 54 were excluded from the final analysis for the following reasons: never started RRT (n = 2), intermittent dialysis only (n = 1), antineutrophil cytoplasmic autoantibody-positive crescentic glomerulonephritis (n = 2), mixed connective tissue disease (n = 2), sarcoidosis (n = 1), rheumatoid arthritis (n = 3), and “rule out SLE” (n = 43).
Based on our chart review, of the 80 patients included in the analysis, we found unequivocal evidence that 46 met at least 4 SLE criteria22, 8 met fewer than 4 SLE criteria but had a documented biopsy consistent with lupus nephritis, 4 met 3 criteria for SLE, 10 met 2 criteria, 5 met 1 criterion, and 7 had no information available. Therefore, 58 patients had probable or definite SLE. Twenty-two did not have complete information in the available records to confirm SLE by the ACR criteria. However, the diagnosis of SLE was clearly documented in all patients.
The baseline characteristics of the 80 patients included in the analysis are summarized in Table 1. Of these patients, 70 (88%) were women, and 45 (63%) were African American. The median age at SLE onset was 27 years [interquartile range (IQR) 19, 37], the median time between diagnosis of SLE and ESRF was 5 years (IQR 1, 10), and the median time between starting RRT and the last followup was 5 years (IQR 3, 9).
Baseline characteristics of the study patients. Continuous variables are reported as median (interquartile range).
Fifteen patients (19%) died of various causes during followup, including sepsis/probable sepsis (n = 5), seizures/status epilepticus (n = 2), subarachnoid hemorrhage (n = 1), pulmonary embolism (n = 1), colon cancer (n = 1), hyper-tension (n = 1), peritonitis (n = 1), and unknown (n = 3). SLE and/or ESRF (most likely related to lupus nephritis) were listed as a secondary cause of death for 8/15 (53%) deaths. Thirty-four (43%) received at least 1 renal transplant, 7/34 (21%) failed at least 1 renal transplant, and 2/34 (6%) had a documented recurrence of lupus nephritis.
Among 80 patients with ESRF/SLE on RRT, 58 (63%) visited rheumatologists at MMC less than twice a year post-ESRF (“infrequent” group), and 22 (28%) visited the rheumatology practice at MMC 2 or more times per year post-ESRF (“frequent” group). The mean number of visits in the “infrequent” group was 0.18 per year, with over 75% of patients not followed by rheumatologists. The mean number of visits in the “frequent group” was 4.3 visits per year (median 3.7, IQR 2.3, 5.5). Twenty-seven patients (47%) in the “infrequent” group and 9 (41%) in the “frequent” group (p = 0.65) were receiving immunosuppressive medications. There were 26 (45%) renal transplants in the “infrequent” group and 8 (36%) in the “frequent” group (p = 0.49). The 2 groups were similar in terms of race, ethnicity, sex, age at SLE onset, and duration from ESRF to last followup.
There were several notable differences between patients followed frequently compared to patients followed infrequently by rheumatologists after starting RRT. In the “frequent” followup group post-ESRF, 11/22 (50%) visited the rheumatology clinic more than once a year prior to developing ESRF, compared with only 12/58 (21%) in the “infrequent” followup group post-ESRF (p = 0.01). Further, the median duration between onset of SLE and onset of ESRF was 6 years (IQR 2, 10) in the “infrequent” group, and 2 years (IQR 1, 7) in the “frequent” group (p = 0.21). Although we did not have sufficient information about pre-ESRF disease activity for patients who were not followed by rheumatologists at MMC, the observations above suggest that patients in the “frequent” group may actually have had more rapidly progressive disease than patients in the “infrequent” group prior to developing ESRF.
The “infrequent” and “frequent” followup groups post-ESRF were also significantly different with respect to medication use while undergoing RRT: 13 (22%) in the “infrequent” group were not receiving any medications, compared with only 1 (5%) in the “frequent” group (p = 0.02). Only 13 (22%) patients in the “infrequent” group were taking HCQ compared with 12 (55%) in the “frequent” group (p = 0.006).
