

Abstract
Objective. To describe hepatitis C virus (HCV)-related systemic vasculitis in patients without detectable mixed cryoglobulinemia (MC) and to compare them to typical cases of HCV-MC vasculitis.
Methods. Twelve HCV RNA+ patients with histologically proven vasculitis in the absence of detectable MC (cases) were retrospectively compared with 48 HCV RNA+ patients with MC vasculitis (controls). Each case was matched with 4 controls for age and sex.
Results. The main epidemiological and virologic features were similar between cases and controls. No clinical difference was found, except for lower rates of arthralgias (33% vs 71%; p = 0.02) and purpura (50% vs 83%; p = 0.03) in cases. Cases showed higher mean serum C3 (1.17 ± 0.21 vs 0.93 ± 0.23 g/l; p = 0.01) and median C4 levels (0.25 vs 0.04 g/l; p < 0.001), lower median serum IgM levels (0.6 vs 1.9 g/l; p < 0.001), and lower rates of rheumatoid factor positivity (8% vs 82%; p < 0.001) than controls. The main histologic features were similar between cases and controls. Immunofluorescence analysis of skin biopsy from 1 case revealed perivascular deposits of C3 and IgA. After treatment, overall clinical response of vasculitis (75% vs 83%) and sustained virological response (40% vs 64%; p = 0.3) were similar between cases and controls, except for higher complete clinical response (42% vs 73%; p = 0.05) in controls.
Conclusion. HCV-related systemic vasculitis may occur in the absence of detectable MC. Our findings suggest that such vasculitis probably results from immune complex-mediated mechanisms, and that the therapeutic management of such vasculitis should be similar to that of HCV-MC vasculitis.
Systemic vasculitis comprises a group of disorders defined by inflammation of the blood vessel walls, which are classified according to their clinical and histologic features and the size of the predominantly affected vessels. Various pathogenic mechanisms have been implicated in the induction of vasculitis: (1) cell-mediated inflammation; (2) immune complex-mediated inflammation such as mixed cryoglobulinemia (MC) vasculitis and polyarteritis nodosa (PAN) associated with hepatitis B virus infection; and (3) autoantibody-mediated inflammation such as antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis1,2,3.
Shortly after the discovery of hepatitis C virus (HCV) in 1989, there was evidence that more than 80% of MC cases were associated with HCV infection4,5,6. In addition, among patients with HCV-related MC (HCV-MC), the prevalence of symptomatic vasculitis ranges from < 1% to 10% according to geographic distribution, with < 5% generally found in larger prospective studies7,8,9. MC is a systemic vasculitis without fibrinoid necrosis that mainly affects the small and, less frequently, medium-size vessels10, and reflects the expansion of B cells producing a pathogenic IgM with rheumatoid factor (RF) activity11,12. MC leads to clinical manifestations ranging from the so-called MC syndrome (purpura, arthralgia, and asthenia) to more serious lesions with neurologic and renal involvement13. Treatment of HCV-MC with severe organ involvement may target either the viral trigger (HCV) or the downstream B cell arm of autoimmunity14,15.
In addition to typical MC vasculitis, necrotizing vasculitis has been described less frequently with HCV infection, most often in association with detectable MC. This particular form of HCV-related vasculitis is described as a systemic necrotizing vasculitis that mainly affects medium-size vessels, with frequent life-threatening symptoms16. In addition, there has been description of patients with peripheral neuropathy occurring with HCV infection without detectable MC or antineutrophil cytoplasmic antibodies (ANCA)17. In these patients, neuromuscular biopsy demonstrated axonal neuropathy with perivascular lymphocytic vasculitis in half the cases, with no features of necrotizing PAN-like vasculitis.
The aim of our study was to describe clinical, biological, virologic, histologic, and therapeutic features and the outcome of patients presenting with systemic vasculitis without detectable MC occurring with HCV infection, and to compare these particular and rare forms of vasculitis to typical HCV-MC vasculitis.
MATERIALS AND METHODS
Patients
The study population consisted of 60 patients with HCV infection (HCV RNA+) and chronic active liver disease. The 12 cases (7 women, 5 men, mean age 60 ± 17 yrs) were defined as patients with histologically proven systemic vasculitis who had not shown evidence of MC on numerous occasions during a followup of 55 ± 38 months. Each case was matched with 4 controls for age and sex. The 48 controls (28 women, 20 men, mean age 60 ± 14 yrs) were randomly selected from our database of patients with typical HCV-MC vasculitis, i.e., they had serum MC levels > 0.05 g/l on at least 2 occasions associated with clinical manifestations of vasculitis (purpura or cutaneous ulcers, arthralgia, myalgia, peripheral neuropathy, renal involvement, cerebral vasculitis, gastrointestinal involvement, cardiac involvement)13. When more than 4 controls from our database were available for one case, controls were selected randomly. Controls were matched with only one case.
