

Abstract
Objective. To characterize the neural circuitry involved in depression associated with systemic lupus erythematosus (SLE), we used single photon emission computed tomography (SPECT) to study regional cerebral blood flow (CBF) in patients with SLE.
Methods. SPECT with 99mTc-ethylcysteinate dimer was performed in 30 depressed women patients with SLE, in 14 women patients with SLE and without history of neuropsychiatric disorders, and in 25 healthy women controls. Magnetic resonance imaging was done for all subjects for diagnostic purposes. Analysis of CBF patterns was performed using statistical parametric mapping. Statistical significance was taken at uncorrected p < 0.001 at cluster level.
Results. There were no significant differences between depressed and nondepressed patients with SLE for any rheumatologic variable. In comparison to healthy controls, depressed patients with SLE had significantly reduced CBF in bilateral frontal and temporal cortex; global maximum was located in the left precentral gyrus. There were no significant CBF differences between nondepressed patients with SLE and controls. Compared to nondepressed patients with SLE, depressed patients with SLE had significantly lower CBF in 2 clusters that had their local maxima in the right precentral gyrus and in the left superior temporal gyrus. The duration of SLE correlated with decreased perfusion in the left middle and superior frontal gyrus.
Conclusion. Depressed patients with SLE have CBF reductions in discrete temporal and frontal regions that may account for depressive symptoms.
Involvement of the central nervous system (CNS) occurs in 20%–75% of patients with systemic lupus erythematosus (SLE) and is a major source of morbidity and mortality1,2. The features of neuropsychiatric SLE vary from global to focal cerebral dysfunction, and include psychiatric disorders as well as central and peripheral neurological disorders. Depression is a particularly frequent psychiatric manifestation in patients with SLE: it may be twice as common as in the general population, and it is associated with an increased risk of attempted suicide1,2,3,4.
Single photon emission computed tomography (SPECT) with cerebral blood flow (CBF) tracers and positron emission tomography (PET) with (18F)fluorodeoxyglucose [(18F)FDG] have demonstrated reduced CBF and reduced cerebral glucose metabolic rate (CMRglc) in various cerebral areas of patients with neuropsychiatric SLE5,6,7,8,9,10,11,12,13,14,15,16. Nevertheless, these studies included patients with different psychiatric disorders as well as neurological disorders. This limitation prohibited investigating the neural circuitries involved in SLE-related depression. Our aim was to investigate CBF changes in depressed patients with SLE using SPECT with 99mTc-ethylcysteinate dimer (ECD).
MATERIALS AND METHODS
We recruited for our study 30 consecutive women patients with SLE (mean age ± SD 42 ± 12 yrs) whose diagnosis of current major depressive episode had been established according to the DSM-IV criteria17. This diagnosis is equivalent to the diagnostic category “mood disorder, major depressive-like episode” of the American College of Rheumatology (ACR)18. Patients were enrolled independently by previous history for recurrent depressive episodes. The psychiatric interview was performed by different senior staff clinicians according to the DSM-IV criteria17 with the aid of a structured clinical interview for DSM-IV. Rating scales for depression were not used. To account for the effect of SLE on CBF6,12,13,16, a second group of 14 patients with SLE who did not have a history of depression or of any neuropsychiatric disorder was recruited (age 43 ± 14 yrs). Patients received standard care for diagnosis and treatment of the disease at the Rheumatology Division of the University of Pisa. All patients were being treated with different combinations of steroids, antimetabolic drugs, and anticoagulants. Patients with depression also received psychotropic drugs, which included selective serotonin reuptake inhibitors, tricyclic antidepressants, and benzodiazepines. Patients were interviewed within 3 days from the scan. Patients with neurological disorders, such as dementia, prior cerebral infarct or hemorrhage, epilepsy, traumatic brain injury, and multiple sclerosis, were excluded. Subjects were asked to refrain from alcohol intake for 24 hours before scanning. Magnetic resonance (MR) fluid-attenuated inversion recovery images (FLAIR) were acquired in all subjects within 1 month from SPECT to exclude cerebral infarct or hemorrhage. The presence of deep white-matter hyperintensities related to chronic subclinical ischemia did not constitute an exclusion criterion14.
