
Abstract
Objective. To determine small artery elasticity (SAE) in patients with longstanding rheumatoid arthritis (RA) in comparison to healthy controls, and to investigate its relation to markers of endothelial cell activation, disease activity, joint damage, and the presence of atherosclerosis.
Methods. Forty-nine patients with RA and 50 age- and sex-matched healthy controls were studied. Traditional cardiovascular risk factors and disease-related factors were recorded. SAE was measured noninvasively by pulse-wave analysis (PWA). Endothelial activation was assessed by measuring levels of soluble vascular cell adhesion molecule-1 (sVCAM-1) and von Willebrand factor (vWF). Carotid intima-media thickness (IMT), as an indicator of subclinical atherosclerosis, was assessed using ultrasonography.
Results. Patients with RA had higher body mass index, blood pressure, and triglyceride levels and were more often cigarette smokers compared to controls. SAE was decreased in RA patients compared to controls and was inversely related with age, smoking, blood pressure, vWF, sVCAM-1, high sensitivity C-reactive protein, and IMT. Presence of RA was independently related to SAE in multivariate linear regression analysis. SAE was inversely related with the Health Assessment Questionnaire score. No correlation was found between SAE and other disease activity markers and damage. IMT in patients and controls was not different.
Conclusion. Small artery elasticity was decreased in patients with longstanding RA. The presence of RA was independently associated with SAE. Whereas IMT in patients with RA was not increased, we hypothesize that endothelial dysfunction, reflected by decreased SAE, is present prior to IMT thickening in these patients.
- SMALL ARTERY ELASTICITY
- ENDOTHELIAL DYSFUNCTION
- ATHEROSCLEROSIS
- RHEUMATOID ARTHRITIS
Rheumatoid arthritis (RA) is associated with increased mortality, mostly due to an excess of cardiovascular disease1,2,3,4,5,6. Even after adjustment for traditional cardiovascular risk factors such as hypertension, diabetes mellitus, smoking, and hypercholesterolemia, a higher rate of atherosclerosis and cardiovascular events in patients with RA compared to healthy subjects has been reported7,8. Therefore it is suggested that additional mechanisms, including genetic factors, are responsible for the excess cardiovascular disease risk observed in RA8,9,10,11,12,13.
Atherosclerosis is regarded as an inflammatory disease that develops over years3,14,15. Early detection might open possibilities for intervention, aiming at the prevention of clinically manifest cardiovascular diseases. Activation and dysfunction of endothelial cells are considered to be the first steps in this inflammatory process15,16. Endothelial activation can be demonstrated by detection of elevated plasma levels of von Willebrand factor (vWF) and soluble adhesion molecules10,14,16,17. Endothelial dysfunction, reflected by decreased small artery elasticity (SAE), can be measured noninvasively by pulse-wave analysis (PWA), a local tonometric assessment of vascular elasticity. PWA is rapid, well tolerated, and reproducible18,19,20,21 and correlates with results of flow-mediated vasodilatation (FMD), another method to determine endothelial cell function19,22,23. SAE inversely relates to intima-media thickness (IMT) of the common carotid artery24, which is considered an indicator of generalized subclinical atherosclerosis25,26.
As atherosclerosis might be more pronounced in patients with longstanding RA27, we hypothesized that in these patients in particular, signs of endothelial cell dysfunction and loss of vascular elasticity would be present. The aim of our study was to evaluate SAE in patients with RA in comparison to healthy controls and to investigate its relation to endothelial cell activation, disease activity, joint damage, and IMT.
MATERIALS AND METHODS
Patients and controls
Fifty consecutive patients fulfilling the American College of Rheumatology criteria for RA28 and a disease duration of at least 11 years, who attended the outpatient clinic of the University Medical Center Groningen, were asked to participate in this study. Patients and healthy controls were recruited at the end of 2008 and beginning of 2009. Healthy controls were recruited in the city of Groningen. One patient dropped out before measurements took place. Exclusion criteria were pregnancy, diabetes mellitus (fasting blood glucose ≥ 7.0 mmol/l or the use of antidiabetic medications), renal impairment (serum creatinine > 140 μmol/l), recent surgery, and myocardial infarction or sepsis in the previous 3 months. Fifty age- and sex-matched healthy volunteers were recruited as controls.