For each patient, clinical and biological data were retrospectively recorded at the time of the initial evaluation, during followup, and at the end of followup. Clinical data included age, sex, cutaneous involvement, arthralgia, neurological involvement, myalgia, gastrointestinal tract involvement, and organomegaly. Laboratory evaluation included a complete hemogram, a serum chemistry profile, and determination of the C3 and C4 fractions of complement, RF and cryoglobulin. A urinalysis was also completed to screen for hematuria, and 24-hour urine collection was performed to quantify daily excretion of protein. Virological and immunological serum markers, HCV antibodies, and RNA were detected as described18. HCV genotyping was performed using a second-generation line probe assay (LiPA; Innogenetics, Brussels, Belgium). Liver biopsy specimens were evaluated according to the validated Metavir scoring system19. Cryoglobulin concentrations were measured and classified as described18. Immunological evaluation included determination of RF and complement components using standard methods. ANCA detection by indirect immunofluorescence was performed on ethanol-fixed human neutrophils (INOVA provided by Menarini, Antony, France).
Histological diagnosis of vasculitis
All the cases (n = 12) had histologically proven vasculitis. Among the cases, 7 patients underwent neuromuscular biopsy, 4 skin biopsy, and 1 muscle biopsy. Among the controls, 13 patients underwent neuromuscular biopsy, 8 kidney biopsy, 2 skin biopsy, and 1 gall bladder biopsy. Kidney biopsy from controls showed typical membrano-proliferative glomerulonephritis, and histological analysis of gall bladder biopsy revealed leukocytoclastic vasculitis.
Patients with vasculitis of small-size vessels (i.e., capillaries, venules, or arterioles) without fibrinoid necrosis associated with serum cryoglobulins were considered to have MC vasculitis. Patients with small and/or medium-size vessel vasculitis associated with fibrinoid necrosis were considered to have necrotizing vasculitis. Among the patients with necrotizing vasculitis (2 cases, 8 controls), medium vessel involvement was documented in 5 patients, while the diameter of the largest affected vessel could not be assessed in 5 patients given the intensity of the necrotizing process. Half the controls (n = 24) had histologically proven vasculitis. Other control patients with purpura were considered to have small-vessel vasculitis based on previously defined clinical and biological criteria2. Patients were considered to have PAN-like vasculitis according to the American College of Rheumatology 1990 criteria20.
The histological features of vasculitis of cases and controls were reviewed by the same neuropathologist (TM), who works in a reference center for peripheral neuropathy. The pathologist assessed the histologic slides and the following features were recorded: type and localization of inflammatory cells, intensity of the inflammatory infiltrate, signs of vessel wall alteration, and presence of fibrinoid necrosis.
Frozen nerve biopsy specimens from 1 case and 1 control and skin biopsy from 1 case were prepared for immunofluorescence (IF) microscopy using standard techniques. The fluorescent-conjugated anti-human IgG, IgA, IgM, C3, and kappa-light chain antibodies were examined. Immunofluorescence analysis of nerve biopsy specimens was reviewed by PR and skin biopsy specimens by NO.
Response to antiviral therapy
The clinical response of vasculitis to anti-viral treatment (interferon-α, ribavirin) was defined by analyzing the course of the following main clinical signs: skin involvement (absence of purpura), peripheral neuropathy (clinical and/or electrophysiological improvement at 2 successive examinations), renal involvement (normalization of serum creatinine level and resolution of proteinuria), and absence of arthralgia. A complete clinical response was defined as an improvement in all baseline clinical manifestations. A partial response was defined as an improvement in at least half the baseline clinical manifestations. All other patients were classified as nonresponders. A relapse was defined as the reappearance of clinical signs of vasculitis. A sustained virological response was defined as the absence of detectable serum HCV RNA (< 12 IU/ml) 6 months after the discontinuation of antiviral treatment; the remaining patients were classified as virological nonresponders.