Finally, a group of 30 age matched (42 ± 12 yrs) female healthy controls without a history of neuropsychiatric disorders or SLE was recruited. Controls were screened with a review of medical history (including psychiatric interview), physical and neurological examination, Mini Mental State Examination, laboratory examinations, and MR images. No control subject was taking psychotropic drugs or substances known to interfere with brain function. The presence of antiphospholipid antibodies (aPL) and lupus anticoagulant (LAC) antibodies in serum was measured with ELISA. The Ethical Committee of the University of Pisa Medical School approved our study. Written informed consent was signed by all subjects, according to the Declaration of Helsinki.
Clinical characteristics of patients with SLE
Mean age was 36 ± 15 years (range 16–58). Thirteen out of 30 depressed patients had a history of recurrent major depressive episode. In 7 out of these 13 patients, the first major depressive episode occurred before the clinical diagnosis of SLE. Four patients had comorbid generalized anxiety disorder. About 39% of patients had positive aPL serum titers, 43% had positive LAC serum titers, and 21% were positive for both antibodies.
SPECT imaging
In a quiet room with dim light, 728 ± 48 MBq of 99mTc-ECD (Neurolite, Bristol-Myers Squibb) was injected into the ante-cubital vein. Subjects were instructed to keep their eyes closed; ears were unoccluded. SPECT acquisition started 30 min after tracer injection. Scans were performed with a dual-head gamma camera (Optima NT; Elgems, Milwaukee, WI, USA) equipped with low-energy, high-resolution collimators. Raw data were collected in a 128 × 128 matrix (3 mm pixel size) with 128 projections over a 360° circular orbit for each detector (acquisition time, 10 s/step). Energy setting was centered on the 140 KeV peak of 99mTc, with a 20% window. Transverse images were reconstructed with filtered back projection using a Butterworth prefilter and uniform attenuation correction. After reconstruction, images were reoriented along the anterior commissure-posterior commissure line. Reconstructed Dicom 3.0 axial slices were exported to a Windows-based personal computer (Microsoft, Redmond, WA, USA) and converted to the Analyze format using MRIcro.
Image processing and statistical comparison
Subsequent image processing was performed using MATLAB 6.5 (The MathWorks Inc., Natick, MA, USA) and statistical parametric mapping (SPM2; www.fil.ion.ucl.ac.uk/spm/software/spm2). SPECT images were spatially normalized to the SPECT CBF template in the standard stereotactic space of the Montreal Neurological Institute, which approximates the space defined by Talairach and Tournoux19. This procedure involves a 9-measurement linear affine transformation and a nonlinear warping. Images were smoothed prior to statistical analysis with an isotropic 14 mm full height at half maximum Gaussian kernel. Individual counts were normalized to mean global activity by proportional scaling. For all statistical analysis, only pixels with CBF values > 80% of the mean for the whole brain were considered. This approach is used to include only gray-matter pixels in the analysis.
A single-subject analysis was performed to investigate CBF deficits in each patient. First, CBF in each healthy subject was compared to the remainders of the normal group (jackknife analysis) to empirically validate the statistical threshold of the single-subject analysis. Then, each patient with SLE was contrasted to the control group using the validated statistical threshold.
In the group analysis, the effect of the duration of SLE and MR-FLAIR white-matter hyperintensities on CBF20 was assessed with a “single-subject, covariates only” design. Factors with significant effect (uncorrected p < 0.001 at cluster level) were used, in addition to age, as nuisance variables in the subsequent group analysis. Group comparison was performed using the “single-subject, condition and covariate” design, where group belonging was used as a condition. Statistical significance was taken at uncorrected p < 0.001 at cluster level. Clinical and demographic characteristics of the sample were compared with t-test and chi-squared test and statistical significance was taken at uncorrected p < 0.05.
RESULTS
Demographic and clinical characteristics
There were no significant differences between depressed and nondepressed patients with SLE for any demographic or rheumatologic variable. White-matter hyperintensities were present in 31/41 (70%) patients with SLE, without significant group differences between patients with and without depression. White-matter hyperintensities had similar regional distribution in the groups.