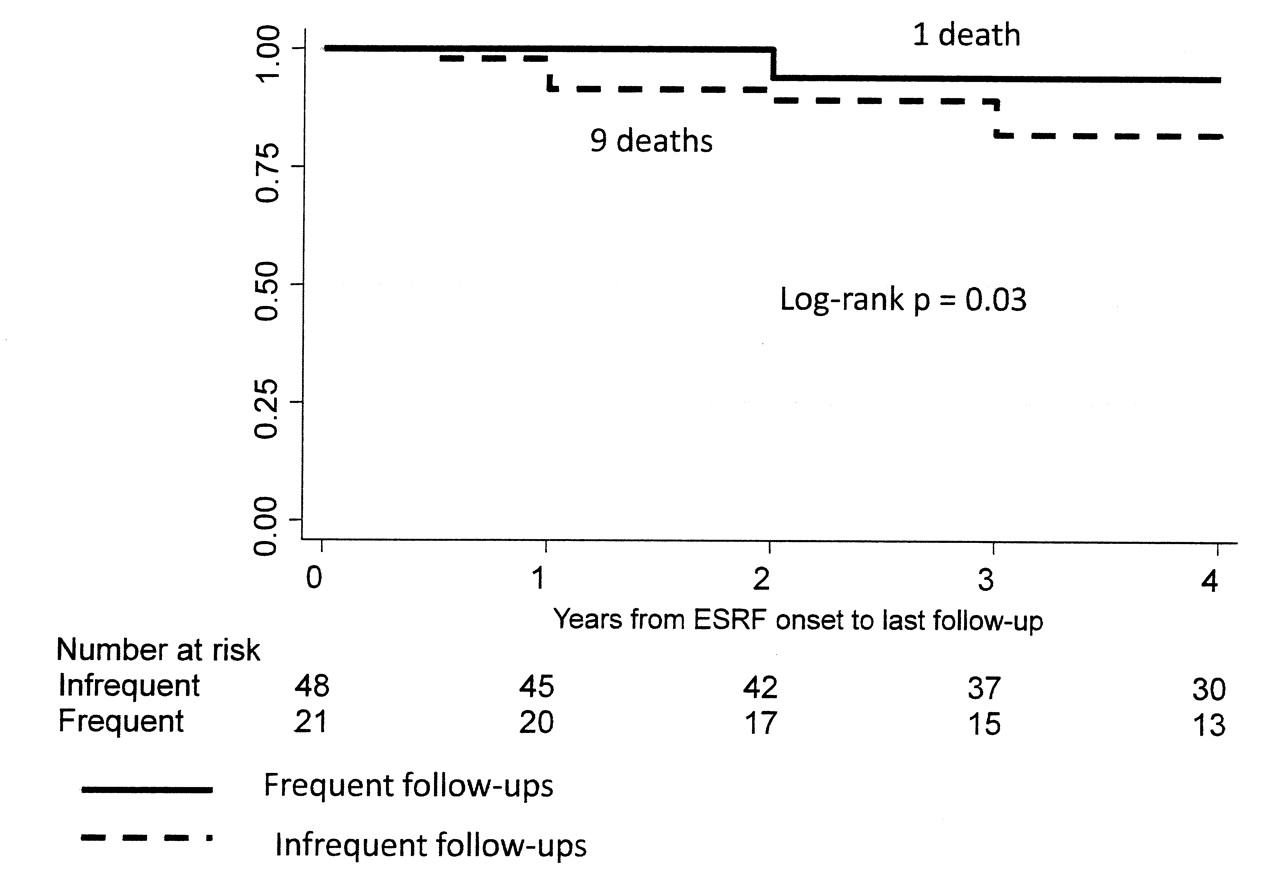
The results of Kaplan-Meier survival analysis are shown in Figures 1 to 6. We were not able to determine conclusively the time of ESRF onset for 11/80 patients. Therefore, 69 patients were included in survival analysis. Patients with SLE who were followed frequently after starting dialysis had significantly higher 4-year survival rates compared with patients followed infrequently after starting dialysis (log-rank p = 0.03; Figure 1). There was a similar trend for the 5-year survival (log-rank p = 0.12) and 10-year survival (log-rank p = 0.14), but these p values did not reach statistical significance because of a relatively small group size and a relatively small number of outcomes. Since transplanted patients with SLE had much higher survival from ESRF onset, compared with SLE patients undergoing dialysis (Figure 2), we performed survival analysis for the subgroup of 40 nontransplanted patients (Figure 3). The results were similar to the results for the entire cohort, with significantly higher 4-year survival rates among nontransplanted patients with SLE who were followed frequently after starting dialysis (log-rank p = 0.03). Again, there was a similar trend for the 5-year and 10-year survival among nontransplanted patients (log-rank p = 0.09 and log-rank p = 0.18, respectively).