Statistical analysis
Data are presented as mean (SD) or as median (range) as appropriate for continuous variables and frequency (percentage) for qualitative variables. Conditional logistic regression analysis was used to compare patients without MC to their matching controls and to estimate unadjusted odds ratios (except for HCV genotype and RF positivity, for which a Fisher exact test was performed). For continuous variables, assumption of linearity was checked using generalized additive models with splines. All tests were 2-sided and a p value < 0.05 was considered significant. Statistical analyses were performed using R version 2.8.0 (R Development Core Team, 2008; R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Patient characteristics
The main epidemiological, clinical, virologic, biological, and histologic characteristics of the 12 cases and 48 controls with systemic vasculitis and chronic active HCV infection, according to presence or absence of detectable MC, are given in Tables 1 and 2.
Baseline epidemiological and virologic features of the 60 patients with systemic vasculitis and chronic active HCV infection according to presence or absence of detectable MC. Except where indicated otherwise, values are no. (%).
Baseline clinical, biological, and histologic features of the 60 patients with systemic vasculitis and chronic active HCV infection according to presence or absence of detectable MC.
The main epidemiological features and characteristics of HCV infection (HCV genotype, HCV-RNA level, duration of infection, severity of liver lesions) were similar between cases and controls. Cases with undetectable MC (n = 12) compared to controls with detectable MC (n = 48) showed lower rates of arthralgias (33% vs 71%; p = 0.02) and purpura (50% vs 83%; p = 0.03). No other specific pattern of vasculitis-related organ involvement was found between cases and controls. The distribution of PAN-like vasculitis was not different between cases and controls (p = 0.2). Mean serum C3 and median serum C4 complement components were significantly higher in cases compared to controls [1.17 ± 0.21 vs 0.93 ± 0.23 g/l, p = 0.01; and 0.25 (0.06–0.41) vs 0.04 (0.01–0.3) g/l, p < 0.001, respectively]. The median serum IgM level was lower in cases than in controls [0.6 (0.3–1.8) vs 1.9 (0.6–9.6) g/l; p < 0.001). Cases compared to controls showed lower rates of RF positivity (8% vs 82%; p < 0.001). None of the cases or controls had ANCA. The mean followup was 55 ± 38 months for cases and 56 ± 39 months for controls.
Histologic characteristics of patients
Ten cases (83%) had small-vessel vasculitis consistent with MC-type vasculitis, and 2 (17%) necrotizing vasculitis. Sixteen controls (67%) had small-vessel vasculitis consistent with MC-type vasculitis, and 8 (33%) medium-size vessel vasculitis with fibrinoid necrosis consistent with PAN-type vasculitis. The distribution of histological types of vasculitis (i.e., small and/or medium-size vessel involvement) was not different between cases and controls (p = 0.2).
Histologic slides of superficial peroneal nerve biopsies from cases and controls with MC-type vasculitis were reviewed in order to compare the type of histological lesions related to the presence or absence of MC. Examination of nerve biopsies from cases and controls showed the same type of histological lesions between the 2 groups. Perivascular, epineural, and perineural inflammatory mononuclear cell infiltrates were found, without blood vessel wall invasion or fibrinoid necrosis. However, inflammatory infiltrates were more prominent and intense in controls (> 150 cells) than in cases (approximately 50 cells; Figure 1A–1D).

Paraffin-embedded longitudinal sections of superficial peroneal nerve biopsy from patients with hepatitis C virus-associated vasculitis (H&E stain, original magnification x270). A and B. Nerve biopsy samples from cases [no detectable mixed cryoglobulinemia MC)] show moderate perivascular and perineural inflammatory mononuclear cell infiltrates (approximately 50 cells). Mononuclear cells do not invade the blood vessel wall. C and D. Nerve biopsy samples from controls (with MC) show the same type of histological lesions, except for more intense inflammatory mononuclear cell infiltrates (> 150 cells). E and F. Paraffin-embedded section of dermis from a patient with HCV-associated vasculitis without MC (H&E stain, original magnification x200 for E, x400 for F). Skin biopsy specimen shows leukocytoclastic vasculitis in small vessels of the upper to middle dermis.
Skin biopsy specimens from all 4 patients demonstrated leukocytoclastic vasculitis in the small vessels of the upper to middle dermis (Figure 1E, 1F).
Immunofluorescence analysis of nerve biopsy specimens from 1 case and 1 control did not show significant deposition of complement or immunoglobulins (Figure 2A). In contrast, IF analysis of skin biopsy specimen from 1 case revealed perivascular deposits of C3 and IgA (Figure 2B).