Single-subject analysis
No significant CBF abnormality was detected among healthy subjects using a threshold of uncorrected p < 0.05 at cluster level. Thus, this threshold was used for the single-subject analysis. No regional CBF deficit was detected in 9 patients with SLE (3 depressed patients, 6 nondepressed patients). Twenty-seven depressed patients with SLE had regional CBF reductions. CBF deficits were more frequent in depressed patients with SLE than in nondepressed patents with SLE (90% vs 57%, respectively; chi-squared, p < 0.05). In the whole sample, CBF deficits were found in the temporal lobe (64%), frontal lobe (56%), parietal lobe (27%), occipital lobe (18%), thalamus (7%), striatum (3%), and cerebellum (3%).
Correlation with clinical measurements of disease
In the whole sample, a significant (uncorrected p < 0.001) negative correlation between CBF and duration of SLE was detected in the left middle and superior frontal gyrus (Table 1). In the whole sample, there was no significant correlation between white-matter hyperintensities and CBF abnormalities. No significant CBF difference was detected between patients with positive LAC serum titers (n = 17) and patients with negative LAC serum titers (n = 27), between patients with positive aPL serum titers (n = 19) and patients with negative aPL serum titers (n = 25), and between patients positive for both antibodies (n = 9) and the remaining patients (n = 35).
Areas with significant (uncorrected p < 0.001) negative correlations between SLE duration and CBF abnormalities in depressed patients with SLE.
Depressed patients with SLE versus controls
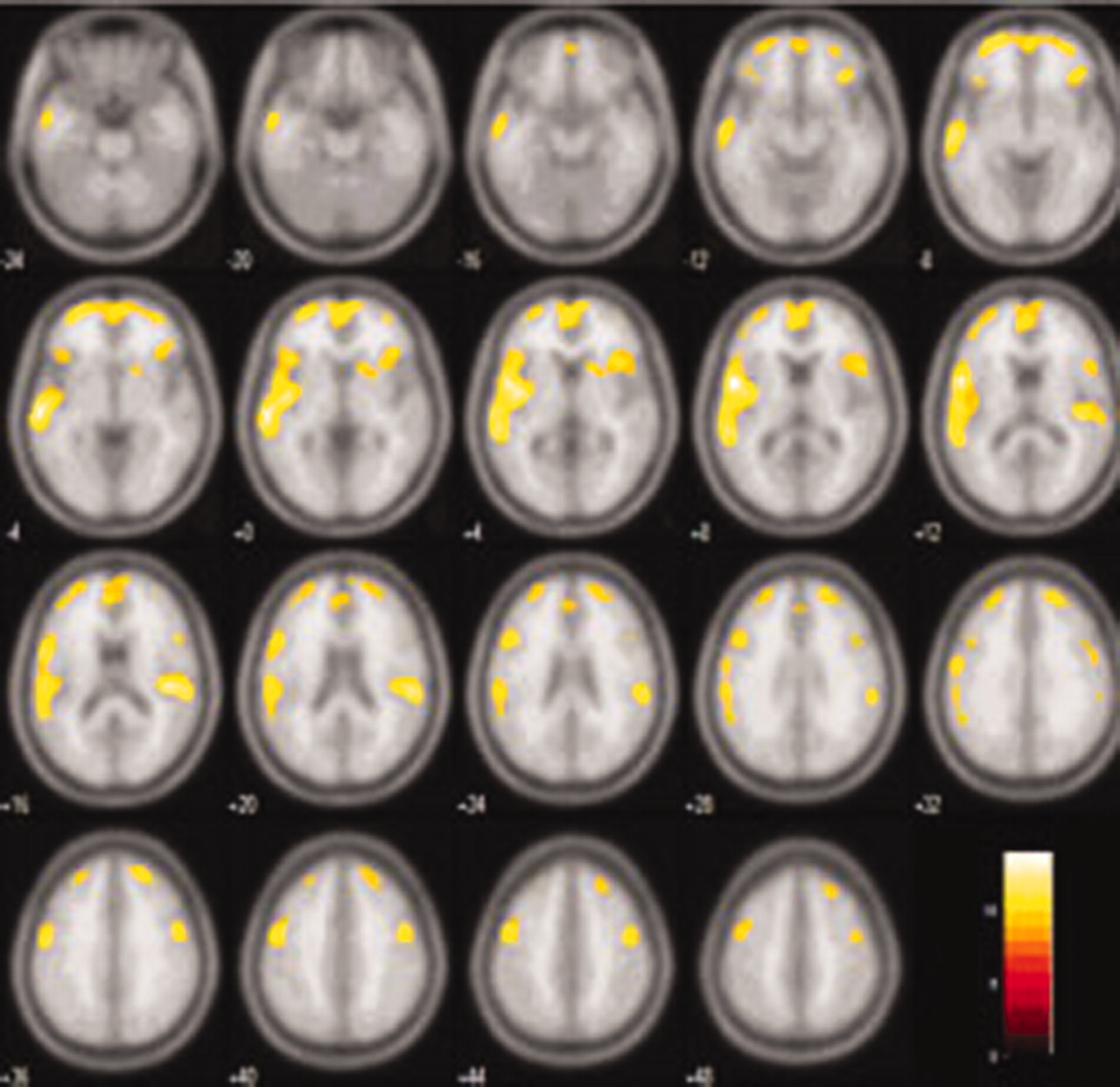