Information was obtained from all subjects regarding traditional cardiovascular risk factors. Blood pressure (BP) and lipid levels were measured. Information regarding body mass index (BMI), smoking, family history of cardiovascular disease, and manifest cardiovascular disease was based on information given by the subjects themselves. The 10-year coronary heart risk was calculated using the Framingham risk score29.
Hypertension was defined as systolic BP > 140 mm Hg and/or diastolic BP > 90 mm Hg and/or current use of antihypertensive drugs30,31. Dyslipidemia was defined as plasma cholesterol > 6.21 mmol/l (240 mg/dl), plasma low-density lipoprotein (LDL) cholesterol > 3.36 mmol/l (130 mg/dl), plasma triglycerides > 2.26 mmol/l (300 mg/dl), or current use of lipid-lowering drugs30,32. Family history of cardiovascular disease was considered positive if first-degree relatives had cardiovascular disease before age 60 years31. Information on current medication use of patients and controls was obtained by questionnaire. In addition, medical records of patients were reviewed, with special focus on disease-modifying antirheumatic drugs (DMARD), nonsteroidal antiinflammatory drugs (NSAID), and lipid-lowering and antihypertensive drugs. Subjects were studied in the morning after an overnight fast and abstinence from tobacco, caffeine, and alcohol.
The local research ethics committee gave approval for the study and informed consent was obtained from each participant.
Blood sampling and analysis
Complete blood sampling for standardized laboratory assessments was performed as appropriate in all individuals: creatinine, total cholesterol, triglycerides, high-density lipoprotein (HDL), LDL, high sensitivity C-reactive protein (hsCRP), erythrocyte sedimentation rate (ESR), and glucose. Blood samples were obtained from each participant on the day of vascular measurements.
Serum and plasma samples were stored at −20°C for determination of endothelial cell activation markers. Serum levels of soluble VCAM-1 (sVCAM-1) were measured according to the manufacturer’s instructions (R&D Systems, Abingdon, UK). Levels of vWF were determined using an in-house ELISA as described33.
Measurement of RA disease activity
Disease activity was assessed using the Disease Activity Score for 28 joints (DAS28)34,35. Ranges of DAS28 scores have been proposed to correspond with disease activity. DAS28 > 5.1 indicates high disease activity, DAS28 > 3.2 to 5.1 moderate disease activity, DAS28 2.6 to 3.2 low disease activity, and DAS28 < 2.6 indicates remission36.
Measurement of functional disability
The Health Assessment Questionnaire (HAQ) evaluates patients’ ability to perform activities of daily living, as described37. The final HAQ index ranges from 0 to 3. Although the mean HAQ of the population rises with age, HAQ scores < 0.3 are considered normal37. Increasing disability is indicated by higher HAQ scores. The HAQ score reflects both joint damage and disease activity38,39.
Measurement of joint damage
To determine the amount of joint damage, we used the van der Heijde modification of the Sharp method40. The maximum erosion score in the hands is 160 and in the feet 120; the maximum score for joint space narrowing in the hands is 120 and 48 in the feet, resulting in a maximum total score of 44840. Radiography of the hands and feet was performed when recent radiographs, taken within 1 year, were not available.
Measurement of small artery elasticity
Arterial elasticity was assessed by pulse-wave analysis using the CR-2000 (Hypertension Diagnostics, Eagan, MN, USA). The CR-2000 records and analyzes BP waveform data from the arterial pulse pressure sensor. SAE was estimated from a computerized pulse contour analysis using a Windkessel model41,42. Measurements were performed after 10 min of acclimatization in a temperature-controlled room (22°C) with the subject in supine position. The arterial pulse pressure sensor was placed over the right and subsequently over the left radial artery. A BP cuff was placed on the opposite arm to record BP. The average of 3 readings of heart rate, BP, and SAE of both the left and right arm were used for analysis. The intraindividual coefficient of variation for SAE in our laboratory was 11.2%.