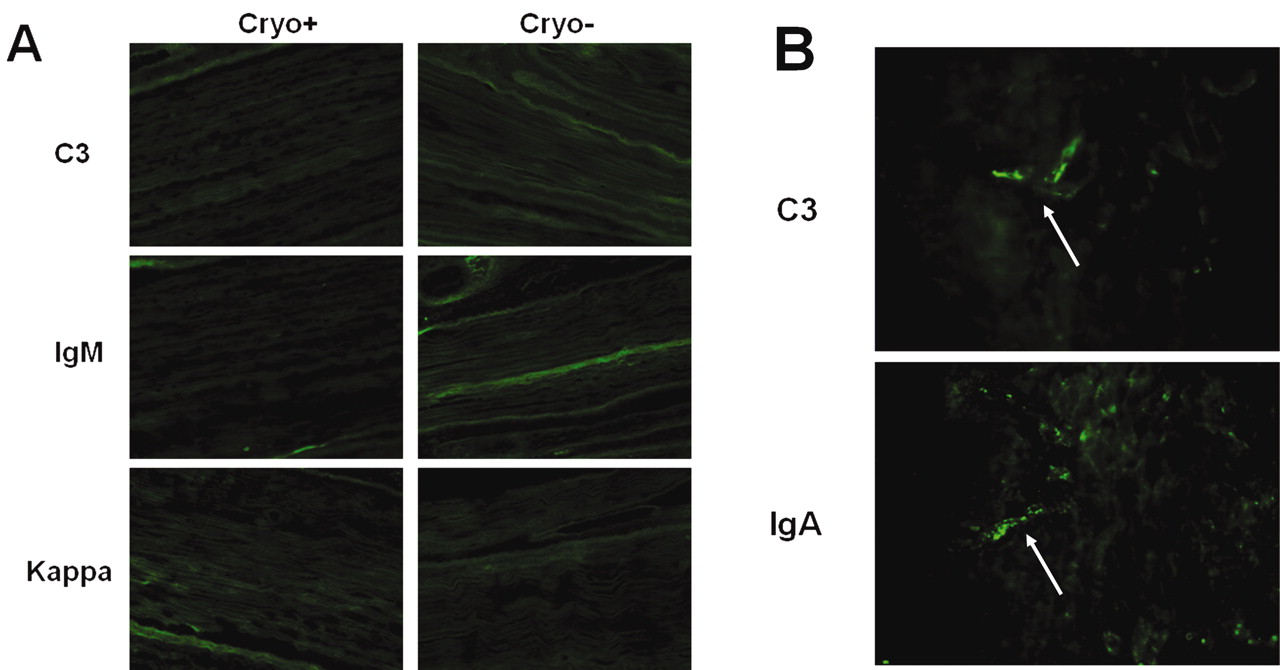
Immunofluorescence (IF) analysis of frozen nerve and skin biopsy specimens. A. Nerve biopsy specimens from 1 case and 1 control show no significant deposition of C3 complement fraction, IgM, and kappa light-chain. B. Skin biopsy specimen from 1 case reveals perivascular deposits of C3 and IgA (arrows).
Response to treatment in cases and controls
Treatment in cases consisted of antiviral therapy (interferon-α plus ribavirin) in 10 patients (83%), prednisone in 8 (67%), plasmapheresis and cyclophosphamide in 1 (8%) each, and rituximab in 2 (17%). Treatment in controls consisted of antiviral therapy in 44 patients (92%), prednisone in 19 (40%), plasmapheresis in 12 (25%), cyclophosphamide in 4 (8%), and rituximab in 11 (23%). No significant difference was found between these 2 groups, although the cases were receiving prednisone more frequently than the controls (67% vs 40%; p = 0.08; Table 3).
Therapeutic management and clinical and virological response to therapy of the 60 patients with systemic vasculitis and chronic active HCV infection according to presence or absence of detectable MC. Except where indicated otherwise, values are no. (%).
Similar rates of overall clinical response of the vasculitis were found between cases and controls (75% vs 83%, respectively). The cases exhibited a trend of lower rates of complete clinical response than the controls (42% vs 73%; p = 0.05). After antiviral therapy, no significant difference in sustained virological response was found between the cases and controls (p = 0.03).
