

To the Editor:
Olech, et al1 recently used extremity-dedicated magnetic resonance imaging (MRI) to highlight hand lesions in patients with rheumatoid arthritis (RA) in comparison with controls. They noted that the second and third metacarpal heads were more often eroded in RA. Bone lesions, morphologically identical with erosions, were also common in controls at the same locations. A similar observation was made by Tan, et al, who linked it to anatomical causes2. The term “lesion” in MRI studies of the joints encompasses bone edema, erosions, and cysts3. According to the OMERACT definition4, an erosion is a sharply marginated bone lesion, of typical juxtaarticular localization and specific signal characteristics, which is visible on 2 planes with a cortical break in at least 1 plane. There is no definition for MRI cyst, but this could possibly correspond to lesions without cortical break, even if their location is central.
Our experience is in agreement that metacarpal heads are a common location of both erosions and cysts. Much attention should be paid to this differential diagnosis by MRI in consideration of their different prognoses. We have recently seen 3 patients with early, undifferentiated arthritis. Two men and a woman complained of metacarpophalangeal (MCP) pain for 2 to 6 months. MRI disclosed large lesions of the third MCP heads. This finding suggested a diagnosis of rapidly progressive, erosive arthritis. IgM rheumatoid factor and anticyclic citrullinated peptide (anti-CCP) antibodies were negative. Turbo 3D T1-weighed MRI showed lesions with cortical break on 3 planes and hyperintense signal on short-tau inversion recovery (STIR) sequences (Figure 1). Because of the large size of these defects, unusual for patients with early disease, computed tomography (CT) was performed to confirm.
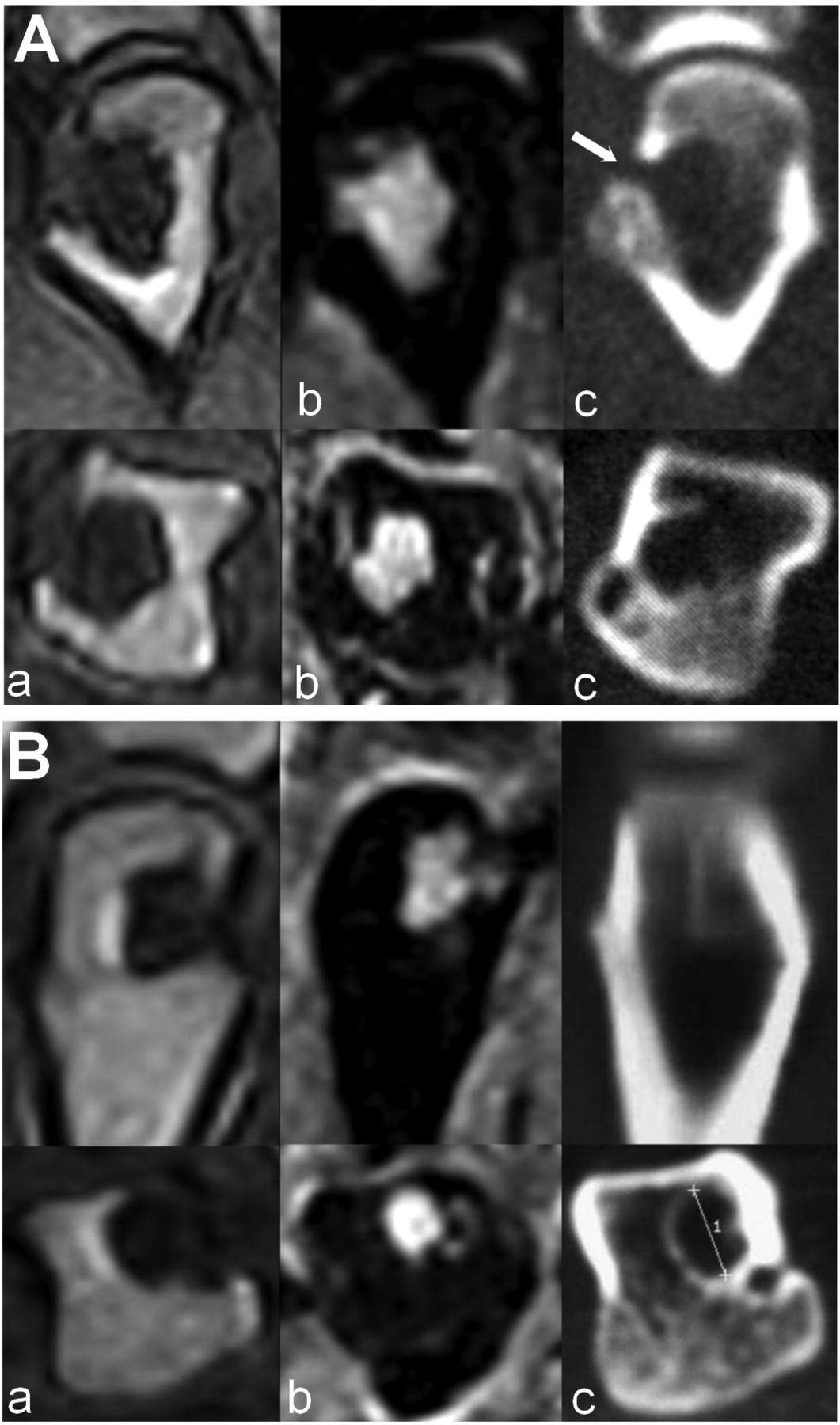
Imaging findings in 2 patients with early arthritis of the metacarpophalangeal joints examined by magnetic resonance imaging (MRI; a, b) and computed tomography (CT; c). A large erosion with cortical break is seen on the MRI Turbo 3D sequence (a). On short-tau inversion recovery images (b), the cortical bone seems to be present, although faint. CT (c) clearly shows the cystic nature of the lesions, although in Patient A a thin interruption of the cortical bone is seen (arrow). The first row shows the coronal images, the second row, the axial images.
CT revealed that these lesions were cysts (Figure 1). In patient A, a thin communication (1.5 mm) through the bone cortex was observed. Because of its small size, it was interpreted as an enlargement of a cortical bone channel5. In the other 2 patients, no cortical disruption was seen. CT is superior to MRI in detecting bone lesions because MRI is unable to image bone per se, but can show only the bone marrow inside. Compact bone, such as that of the cyst wall of our patients, is invisible on MRI. STIR sequences, which suppress fat bone marrow, may be superior to other morphological MRI sequences for correctly interpreting cysts. In fact, compact bone, which is deprived of water and fat, appears black (Figure 1). The followup reflected our interpretation: the patients experienced disease remission after a short period of methotrexate treatment, without the onset of new bone lesions.
In general, MRI is a powerful technique to diagnose erosions because of its multiplanar imaging capability. However, in doubtful cases, careful examination of the STIR image and CT, which represents the gold standard, should be considered. Caution should be used in the diagnosis of erosions, especially in the metacarpal heads. Further prospective studies could evaluate whether cysts are a pre-erosive condition.








{kind=link}