Measurement of IMT
Details of the method have been described by de Groot, et al43. In short, IMT was determined in the far wall segments of the common carotid artery, carotid bulb, and the internal carotid artery. A B-mode image of these segments was obtained from a lateral transducer position, during which the probe was positioned perpendicular to the far wall, showing an intima-media complex over about 1 cm. Subjects lay in the supine position. Mean IMT (mean of the measurements in a segment) and maximum IMT (the highest IMT value found within the segment studied) per segment were calculated. Mean mean IMT (further referred to as mean IMT) and mean maximum IMT (further referred to as maximum IMT) were calculated as the average for the 6 carotid segments of mean value and of the maximum value per segment, respectively43.
Statistical methods
Power analysis revealed that 45 subjects had to be included in each group to detect a difference in SAE of 2 mm Hg × 100 with an SD of 2.8, as we previously found (data not shown), at a significance level of 0.05 with a power of 90%. Anticipating missing data, we included 50 subjects in each group. Data are expressed as mean (± SD) when normally distributed and as median with interquartile range (25%–75%) when non-normally distributed. Two-sample t tests or Mann-Whitney tests were used to make comparisons between patients and controls for continuous variables. The chi-square method was used for categorical variables and Fisher’s exact test for very small expected frequencies. Correlation analyses were performed by Pearson correlation when variables were normally distributed, otherwise the Spearman correlation was used. Independent associations of SAE with RA and other traditional cardiovascular risk factors were assessed using multivariate linear regression analysis. All analyses were performed using SPSS 16.0. Two-sided p values < 0.05 were considered significant.
RESULTS
Clinical characteristics of patients and controls
Characteristics of patients and controls are given in Table 1. Concerning traditional cardiovascular risk factors, BMI, number of cigarette smokers, prevalence of hypertension, and levels of triglycerides were higher in patients with RA compared to controls. HDL levels were lower in patients with RA than in controls. As expected, median CRP levels were significantly higher in patients compared with controls (p < 0.001).
Clinical characteristics of patients and controls. Data are expressed as mean ± (SD) when normally distributed or as median (25–75%) when non-normally distributed.
Disease-related factors
The mean disease duration was 12.5 (11.0–14.1) years. Although presence of rheumatoid factor (RF) and antibodies against citrullinated proteins (ACPA) was not an issue in the selection process, it is notable that 48 (98%) of the patients were RF-positive and 39 (80%) ACPA-positive. The median HAQ score was 0.18 (0.0–0.64), the mean DAS28 score 3.09 (± 1.26), and the median modified Sharp-van der Heijde score was 19 (9.0–39.0).
At the time of measurement, 88% of patients were treated with 1 or more DMARD and 59% used an NSAID. Methotrexate was used by 63% of patients. Only 14% of patients were treated with prednisolone (Table 2).
Disease-related factors in patients. Data are expressed as mean ± SD when normally distributed and as median (25–75%) when non-normally distributed.
Markers of endothelial cell activation
RA patients had higher levels of sVCAM-1 and vWF than healthy controls (both p < 0.001; Table 3).
Surrogate markers for atherosclerosis and endothelial cell activation. Data are expressed as mean ± SD when normally distributed and as median (25–75%) when non-normally distributed.
Small artery elasticity
SAE was decreased in RA patients compared to healthy controls (p < 0.001; Figure 1 and Table 3). When data from patients and controls were analyzed together, SAE was found to be negatively correlated with age (r = −0.429, p < 0.001), mean IMT (r = −0.344, p = 0.001), maximum IMT (r = −0.276, p = 0.007), systolic BP (r = −0.292, p = 0.004), diastolic BP (r = −0.207, p = 0.041), hsCRP (r = −0.344, p = 0.001), sVCAM-1 (r = −0.247, p = 0.014), and vWF (r = −0.385, p < 0.001).

