

Abstract
Objective. In 2005 a large outbreak of Salmonella hadar occurred in Spain following the consumption of commercial precooked roast chicken. We estimated the incidence and risk factors for reactive arthritis (ReA) and other musculoskeletal sequelae in the patients of this outbreak in 2 health departments of Castellon province.
Methods. A prospective cohort study of the patients and their families was carried out. Clinical infection with Salmonella was considered as the exposure factor. The cohort was studied for ReA symptoms using a telephone questionnaire. Telephone interviews or medical examinations of subjects with musculoskeletal symptoms were conducted by a rheumatologist. Robust Poisson regression models were used in the analysis.
Results. From the cohort of 262 people, 248 (94.7%) participated in the telephone survey, 155 with clinical salmonellosis (infected), 78 noninfected, and 15 with some symptoms but not clinical salmonellosis. One hundred one infected patients (65%) reported musculoskeletal symptoms, compared to 19 noninfected (24%) (adjusted relative risk = 2.60, 95% CI 1.73–3.90). Of the infected group, 16 ReA (incidence 10%, 95% CI 6.0–16.2), 7 enthesopathies, and 2 arthralgias were detected, and zero in the noninfected group. The risk factors for ReA were age, weight loss, and duration of diarrhea. Antibiotic treatment for the infection protected against symptoms of peripheral or axial arthritis (adjusted relative risk = 0.73, 95% CI 0.55–0.98).
Conclusion. The incidence of ReA and musculoskeletal symptoms after the infection was high. The use of antibiotics for S. hadar infection offered some protection against musculoskeletal symptoms.
The importance and magnitude of longterm sequelae of intestinal infections have recently been reviewed1,2. These sequelae include inflammatory bowel disease, irritable bowel syndrome, Guillain-Barré syndrome, and reactive arthritis (ReA)3. ReA was defined as “a sterile joint inflammation during or after an infection elsewhere in the body”4. However, DNA or RNA bacteria have been detected in the joints of some patients with ReA5. The clinical spectrum of the disease is extended and no laboratory diagnosis is available. Among the bacteria that can produce ReA, Salmonella is the most frequent etiologic agent of foodborne outbreaks in many countries. After a Salmonella intestinal infection, the incidence of inflammatory joint symptoms may be high in infected patients6,7, and the incidence rate of ReA varies from 5% to 29%8.
During July 2005, a serious foodborne outbreak of S. hadar, associated with the consumption of commercial precooked roast chicken, occurred in Spain; 3451 cases of salmonellosis were reported9,10. To date, this outbreak is the largest registered in Spain for this agent, and it offered the opportunity to investigate epidemiological aspects of ReA, a limited area of research in Spain11.
Castellon was one of the first health departments to establish the cause of the outbreak, which occurred in the last week of July 2005. Our aim was to estimate the incidence and risk factors for ReA and other musculoskeletal sequelae as a consequence of the S. hadar outbreak in the province of Castellon, in the autonomous community of Valencia, Spain.
MATERIALS AND METHODS
A total of 162 patients with clinical salmonellosis associated with the consumption of the roast chicken were reported in 2 health departments in the province of Castellon (500,000 habitants). Examination of fecal cultures of 79 patients revealed 67 positive for S. hadar. Cultures were processed in the microbiology laboratories of the following hospitals: General (Castellon), La Plana (Vila-real), Sagunto (Valencia), and Rey Don Jaime (Castellon). The National Reference Laboratory for Salmonella and Shigella12 identified Salmonella as serotype hadar, phage type 2, resistant to ampicillin, cephalothin, cefuroxime, streptomycin, amikacin, tobramycin, gentamicin, piperacillin, nalidixic acid and tetracycline, intermediately resistant to amoxicillin-clavulanic acid, and sensitive to ciprofloxacin, norfloxacin, cotrimoxazole, cefepime, cefotaxime, cefoxitin, ceftazidime, furantoin and meropenem. The patient with clinical salmonellosis was defined as having developed gastroenteritis (3 or more episodes of diarrhea per day) or fever (≥ 38°C) and vomiting in the 72 hour period after eating a meal that included the commercial precooked roast chicken. “Nonaffected” referred to the person who had no symptoms in the 72 hours after eating a meal that included the chicken. The Epidemiology Division of the Castellon Public Health Center made the study of sequelae of the S. hadar infection in the context of the control and prevention of the S. hadar outbreak.