4-year Kaplan-Meier survival among patients with SLE stratified by the frequency of rheumatology followup after ESRF.
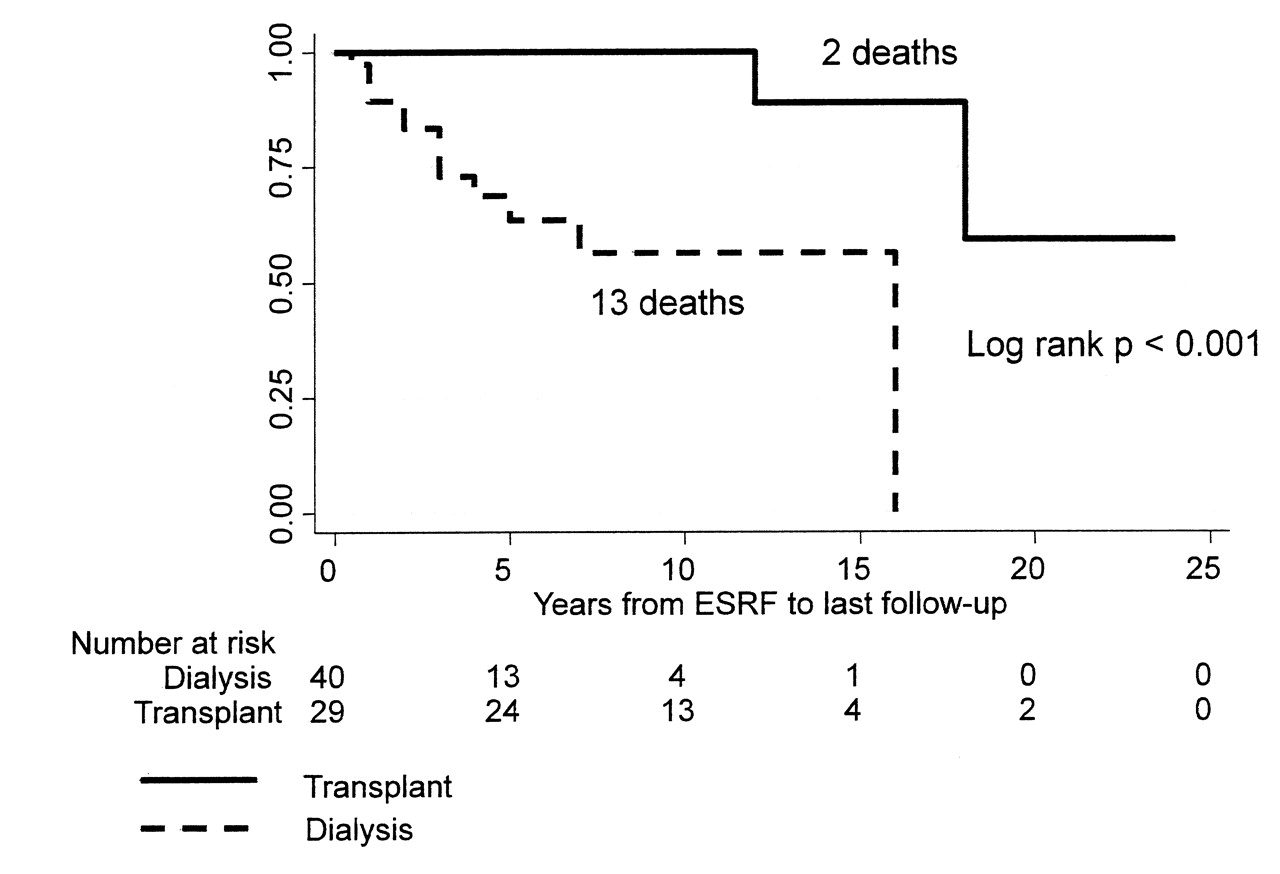
Kaplan-Meier survival in dialysis and transplant patients with SLE.