Small artery elasticity (SAE) and mean intima-media thickness (mean IMT) in RA patients and age and sex-matched healthy controls. SAE is significantly decreased in RA patients compared to controls. Mean IMT is not different between RA patients and controls. NS: nonsignificant.
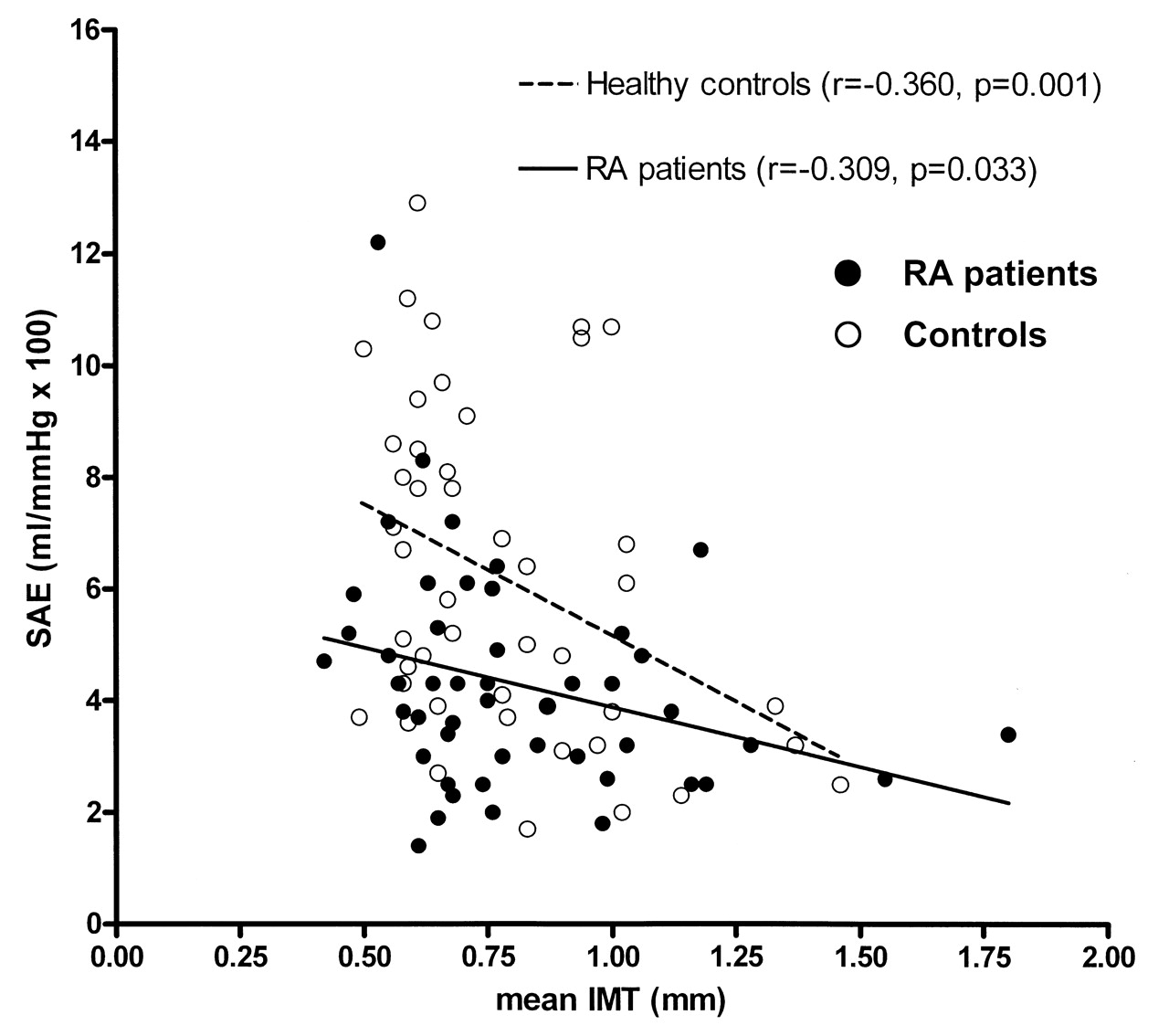
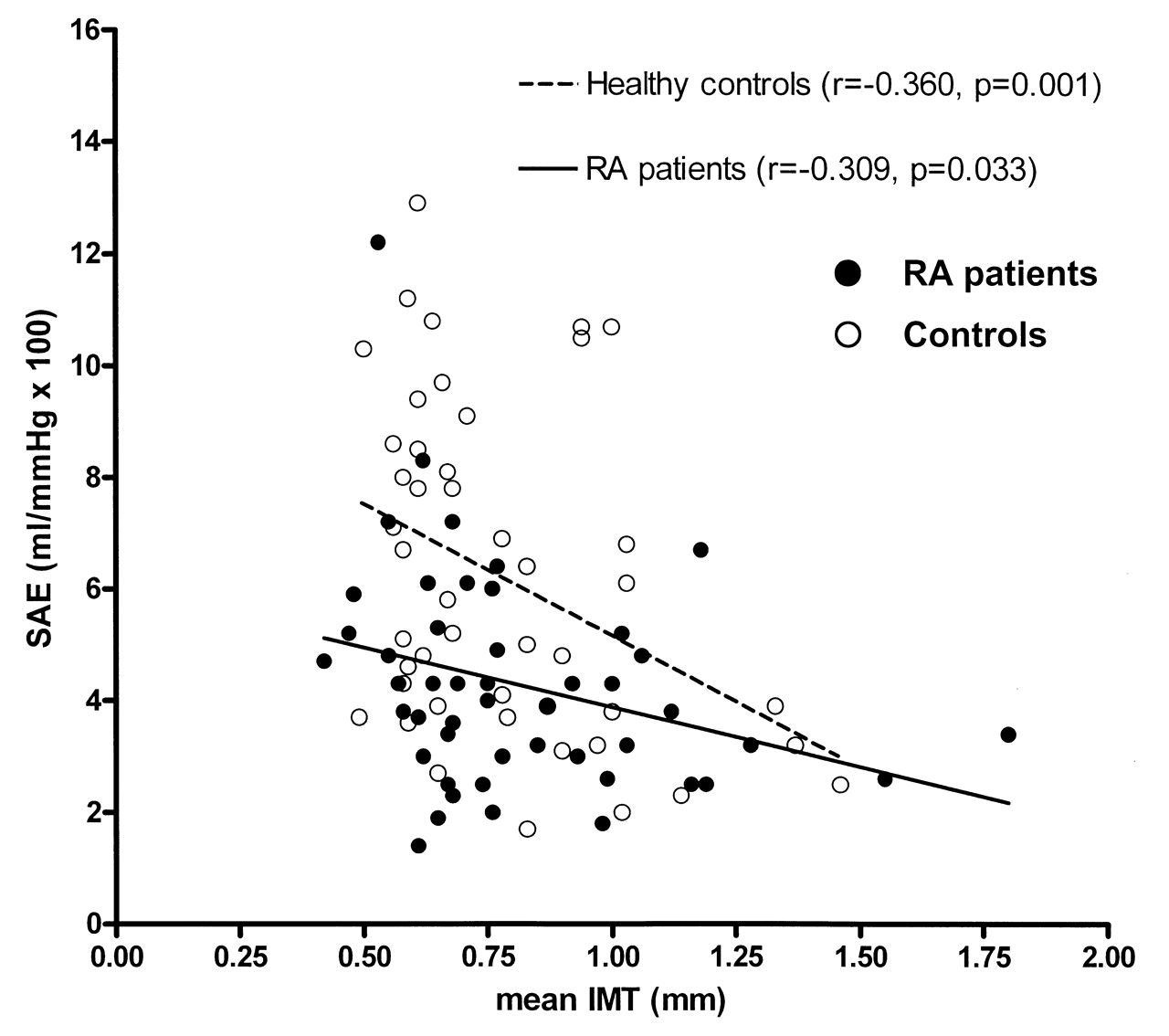
When RA patients were analyzed separately, the relation between SAE and mean IMT and maximum IMT remained (mean IMT: r = −0.309, p = 0.033; maximum IMT: r = −0.355, p = 0.013; Figure 2).