Depressed patients with SLE had significantly reduced CBF in various areas of the frontal lobe, temporal lobe, and insula, and less extensively, in the more anterior part of the parietal lobe (Table 2; Figure 1). Deficits were bilateral, although they were greater on the left side. The greatest CBF group difference was observed in the left precentral gyrus, in close proximity with the left superior temporal cortex and the left insula. Additional sites of peak CBF reduction in depressed patients with SLE compared to healthy controls were found in the right insula and right inferior temporal gyrus, right precentral gyrus, and right postcentral gyrus. CBF reduction was observed also in the bilateral anterior cingulate and lateral prefrontal cortex. There was no significant increase of CBF compared to controls in any cerebral region.

Areas with significant (uncorrected p < 0.001) cerebral blood flow reduction in depressed patients with SLE compared to healthy controls. Numbers at bottom left refer to slice separation from the anterior commissure-posterior commissure transverse plane. The left side of the image refers to the left hemisphere. Numbers in the color bar refer to t-values.
Areas with significant (uncorrected p < 0.001) CBF reduction in depressed patients vs healthy controls.
Nondepressed patients with SLE versus controls
There were no significant CBF differences between nondepressed patients with SLE and healthy controls.
Depressed versus nondepressed patients with SLE
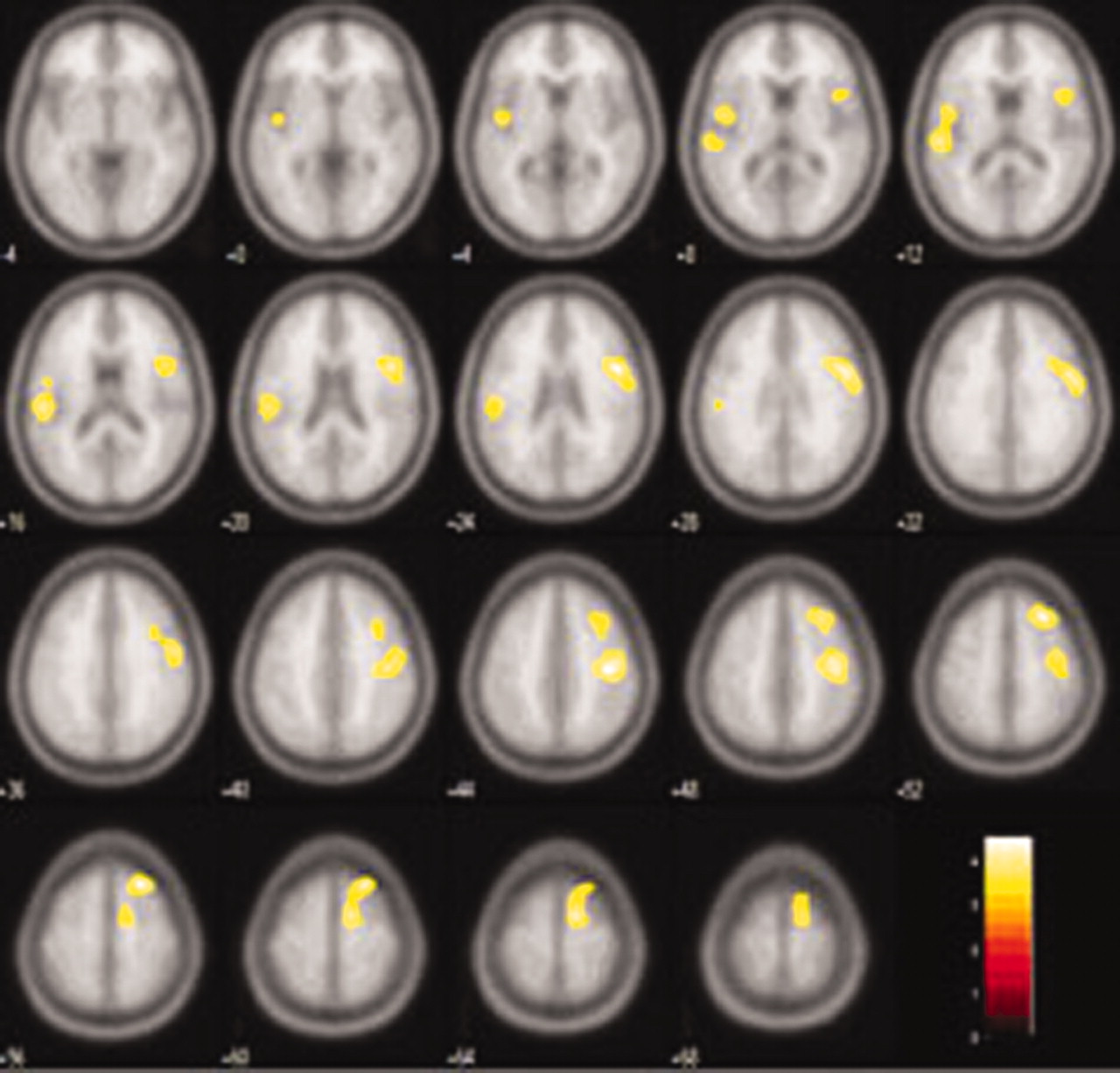
In comparison to nondepressed patients with SLE, depressed patients with SLE had significantly lower CBF in 2 brain clusters: the largest (where group differences were greatest) was located in the right frontal lobe and had 3 local maxima in the right precentral gyrus, in the right inferior frontal gyrus, and in the right middle frontal gyrus. The second cluster was located on the left hemisphere, and peak CBF reductions were detected in the left superior temporal and left precentral gyrus (Table 3; Figure 2). There was no significant increase of CBF compared to controls in any cerebral region.