This was a prospective cohort study. Clinical infection by Salmonella was the exposure factor for ReA. A cohort of 262 people was divided into 2 groups — patients with clinical salmonellosis and probably infected with Salmonella (infected group) and persons with no symptoms (noninfected group). Patients with clinical salmonellosis, but who had not ingested the chicken, were included in the infection group, as possible contact transmission with other family patients was taken into account. Persons who had ingested the chicken but had no symptoms were probably not infected for several possible reasons, including that not all the chickens may have been contaminated with Salmonella, variations in the ingestion of the chicken and interaction with other foods such as alcoholic beverages, or specific immunity in some persons. In order to improve comparability between the 2 groups and to increase the sample size, these individuals were included in the noninfected group, together with those who had not ingested the chicken and had no clinical salmonellosis. Over the 3 month period after the outbreak, a telephone questionnaire survey was carried out by the Epidemiology Division. A specific questionnaire was used to estimate the incidence of joint, mucous, and cutaneous symptoms of infection. This questionnaire was based on one used by the British Columbia Center for Disease Control, Vancouver, Canada, for epidemiological studies of ReA7. The clinical history of hospitalized patients and medical emergency records were consulted to find complementary information. Trained healthcare staff administered the questionnaire. The questionnaires were evaluated by a rheumatologist, and all the participants with some suspected symptoms of ReA, without knowledge of their Salmonella infection status, were invited for a medical examination at the Rheumatology Division, General Hospital, Castellon. If the participant did not attend the examination, principally due to living at a distance, he/she was interviewed again by telephone by the rheumatologist.
Permission and authorization to carry out the study were obtained from the respective health departments. Verbal consent was obtained from each participant or their parents.
The questionnaire gathered information on the following symptoms: joint pain, joint swelling, joint redness or warmth, and with at least one positive symptom: peripheral arthritis; lower back or buttock pain, and with at least one positive symptom: axial arthritis; heel pain or periarticular symptoms of the heel; mouth sores/ulcers, genital sores, red, painful, burning or itching eyes, and with at least one positive symptom: mucous symptoms; rash or other cutaneous symptoms; urethritis (male only): dysuria, penile discharge; and constitutional symptoms: fever, weight loss; new variables were joint symptoms (peripheral arthritis, axial arthritis, or positive periarticular symptoms), mucocutaneous symptoms (positive mucous or cutaneous symptoms) and any symptom (at least one positive symptom). These variables were determined in order to combine the symptoms and were based on self-reported symptoms.
Responses were also recorded to questions about the duration of salmonellosis (number of days from onset until complete recovery), duration of diarrhea (number of days symptom was present), frequency of diarrhea per day, medical attention, hospitalization, antibiotic taken for the salmonellosis, and consultations with a physician for joint symptoms.
ReA was defined following the criteria set out by Hannu and coworkers13: “... development of synovitis (either swelling or limitation of joint movements, and pain) in a previously asymptomatic joint, or as inflammatory low back pain (low back pain worse at night) within the first 2 months after a gastrointestinal infection,” and ReA was considered to be confirmed after examination by the rheumatologist. In the telephone survey by the rheumatologist, if synovitis was suspected, affirmative responses referring to redness, swelling, and pain in a peripheral joint were considered as probable ReA.
The clinical examination by the rheumatologist consisted of a medical history, a thorough physical examination with special attention to signs and symptoms of ReA and other sequelae, and complementary analyses, including blood tests and radiographic examinations.
Statistical methods
The incidence was calculated by dividing the number of cases of ReA and other joint pathologies by the total of patients with clinical salmonellosis assuming a binomial distribution. The Kruskal-Wallis test for continuous variables and chi-square or Fisher test for categorical variables were applied in the comparisons. Relative risk (RR) with a 95% confidence interval (CI) was used to estimate the risk of musculoskeletal and mucocutaneous symptoms in the infected group as compared to the noninfected group, with exclusion of patients with some symptoms but not clinical salmonellosis. Risk factors for ReA were studied in the infected group. Crude RR and adjusted RR (aRR) for various variables were estimated with robust Poisson regression models14, and all models presented a good fit (p > 0.05). Analyses were conducted using Stata® version 9 (Stata Corp., College Station, TX, USA).