{kind=link}
{kind=link}
Relationship of small artery elasticity (SAE) to mean intima-media thickness (mean IMT). Closed dots represent patients and open circles represent controls. Solid line represents the correlation between SAE and IMT in patients (r = −0.309, p = 0.033). Broken line represents the correlation between SAE and IMT in healthy controls (r = −0.360, p = 0.001). IMT correlates negatively with SAE in both groups.
Further, SAE was negatively correlated with the HAQ score (r = −0.297, p = 0.040).
In multivariate linear regression analysis the presence of RA, smoking, and hypertension appeared to be independently associated with SAE (Table 4). After adding the term “history of cardiovascular disease” as an interactive term in our regression analysis, the presence of RA remained significant (p = 0.004 before adding this term, p = 0.008 after adding the term).
Regression analysis of associations with small artery elasticity (SAE), von Willebrand factor (vWF), or soluble vascular cell adhesion molecule-1 (sVCAM-1) as dependent variable in all subjects (n = 99) using multivariate linear regression analysis. Values are presented as B; B refers to the influence on dependent variable (SAE, vWF, and sVCAM-1, respectively). RA patients were defined as 1, controls as 0.
Further, in a subanalysis excluding patients (n = 7) and controls (n = 5) with a history of cardiovascular events, the presence of RA still remained independently associated with SAE (data not shown). Usage of NSAID was significantly associated with SAE in univariate regression analysis (r = −0.1338, p = 0.023). However, in multivariable regression analysis, usage of NSAID was not significant (r = −.0451, p = 0.496).
No correlation was found between SAE and other disease activity markers such as hsCRP and DAS28 score and joint damage as represented by the modified Sharp-van der Heijde score (data not shown).
DISCUSSION
In patients with longstanding RA, SAE is decreased, reflecting endothelial dysfunction. This decrease is related to age, hypertension, smoking, and mean IMT, but also independently to the presence of RA.
Consistent with results from other studies, we found a higher prevalence of several traditional risk factors (hypertension and smoking) in patients with longstanding RA compared to healthy controls5,21,44. In some studies SAE showed a negative correlation with high cholesterol levels45,46. Other studies, however, including ours, could not confirm this association21. In our study, lipid profiles were only slightly different between the RA patients and controls, as triglyceride levels were higher in RA patients and HDL levels were higher in controls. Further, no correlation was detected between BMI and SAE. Several other studies also found no association47,48, whereas others did find that obesity was associated with a decreased arterial compliance49,50,51. A possible explanation for this might be that there are limitations of BMI as an estimate of body fat. Fjeldstad, et al suggest that the association of BMI and arterial compliance may be dependent on the extent to which BMI reflects fat vs lean body mass47.
Although the prevalence of traditional cardiovascular risk factors differed between our 2 study groups, they cannot fully explain the decreased SAE in our patients, as the independent variable — that is, having or not having RA — showed a significant association with SAE in multivariate linear regression analysis.
Disease-related factors are probably involved in the pathophysiology of atherosclerosis in RA. Assuming that disease activity and in particular chronicity (reflected by increase in HAQ and increase in joint damage) might be related to development of endothelial dysfunction, we analyzed the relation between SAE and hsCRP, DAS28 score, HAQ score, and the modified Sharp-van der Heijde score. Surprisingly, correlations between SAE and markers of disease activity and damage were scarce. Only a weak negative correlation with the HAQ score was found (r = −0.297, p = 0.040). There were no other significant correlations between SAE and other markers of disease activity and joint damage.