Areas with significant (uncorrected p < 0.001) cerebral blood flow reduction in depressed patients with SLE compared to nondepressed patients with SLE. Numbers at bottom left refer to slice separation from the anterior commissure-posterior commissure transverse plane. The left side of the image refers to the left hemisphere. Numbers in the color bar refer to t-values.
Areas with significant (uncorrected p < 0.001) CBF reduction in depressed patients with SLE compared to nondepressed patients with SLE.
There were no significant (p > 0.05) differences between depressed patients with recurrent major depressive episodes and patients with first major depressive episode in any brain region.
DISCUSSION
A major debated issue in the SLE field is whether depression associated to SLE should be considered “depression due to a general medical condition” or comorbid “major depressive disorder” (MDD)1,21. The DSM-IV defines depression due to a general medical condition as the presence of depressive symptoms that are judged to be a direct physiological consequence of the medical disease17. Conversely, the diagnosis of MDD excludes the presence of a medical condition that could account for the psychiatric symptoms. More recently, the ACR developed classification criteria for 19 neuropsychiatric syndromes of SLE18. The case definition for mood disorders was largely based on DSM-IV terminology.
To be a direct result of a general medical condition, depression should occur after the onset of the condition, and there should be a plausible pathogenetic mechanism between the 2 conditions. In our sample, the majority of patients experienced their first depressive episode after the onset of SLE, even though 23% of patients had a history of major depressive episode before the onset of SLE. Previous reports indicated that in 12%–49% of patients with SLE, psychiatric symptoms were present before SLE was diagnosed4,22,23.