DISCUSSION
We found that systemic vasculitis in patients with HCV infection without detectable MC had epidemiological, clinical, biological, virologic, and histologic features similar to typical HCV-MC vasculitis, except for lower rates of arthralgias and purpura and the absence of indirect biomarkers of MC. In our entire cohort of patients with HCV-related vasculitis, patients without detectable MC represented roughly 8% of the patients.
The absence of detectable MC in our series of cases was based on the negative results of repeated cryoglobulin detection during a long followup. The possibility of overlooking MC in cases can be ruled out as the methods used in our immunology department have proven sensitivity in detection of cryoglobulin21, and the cases did not show indirect biomarkers of MC such as RF (except in 1 case) and low serum C4 level (except in 1 case). The diagnosis of vasculitis was histologically proven in all the cases without detectable MC. No patient in our study population had other causes of systemic vasculitis such as ANCA-associated vasculitis, hepatitis B virus or human immunodeficiency virus coinfection, or other autoimmune disorders.
The absence of detectable MC in such HCV-related systemic vasculitis raises questions regarding the possible pathogenic mechanisms involved in the vasculitic inflammatory process. First, we hypothesized that a direct infection and in situ replication in target tissues could be responsible for vasculitis. However, the direct pathogenicity of HCV has been studied recently in MC vasculitis. A positive-strand genomic HCV RNA was detected in tissues of up to 30% of patients with MC vasculitis, whereas negative-strand replicative RNA was not detected. This lack of local HCV replication indicated that HCV-MC neuropathy probably results from virus-triggered immune-mediated mechanisms rather than from direct nerve infection and in situ replication22. In HCV-related vasculitis without detectable MC, there is no local HCV replication, but it would be interesting to assess the presence of the replicative strands of HCV RNA using special reverse transcription nested polymerase chain reaction in tissue samples of these patients.
Second, HCV-related vasculitis without MC could result from cell-mediated inflammation rather than immune complex and cryoglobulin-mediated inflammation. As in giant cell arteritis, dendritic cells of the blood vessel could be responsible after contact with HCV antigens for the activation of T cells, which would orchestrate vascular injury by recruiting macrophages and monocytes to the vessel walls, leading to intimal thickening and vessel occlusion1. However, we found similar histologic features in patients with and without detectable MC, and in particular MC-type vasculitis in the majority of patients without MC and the absence of epithelioid cells or granulomas.
Lastly, MC serum levels may have been too low to be detectable but sufficient for the formation of circulating immune complexes and deposition within the vessel wall. The absence of differences on histologic examination, except for more prominent and intense inflammatory infiltrates in controls with detectable MC than in cases without detectable MC, supports common pathogenic mechanisms, i.e., an immune complex-mediated inflammation. The IF analysis of nerve biopsy specimens showed no complement or immunoglobulin deposition in cases or controls. The absence of immune complex deposition has been reported in peripheral nerve from patients with MC vasculitis, suggesting a minor role for humoral mechanisms in the formation of vasculitic lesions in the peripheral nerve23. T cells and macrophages were the dominant infiltrating cells in vascular walls, and a T cell-mediated process appears to be the primary mechanism of vessel injury from MC vasculitis patients with peripheral neuropathy. In contrast, microscopic examination of skin biopsy specimens from cases demonstrated leukocytoclastic vasculitis with perivascular deposits of C3 and IgA, consistent with an immune complex disease. Besides complement and immunoglobulin depositions, analysis of HCV antigen deposition within vasculitic lesions would be of interest in order to precisely define any underlying pathogenic mechanisms.
Because of the retrospective design of our study and the low number of patients, any conclusions should be interpreted with caution. However, sensitive methods were used for detection of cryoglobulin, and diagnosis of vasculitis was histologically proven in all the cases without detectable MC and reviewed by the same neuropathologist from a national reference center for peripheral neuropathy.
In summary, physicians should be aware of the occurrence of systemic vasculitis during HCV infection in the absence of detectable serum MC. Systemic vasculitis without MC showed quite similar epidemiological, clinical, biological, virologic, and histological features as MC vasculitis, except for lower rates of arthralgias and purpura and the absence of indirect biomarkers of MC. Response to therapy was also comparable between patients with and those without MC. Our findings suggest that HCV-related vasculitis without detectable MC probably results from immune complex-mediated mechanisms. However, even if no definitive conclusions may be drawn regarding pathogenesis of such vasculitis, the therapeutic management should be similar to that of typical HCV-MC vasculitis.
- Accepted for publication August 17, 2010.








{kind=link}
{kind=link}