RESULTS
The outbreak of salmonellosis occurred in 62 families comprising 262 people and the attack rate was 61.8% (162/262). The disease presented a strong association with the consumption of the chicken: 157 of the patients with clinical symptoms of salmonellosis out of 203 people who had eaten it, versus 2 patients out of 41 people who had not eaten the chicken (RR 15.9, 95% CI 4.1–61.4).
Three months after the outbreak, 248 people were followed up, representing a 94.7% participation rate (248/262). Figure 1 shows the study population, comprising 155 patients with clinical salmonellosis, the infected group (153 had ingested the chicken and 2 had not), and 78 with no symptoms, the noninfected group (44 had ingested the chicken, 34 had not), and 15 with some symptoms that did not respond to the definition of clinical salmonellosis (all had ingested the chicken). Through the telephone questionnaire survey, 101 of the infected group (65.2%) and 19 of the noninfected group (24.4%) reported musculoskeletal symptoms, after a mean of 28 days following the onset of symptoms (range 3–83 days) from the end of clinical salmonellosis in the first group, and a mean of 21 days (range 2–69 days) from the end of clinical salmonellosis in patients of his/her family in the second group. The participants with some suspected symptoms of ReA were invited for a medical examination, 75 in the infected group and 7 in the noninfected group. Forty-six patients in the infected group were given a medical examination, 26 were administered a new telephone survey, and 3 were lost. In the noninfected group, 2 persons were given a medical examination, 2 a telephone survey, and 3 were lost. In the infected group, 13 had confirmed ReA through examination and 3 probable ReA by telephone interview by the rheumatologist, 7 enthesopathies (5 by examination and 2 by telephone interview by the rheumatologist) and 2 arthralgias (all by examination) were detected, and zero in the other group (p = 0.001; p = 0.054; p = 0.541, respectively). Of the probable 3 cases of ReA diagnosed by telephone interview, 1 presented inflammatory lower back pain and 2 synovitis. The incidence rates were 10.3% for all ReA (16/155; 95% CI 6.0–16.2) and considering patients with positive stool culture for S. hadar 9.0% (6/67; 95% CI 3.4–18.5), 4.5% for enthesopathies (7/155; 95% CI 1.8–9.1), and 1.3% for arthralgias (2/155; 95% CI 0.1–9.6).