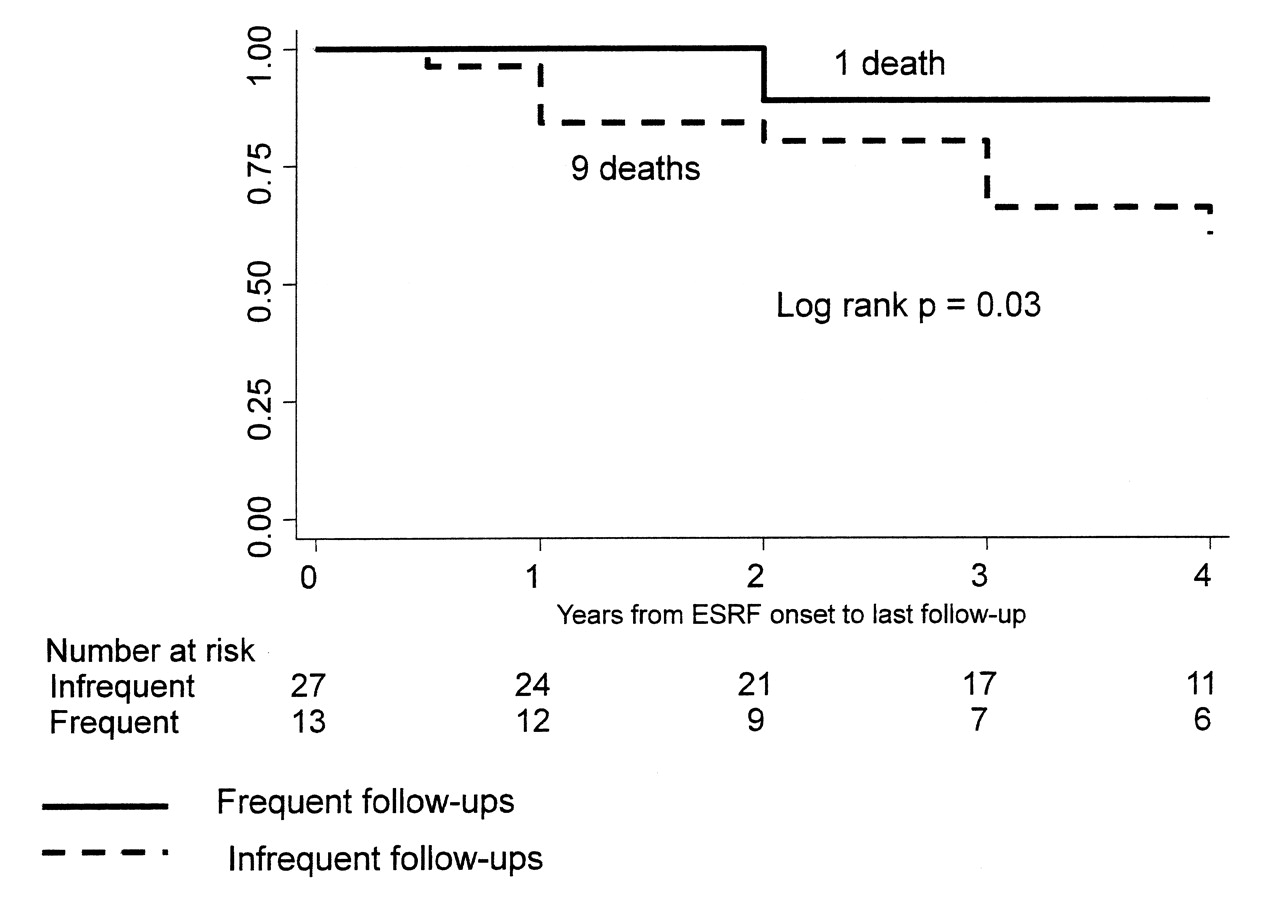
Four-year Kaplan-Meier survival among dialysis patients stratified by the frequency of rheumatology followup after ESRF.