Several pathophysiological mechanisms can account for neuropsychiatric symptoms in patients with SLE, including immune complex vasculitis, neuron-reactive antibodies, microembolic and macroembolic disease associated with Libman-Sacks endocarditis, thrombosis associated with aPL, ischemic events, corticosteroid treatment, and psychosocial factors14,24,25. Iverson first pointed out that there is generally an implicit and often explicit assumption in the medical literature that psychiatric symptoms in patients with SLE are a direct manifestation of disease pathology. However, there is limited empirical evidence supporting this assumption21.
Ischemic white-matter hyperintensities are frequently found in patients with SLE14,26 and they are strongly associated with late-life depression20. In our sample, white-matter hyperintensities were found with similar frequency in depressed as in nondepressed patients with SLE. A significant relationship was found between white-matter hyperintensities and CBF reductions in patients with MDD, but not in depressed patients with SLE14,20. This observation is consistent with our results indicating no significant relationship between CBF and white-matter hyperintensities.
Another possible explanation for the occurrence of depression in patients with SLE is autoimmunity-mediated brain damage. Sanna, et al found an association between regional CBF reductions and the presence of antiserine protease 3 antibodies11. The same group reported that aPL were independently associated with cerebrovascular disease, headache, and seizures, but not with depressive symptoms27. In our study, no significant relationship was found between CBF and aPL titers or LAC titers. The relation between autoantibody serum concentration and CBF values may vary depending on several factors, including the data analysis approach and the temporal relationship between SPECT imaging and peak activity of disease.
In other chronic diseases, with CNS involvement (e.g., multiple sclerosis) or without (e.g., rheumatoid arthritis), depression is often reported as the most prevalent psychiatric symptom28,29. Such a finding suggests that depressive symptoms are also common in patients with other chronic disabling diseases. Thus, it cannot be excluded that depressive symptoms in patients with SLE are “reactions” to the stresses of the systemic disease.
There is a paucity of information comparing the clinical features of SLE-related depression and MDD. This is because of the lack of studies directly contrasting the 2 conditions21,23. In both cases, women are affected more often. Peak onset is at age 25 to 44 years for MDD and 35 to 44 years for SLE-related depression5,14,17. Suicide attempts are common to both disorders2,3,17. Both causal and merely associative relations between SLE and depression are likely to occur in a large cohort of patients with SLE.
Independent of the nature of the association, it is of interest to assess whether MDD and SLE-related depression share a neural circuitry abnormality that could account for depressive symptoms. Under the general assumption that similar psychopathological symptoms are connected by dysfunction of the same brain areas30, it would be reasonable to predict some overlap in the topography of CBF deficits between SLE-related depression and MDD. Previous SPECT and PET studies on neuropsychiatric SLE did not distinguish depressed patients from patients with other psychiatric and neurological disorders, including schizophrenia, epilepsy, and stroke6,8,11,12,13,31. Some authors distinguished patients with SLE who have major (psychotic) symptoms from those with minor (nonpsychotic) symptoms5,6,14,31,32, while others emphasized the presence or absence of abnormal MR findings5,11,12,13,14,15. CBF deficits were more frequent in patients with major neuropsychiatric symptoms than in patients with minor neuropsychiatric symptoms5,6,14,31,32, and in patients with abnormal MR compared to patients with normal MR results11,12,13,14. Affected brain areas varied among the different studies because of the heterogeneity of the samples. CBF SPECT and (18F)FDG PET were more sensitive than MR for distinguishing areas involved in neuropsychiatric symptoms5,16.
We selected depressed patients with SLE according to DSM-IV criteria. To ascertain the effect of SLE disease activity per se on CBF, we also recruited patients with SLE who did not have depression or any neuropsychiatric disorder, but with similar demographic and immunologic features. By performing such disease-specific comparison, CBF reductions related to the depressive state could be dissociated from CBF reduction related to SLE. After controlling for the effect of SLE, frontal and temporal CBF reductions in depressed patients with SLE were more limited, more prominent in the right hemisphere than in the left, and in the more superior part of the right precentral gyrus, and of the right inferior and middle frontal gyri rather than in the subgenual cortex33. Compared to healthy controls, reduced CBF was found in specific areas of the frontal and temporal cortex in depressed patients with SLE, but not in nondepressed patients with SLE. Altered neural processing, as expressed by reduced CBF, could underlie psychiatric symptoms as well as cognitive deficits reported in patients with SLE1,34,35,36.