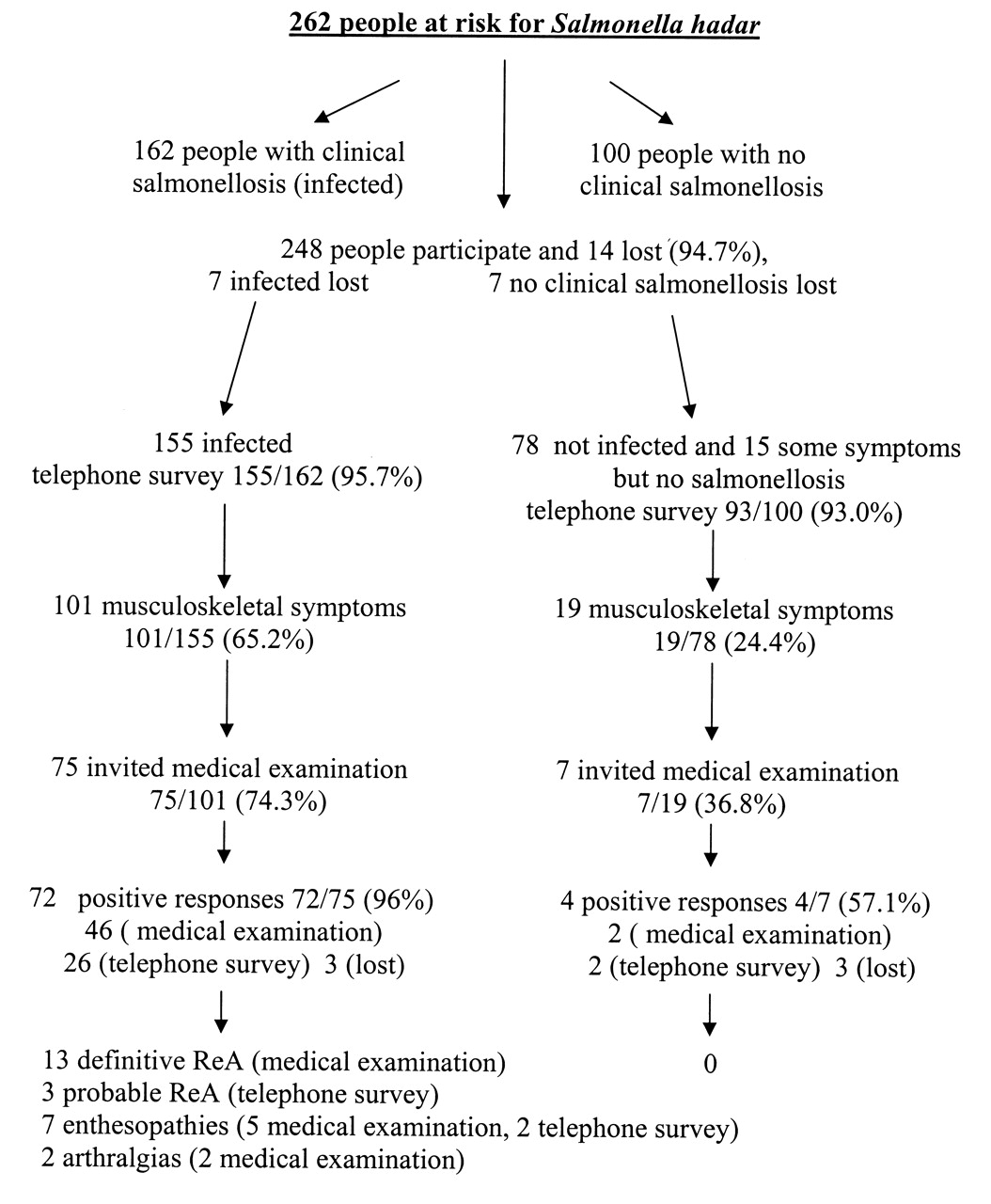
Participation in the cohort study of reactive arthritis (ReA).
Table 1 shows the study population characteristics. No difference by age, sex, or history of rheumatic disease or arthrosis was found. For the patients with clinical salmonellosis, the disease lasted a mean of 9.5 days.
Characteristics of the study population.
The incidence of new musculoskeletal and mucocutaneous symptoms is shown in Table 2. The infected group presented higher incidence of symptoms compared with the noninfected group. The most frequent symptom was joint pain, 50% in the infected group and 17% in the noninfected group (aRR 2.91, 95% CI 1.73–4.91), followed by lower back pain (42% versus 6%, respectively). The highest aRR were for joint swelling (aRR 7.35, 95% CI 1.79–30.11) and lower back pain (aRR 6.31, 95% CI 2.64–15.03). A minor difference between the 2 groups was observed for mucocutaneous symptoms.
Incidence of musculoskeletal symptoms in the study population. Comparison of patients with clinical salmonellosis (infected) and noninfected persons. Relative risk (RR) and 95% confidence interval.
Table 3 shows the comparison of infected and noninfected groups with regard to the incidence of aggregate musculoskeletal and mucocutaneous symptoms. Joint symptoms were reported by 101 of the infected group (65%) versus 19 of the noninfected group (24%) (aRR 2.60, 95% CI 1.73–3.77). At least one symptom was reported by 123 infected (79%) and 28 noninfected (36%) individuals (aRR 2.17, 95% CI 1.60–2.95). The highest aRR was for axial arthritis symptoms (aRR 4.21, 95% CI 2.13–8.31).
Incidence of musculoskeletal and mucocutaneous symptoms in the study population. Comparison of patients with clinical salmonellosis (infected) and noninfected persons. Relative risk (RR) and 95% confidence interval.