Finally, we investigated whether survival was associated with different medication regimens. ESRF/SLE patients treated with Pred alone had survival rates similar to those of untreated patients, and significantly lower survival rates, compared with patients who were treated either with Pred/HCQ alone or with a combination of immunosuppressive medications with or without Pred/HCQ (log-rank p < 0.001; Figure 4). Similar results were observed in a subgroup of dialysis patients stratified by medication use (log-rank p = 0.02; Figure 5).

Kaplan-Meier survival stratified by medication use after ESRF. HCQ: hydroxychloroquine.

Kaplan-Meier survival among dialysis patients stratified by medication use after ESRF. HCQ: hydroxychloroquine.
Since we did not have enough information to confirm SLE diagnosis by ACR criteria in some of the patients, we performed survival analysis in 58 patients with definite or probable SLE who met at least 3 SLE criteria and/or had biopsy-proven lupus nephritis. Similar to the overall cohort, untreated patients and patients taking Pred alone had much lower survival rates compared with patients treated with Pred/HCQ or other immunosuppressive medications (log-rank p < 0.001; Figure 6).

Kaplan-Meier survival analysis among people who met at least 3 American College of Rheumatology criteria and/or had biopsy-proven lupus nephritis stratified by medication use after ESRF. HCQ: hydroxychloroquine.
In the adjusted Cox proportional hazards model (Table 2), untreated patients had a hazard ratio (HR) of death of 13 (95% CI 1.5, 106; p = 0.02) compared with those who were on a combination of medications. Similarly, those who were taking Pred alone had a HR of death of 6.1 (95% CI 1.1, 34; p = 0.04) compared with those who were on immunosuppressive therapy with or without Pred. Receiving a renal transplant was associated with a decreased HR of death of 0.08 (95% CI 0.01, 0.79; p = 0.03). This model was also adjusted for age at SLE onset, sex, and visit frequency post-ESRF.
Adjusted Cox proportional hazards model with death from any cause as an outcome and use of immunosuppressives as the main variable of interest*.
DISCUSSION
We show that survival rates are significantly higher in patients with SLE/ESRF who follow up at least twice a year with a rheumatologist, compared with those who follow up less than twice a year. This novel observation concurs with more recent evidence suggesting that SLE remains active after onset of ESRF. Thus, monitoring disease activity and adjusting immunosuppressive therapy may lead to improved survival after onset of ESRF. Further, patients receiving Pred alone had significantly lower survival rates compared with those who were on any other combination of immunosuppressive medications. The survival rates in patients treated with Pred alone were similar to those treated with no medications, suggesting that low-dose Pred may be inadequate treatment for SLE/ESRF patients. Based on our review of the literature, the association between rheumatology visits and immunosuppressant use with survival post-ESRF has not been previously reported. Thus, following up with rheumatologists and maintaining immunosuppressive therapies in SLE patients with ESRF may be modifiable risk factors for improving outcomes in these patients. This is an important observation and, if confirmed in prospective studies, may change the way SLE/ESRF patients are managed while undergoing RRT.
Use of immunosuppressive medications post-ESRF remained a significant predictor of improved survival even after adjustment for a history of renal transplant. Further, survival rates were similar between patients receiving the Pred/HCQ combination and patients on other immunosuppressive therapies, suggesting that the Pred/HCQ combination may provide a survival benefit in SLE/ESRF unrelated to their transplant status.