A possible explanation for these results is that our patients had low to moderate disease activity and functional disability at the time of measurement, as shown by the low DAS28 score (mean 3.09), hsCRP (median 4.5), and low HAQ score (median 0.18). Further, the amount of damage, as measured by modified Sharp-van der Heijde score, was relatively low (median 19) in comparison to reports from other cohorts19,52. In patients with RA with higher damage scores, Van Doornum, et al found a significant inverse correlation between SAE and modified Sharp scores. In addition to differences in the score itself, differences in methods used for measuring joint damage (modified Sharp method versus modified Sharp-van der Heijde method) might also explain discrepancies19. Moreover, atherosclerotic damage in RA is the result of the cumulative effect of the chronic inflammatory burden. In this regard, an association between the mean values of CRP over an extended followup, rather than a single determination of CRP at the time of the carotid ultrasonography evaluation, and the carotid IMT has been reported53. Indeed, hsCRP as a marker of inflammation and vWF and sVCAM as markers of endothelial activation were also (inversely) related to SAE, but not to IMT (data not shown), supporting the suggestion that SAE reflects actual disease activity and IMT reflects presence of chronic inflammation.
SAE was also inversely related to IMT (Figure 2). Nevertheless, we did not find a significant difference in IMT between patients and controls, despite longstanding disease and increased levels of endothelial cell activation markers, such as vWF and sVCAM-1, in the patients with RA. This seems to be in contrast to a majority of other studies that demonstrated an increased mean IMT in RA patients compared to healthy controls54. Increased IMT was described in patients with a longer duration of RA27,55,56 as well as in patients with a shorter disease duration17,25,57. Although IMT is accepted as an early surrogate marker for atherosclerosis, it might not always give a good indication of actual atherosclerosis. Georgiadis, et al58 described that patients with early active RA (DAS28 score 5.8, indicating high disease activity) had an increased IMT compared to controls, which improved after therapy. They stated that effective suppression of disease activity with methotrexate at an early stage was associated with improvement of IMT, suggesting that IMT at this stage of disease reflects intimal inflammation rather than atherosclerosis.
The low to moderate disease activity and low functional disability in our patients probably explains why no difference in IMT could be found between patients and controls. Indeed, in comparison, disease activity as indicated by the hsCRP, ESR, HAQ score, and DAS28 score was higher in other studies25,55,57,58,59,60. Finally, it is acknowledged that our study was not specifically powered to detect differences in IMT.
In our study, SAE was chosen to measure endothelial dysfunction, as SAE is less bothersome than flow-mediated vasodilatation. Whether SAE is solely a measure of endothelial cell dysfunction has been debated61,62. Indeed, there is no consensus on standard measurement for endothelial cell dysfunction: some authorities advocate flow-mediated vasodilatation23,61,62, others choose SAE19. Although the physiological meaning of SAE remains unclear, it is regarded as a biomarker of vascular dysfunction19,20.
A limitation of our study is the relatively low number of patients included. Also, we did not exclude patients and controls who had had a cardiovascular event more than 3 months before inclusion; we deliberately chose this approach because including all patients reflected daily practice in our outpatient clinic as closely as possible. Realizing this might influence our results, we performed a subanalysis that excluded all patients and controls with a history of cardiovascular events. This subanalysis showed that the presence of RA remained independently associated with SAE. Further, we included out-clinic patients only; this also reflects daily practice, as we only have hospitalized patients occasionally. Finally, the ultrasonographer was not blinded to the health status of the participants.
In this cross-sectional study, SAE was decreased in patients with longstanding RA compared to healthy controls matched for age and sex. Presence of RA was independently associated with SAE. Whereas IMT in RA patients was not significantly increased, we hypothesize that endothelial dysfunction, reflected by decreased SAE, is present prior to thickening of the IMT in these patients. Prospective longitudinal studies are needed to test this theory and to evaluate the influences of disease activity and treatment on indicators of premature atherosclerosis.
Acknowledgment
We are grateful to W.J. Sluiter for help with the statistical analyses; and to the personnel of the vascular laboratory, M.C. Bruin, A.I. van Gessel, W.D. Kuipers, A. Possel-Nicolai, and G.C. Teune-Weesjes, for technical assistance and performance of pulse-wave analysis and measurements of intima-media thickness.
- Accepted for publication June 7, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.