Of the 155 patients with clinical salmonellosis, 57 received antibiotic treatment, while 3 patients did not remember whether they had taken antibiotics or not (57/152, 37.5%). Antibiotic treatment distribution was as follows: 44 patients ciprofloxacin (77%), 4 cotrimoxazole (7.0%), 1 amoxicillin (2%), and 1 sulphintestin neomycin (2%). In 7 patients, the antibiotic taken was not known. The 56 patients who had taken antibiotics were compared with the 92 patients who had not, in light of the completed information on adjusted factors (Table 4). The proportion of symptoms was high in both groups, and antibiotic treatment protected against further symptoms, with the exception of mucous symptoms and arthralgias, although there were no significant differences in the crude analysis. In the adjusted analysis, antibiotic treatment was found to be a significant protector for peripheral arthritis symptoms (aRR 0.65, 95% CI 0.46–0.92) and peripheral or axial arthritis symptoms (aRR 0.73, 95% CI 0.55–0.98). In relation to ReA, when antibiotics were taken, the risk of ReA decreased, although it was not significant (aRR 0.43, 95% CI 0.17–1.08).
Reactive arthritis (ReA) and musculoskeletal and mucocutaneous symptom comparisons among patients with clinical salmonellosis in relation to antibiotic treatment during the infection period. Relative risk (RR) and 95% confidence interval.
The cases of ReA, enthesopathies, and arthralgia were compared with the rest of the patients with salmonellosis (Table 5). There were significant differences related to age and severity of the salmonellosis. Patients with ReA were older, with longer duration of diarrhea, longer duration of salmonellosis, and greater weight loss, and sought medical attention for musculoskeletal symptoms. In the infected group, the risk factors for ReA, estimated by a Poisson model from Table 5, were age (aRR 1.03, 95% CI 1.01–1.05), weight loss (aRR 1.15, 95% CI 1.00–1.32), and duration of diarrhea (aRR 1.04, 95% CI 1.02–1.06). For the cases of ReA, the mean period of the onset of symptoms was 19 days (range 4–45 days) after the end of the salmonellosis, and the mean duration was 89 days (range 25–193 days); 3 patients presented symptoms of ReA more than 6 months after the infection. Predominant symptoms were inflammatory lower back pain and inflammatory heel pain, and the most affected joints were knees and ankles.
Comparisons between cases of reactive arthritis, enthesopathies, or arthralgias and the other patients with clinical salmonellosis.
DISCUSSION
Our study revealed an elevated incidence of ReA and musculoskeletal symptoms in the infected group compared with the noninfected group. Use of antibiotics during acute salmonellosis decreased peripheral joint arthritis symptoms, and some protective effect is suggested in the development of ReA.
Most studies of ReA have been made after outbreaks of foodborne gastroenteritis15, and the incidence of ReA following salmonellosis infections had important variations. The causes of the variations include the following: Salmonella serotypes, study design, case definition, methods of study, characteristics of exposed population, and medical attention. In Spain, the incidence of ReA as a consequence of this widespread foodborne outbreak was studied in 5 autonomous communities (Castilla and Leon, Navarra, Galicia, Madrid, Aragon) and the city of Ceuta out of the 17 communities with cases10. A mailed survey based on a Canadian questionnaire16 was used, and the rate of participation was low (32.5%). The incidence of ReA was 15.1% out of 232 clinical cases of salmonellosis. The estimated incidence in our study was lower (10.3%), but a telephone survey was used in addition to a medical examination. In Castellon, the first Spanish study of ReA after a foodborne outbreak of S. enteritidis11 detected a lower incidence of ReA (5%) and musculoskeletal symptoms (32%) than the present study. These data indicate the importance of the problem in light of the high frequency of salmonellosis caused by foodborne outbreaks of gastroenteritis in Spain17, where S. hadar was the third most frequent Salmonella serotype (8.6%), with almost 7000 strains isolated from patients in the period 1997–200118. To our knowledge, only one clinical case of ReA associated with S. hadar has been published19. On the other hand, the detected incidence of ReA was in the middle range of incidence observed in outbreaks caused by different Salmonella serotypes20.