Our study has several limitations related to its retrospective design and a relatively small sample size. Confidence intervals in the Cox proportional hazards model were influenced by the relatively small sample size and relatively few deaths in the stratified analysis.
We did not have sufficient information about lupus activity scores in this cohort pre- or post-ESRF, since disease activity was not monitored in those who did not follow up with rheumatologists. Nevertheless, we were able to determine information related to SLE activity pre-ESRF for 35 patients, and found no difference between the 2 groups. However, these findings need to be interpreted with caution because of the missing data.
Missing information, differential selection, and differential and nondifferential misclassification, especially with respect to the diagnosis of SLE by rheumatologists vs other physicians, may have affected the results in this retrospective analysis. To evaluate whether excluding the 11 patients with missing time of ESRF onset from survival analysis influenced our results, we performed survival analysis using the first year of followup for these patients, and obtained similar results.
We could not assess compliance in this study. Therefore, patients who were followed more frequently post-ESRF may have been generally more compliant and concerned about their health, which would lead to lower mortality rates. Alternatively, if patients who visit rheumatologists frequently post-ESRF have more active SLE, the true differences in mortality rates between “frequent” and “infrequent” groups would be underestimated. Further, the differences in survival stratified by medication use are less likely to be explained by compliance alone.
It is also possible that patients in our study who followed up infrequently with MMC rheumatologists after starting RRT were following up with rheumatologists outside MMC. In this case there are 2 possible interpretations of our results with respect to the visit frequency: (1) receiving centralized care at a large tertiary care center after starting RRT is associated with better survival; (2) the actual survival differences between SLE patients who follow up with rheumatologists post-ESRF and SLE patients who do not follow up with rheumatologists post-ESRF may be underestimated in our analysis. Nevertheless, since MMC is the only tertiary care center in the Bronx, and all the patients included in the study were receiving medical care for other conditions at MMC, it is unlikely that a significant number of these patients were followed by outside rheumatologists.
Finally, we chose to use all-cause mortality rather than SLE-related mortality as the main outcome, since cause of death was unknown for 3 patients, and causes of death listed on death certificates are not always accurate and reliable23. However, we did investigate whether frequent followup visits post-ESRF were associated with SLE-related mortality. While the results showed a trend similar to all-cause mortality, they did not reach statistical significance, most likely because there were only 8 deaths attributed to SLE. We plan prospective studies to address some of these limitations and to evaluate the associations observed in this study.
Despite these limitations, overall mortality rates and data related to progression of ESRF observed in our study are consistent with those reported in other studies3,4,24, suggesting that our results may be generalized to the overall SLE/ESRF population undergoing RRT.
We considered whether some of the survival differences observed between patients on immunosuppressive therapy plus low-dose Pred and those on no medications were due to the fact that among the 36 patients on immunosuppressive therapy post-ESRF, 27 (75%) were renal transplant patients. However, medication use post-ESRF independently predicted survival in the Cox proportional hazards model, even after adjustment for transplant rates. Another important observation is that post-ESRF, the Pred/HCQ-only subgroup (not including transplant patients) had survival rates similar to the subgroup on immunosuppressive therapy (including renal transplant patients). Further, similar survival analysis results were observed in the subgroup of dialysis patients.
Treatment with immunosuppressive therapies with or without prednisone in ESRF/SLE patients undergoing RRT is associated with lower mortality rates compared to either prednisone alone or no treatment in the entire study cohort, and in the subgroup of dialysis patients. Indeed, some of the improved survival observed in renal transplants may be secondary to immunosuppression and better SLE control. Our results provide preliminary evidence that active lupus disease in SLE/ESRF patients on RRT may be underrecognized and undertreated, which may lead in turn to increased all-cause mortality. Close monitoring of disease activity and maintenance therapy for SLE with HCQ and other immunosuppressive treatments may improve survival in post-ESRF patients on RRT.
Acknowledgment
We thank Miriam Gordon, PhD, for valuable assistance in editing the manuscript.
Footnotes
-
Supported in part by a National Institutes of Health grant, RO1 AR048692, to Dr. Putterman.
- Accepted for publication June 27, 2011.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}