Reduced CBF or CMRglc in the frontal lobe of patients with MDD is well established, although results of studies differed substantially in the topography of the involved region. Preferential involvement has been reported for the subgenual prefrontal cortex33, the dorsolateral prefrontal cortex37, the orbitofrontal cortex33,38, and the anterior cingulate cortex37. Temporal and parietal lobes were also involved in MDD, although CBF abnormalities in these brain areas have been replicated less consistently39. Reduction of CBF in the superior temporal cortex, amygdala, and insula was detected in patients with MDD38,40,41,42. Reduced CBF in the left angular gyrus was correlated to psychomotor retardation in patients with MDD43. Although SLE-related depression and MDD may have different pathophysiological mechanisms, our results suggest that the 2 medical conditions might share a final pathway represented by abnormal functioning of a neural circuitry involving frontotemporal areas. This abnormality may contribute to psychiatric symptoms of the depressive state.
Since all patients were taking multiple drugs for treatment of SLE and depression, it is possible that our results are at least partly affected by drugs. Most psychotropic drugs have the capability of affecting CBF either directly or indirectly, but the magnitude of this effect is difficult to quantify37. In patients with SLE, partial or complete recovery of CBF and CMRglc deficits were attributed to the immunosuppressive therapy, although resolution of moderate CBF and CMRglc deficits detected during the acute phase was reported also for untreated patients12,44. Glucorticoids in particular may have introduced a confounding effect. These drugs are known to profoundly interfere with brain metabolism. A generalized reduction in CMRglc in patients with brain tumor taking dexamethasone was found in comparison to other brain tumor patients and normal volunteers45. However, no relationship was found between glucocorticoid dose and CBF deficits46. Treatment with glucocorticoids may also induce psychiatric symptoms in some patients with SLE21. Clinically, the observed pattern of CBF reductions does not indicate that additional immunosuppressive therapy should be administered. Rather, specific treatment with psychotropic drugs should be initiated or titrated according to clinical symptoms.
We enrolled a group of patients with SLE who did not have neuropsychiatric syndromes to control for effects of subclinical SLE on CMRglc. This choice was motivated by the fact that impairment of neuropsychological functions and regional reductions of CMRglc or CBF were reported in up to 28% of patients without clinically evident CNS involvement6,12,13,16,34,35,47. In an alternative approach, we could have neglected the issue of the aspecific changes in CBF due to the systemic disease, and enrolled patients with MDD. This would have allowed a more straightforward comparison of the 2 diseases and direct assessment of the extent that cerebral areas involved in the 2 conditions overlap.
There were limitations in our study. We did not measure disease activity according to standard scales, including the Systemic Lupus Erythematosus Disease Activity Index and the Systemic Lupus Activity Measure-revised. Correlation between such measurements and CBF values would have been helpful to clarify the relation between SLE activity and depressive symptoms. We did not measure some antibodies, such as antiribosomal P antibodies48 and antibodies to N-methyl-D-aspartate receptor49, that have been related to depressive symptoms in patients with SLE.
Reduced CBF in depressed patients with SLE was maximal in the more superior part of the frontal lobe extending to premotor and motor areas. This pattern is not typical of MDD, in which the prefrontal cortex is predominantly affected33. It is possible that differences in PET tracers and 99mTc-ECD, which is sensitive to intracellular and trans-membrane esterase in addition to blood flow50, partially contribute to this finding.
Finally, we used SPECT with statistical parametric mapping for pixel-by-pixel analysis. This approach does not allow absolute measurements of CBF. Other approaches were developed for quantification of brain perfusion with SPECT51. However, these approaches are invasive, time-consuming, and not ideally suited for routine clinical studies. Nevertheless, the absence of quantitative values should be regarded as a limitation of our study.
Depressed patients with SLE had CBF reductions in frontal and temporal areas that partially overlap with areas known to be involved in MDD. Abnormal functioning of the frontotemporal cortex may contribute to psychiatric symptoms of SLE-related depression.
Acknowledgments
The authors thank Cristiana Nisita and the staff physicians of the Psychiatry Department for interviewing the patients, and Mirco Cosottini, Neuroradiology Division, Department of Neuroscience, for reading MR images.
- Accepted for publication April 21, 2010.








{kind=link}
{kind=link}