The risk factors associated with the incidence of ReA included several signs of disease severity: the duration of diarrhea and weight loss. Age was also associated with the ReA, and all patients with ReA were over 14 years old, in line with the low incidence of ReA in children21. However, cases of ReA among children have been reported22. Other studies have indicated that the severity of gastroenteritis is related to the incidence of ReA23,24.
The role of antibiotics in the development of ReA is a much debated subject. It is generally accepted that once ReA has occurred no effect of antibiotics can be expected, although with some reservations25. On the other hand, the use of antibiotics before the ReA could be sustained. Hannu, et al20 found that ciprofloxacin treatment during the acute phase of salmonellosis was associated with minor incidence of musculoskeletal symptoms, and this association was observed in other studies7,11, although without becoming significant. However, some studies found no differences26,27 or found that the use of antibiotics increased the incidence of ReA28. A recent study3 indicated no effect of antibiotics on new rheumatic symptoms following enteric bacterial infections after adjusting for age and sex. The use of antibiotics is related to the severity of salmonellosis, and this severity is associated with the incidence of ReA; therefore it is important to control for severity when estimating the effect of antibiotic treatment. In the study, the use of antibiotics protected against symptoms of peripheral or axial arthritis after adjustment for signs of salmonellosis severity (weight loss and duration of diarrhea). In relation to ReA and antibiotic treatment, the study had a limited power to detect significant differences, but some protective effect was observed. However, considering the observational design of this study, these effects should be interpreted with some caution.
The most commonly used antibiotic was ciprofloxacin, which appeared to lead to a decrease in joint symptoms. Hannu, et al29 indicated that ReA could be considered a postinfection sequela of gastrointestinal infection, and the use of antibiotics could be recommended when the patient with the Salmonella infection had a history of ReA. However, it has been indicated3 that use of antibiotics could increase the fecal carriers of Salmonella, and theoretically the risk of ReA. However, the complexity of the situation, including patient background (genetics, HLA-B27 status, age, history of Salmonella infections, etc.), antibiotic used (type, doses, duration, start date, etc.), agent (serotype, antibiotic resistance, inoculum size, virulence, etc.), and other unknown factors, makes it difficult to establish the true effect of antibiotics on the development of the ReA.
Our study presented a high participation rate and the use of a noninfected group allowed the RR of musculoskeletal and mucocutaneous sequelae to be calculated. The telephone survey was completed with a medical examination to reduce information bias. The questionnaire we used had previously been validated in Canada7. Adjusted RR were estimated by controlling for potential confounders using robust Poisson regression models.
Our study has several limitations. There was no laboratory diagnosis of ReA and the report of symptoms was somewhat subjective. The questionnaire asked about new symptoms, but some patients may have reported exacerbations rather than new symptoms. The medical examination by the rheumatologist was more objective, since investigations and additional tests were included. Some reporting bias of symptoms could have occurred, considering that patients received economic compensation from the producers of the precooked roast chicken. Recall bias may also have been present due to the time lapse between the date of symptoms and the date of the questionnaire survey. In items such as antibiotic treatment, some information was lost. There may have been misclassification bias regarding the clinical infection, considering that persons without symptoms (noninfected) could have had Salmonella infection if they had consumed the chicken. Therefore, the reporting of musculoskeletal symptoms could be high in the noninfected group, because asymptomatic but infected persons had reported joint symptoms3. In addition, patients’ genetic characteristics were not studied30,31.
Some aspects of ReA deserve new research, including the effect of antibiotics, the risk factors, and the longterm followup of patients. The study of sporadic cases of salmonellosis and the estimate of incidence of ReA would be of special interest32.
We found that the incidence of ReA and musculoskeletal symptoms was high following S. hadar infection. The use of antibiotics for S. hadar infection could protect against musculoskeletal symptoms.
Acknowledgments
We thank the families and patients affected by the S. hadar outbreak for their cooperation in making this study possible. We are grateful to Dr. Jane Buxton from the British Columbia Center for Disease Control Society in Vancouver, Canada, and Dr. Leena Mattila from the Department of Medicine, Division of Infectious Diseases, Helsinki University Central Hospital in Helsinki, Finland, for help in preparing the study.
- Accepted for publication March 26, 2010.








{kind=link}