

Abstract
Objective. Giant cell arteritis (GCA) is a complex polygenic disease in which more than 1 genetic locus is likely to contribute to disease susceptibility and clinical expression. BANK, an adaptor molecule, has been suggested to participate in the B cell antigen receptors-mediated calcium homeostasis. We assessed for the first time the implication of BANK1 functional variants in susceptibility to GCA.
Methods. Two hundred twenty-two patients with biopsy-proven GCA and 534 matched controls were assessed. DNA from patients and controls was obtained from peripheral blood. Samples were genotyped for 3 putative functional BANK1 gene polymorphisms (rs17266594 T/C, rs10516487 G/A, rs3733197 G/A) using a TaqMan allele discrimination assay.
Results. No significant differences were observed in genotype distribution between patients with biopsy-proven GCA and controls for these 3 gene polymorphisms. A trend for a decreased risk of having GCA was observed in individuals carrying the BANK1 rs3733197 GG genotype (patients with GCA 43.9% compared to 51.6% in controls; p = 0.06, OR 0.73, 95% CI 0.53–1.02). The frequency of BANK1 rs3733197 allele G was marginally decreased in patients with biopsy-proven GCA compared to controls (p = 0.09, OR 0.82, 95% CI 0.64–1.04). Haplotype analysis of 3-single-nucleotide polymorphisms found no statistically significant differences between patients with GCA and controls. No significant differences for the BANK1 gene polymorphisms were found when patients were stratified according to specific clinical features of the disease.
Conclusion. Our results do not support a major implication of the BANK1 locus in susceptibility to GCA.
Giant cell arteritis (GCA) is the most common vasculitis in the elderly in Western countries1. This granulomatous vasculitis involves large and medium-size arteries derived from the aorta, in particular the cranial branches of the carotid artery2. Evidence supports a strong genetic component for GCA3–5.
It has been suggested that BANK, an adaptor molecule, participates in B cell antigen receptors-mediated calcium homeostasis6. Association has been described between several variants within the B cell scaffold protein with ankyrin repeats (BANK1) gene and systemic lupus erythematosus (SLE)7. BANK1 is specifically expressed in B cells, and seems to be involved in B cell receptor-mediated activation6,8.
We assessed the implication of BANK1 functional variants in the susceptibility to biopsy-proven GCA. We selected the following 3 putative functional BANK1 gene polymorphisms: the BANK1 rs10516487 single-nucleotide polymorphism (SNP) leads to a substitution of arginine by histidine at position 61 (R61H) of the BANK-1 protein, which lies within the region essential for the binding of IP3R; the BANK1 rs3733197 SNP leads to an alanine to threonine substitution at position 383 (A383T) in exon 7, which encodes the ankyrin repeat–like motif; and the BANK1 rs17266594 SNP (branch-point variant) may affect the relative splicing efficiency, but not splicing per se, of the full-length and Δ2 isoforms of BANK1.
MATERIALS AND METHODS
Patients
Two hundred twenty-two patients diagnosed with biopsy-proven GCA between 1991 and 2007 were initially included in our study. Clinical information about this series of patients has been reported9. A control population (n = 534) matched by age, sex, and ethnicity with patients with GCA was also studied. Patients and controls were included in this study after providing written informed consent. Ethical committee approval was obtained.
All patients with GCA had a positive temporal artery biopsy10. Patients with GCA were considered to have polymyalgia rheumatica (PMR), visual ischemic manifestations, or severe ischemic complications in the context of GCA if they fulfilled established definitions11,12.
SNP genotyping
Genomic DNA was extracted from peripheral blood. The rs17266594, rs10516487, and rs3733197 polymorphisms of the BANK1 gene were genotyped as reported13.
Statistical analysis
Odds ratios and 95% CI were calculated according to Woolf’s method using the Statcalc program (Epi Info 2002, Centers for Disease Control and Prevention, Atlanta, GA, USA). Haploview software (Broad Institute, Cambridge, MA, USA) was used to obtain linkage disequilibrium pairwise values. Haplotypes were constructed with the expectation maximization algorithm implemented in the Unphased software package (F. Dudbridge, Medical Research Council Human Genome Mapping Project Resource Centre, Hinxton, UK). P values < 0.05 were considered statistically significant.
RESULTS
A genotyping success rate > 96% was achieved in patients with GCA and controls. No evidence of departure from Hardy-Weinberg equilibrium was observed in controls. The estimated power of this study for an estimated OR between 1.5 and 2.0 was 72%–99%, for a type I error rate of 0.05. No significant differences in the genotype distribution between patients with GCA and controls for these 3 gene polymorphisms were observed (Table 1). A trend for a decreased risk of having GCA was observed in individuals carrying the BANK1 rs3733197 GG genotype (43.9% in patients with GCA vs 51.7% in controls; p = 0.06, OR 0.73, 95% CI 0.53–1.02; Table 1). The frequency of the BANK1 rs3733197 allele G was also marginally decreased in patients with GCA (65.9%) compared to controls (70.3%; p = 0.09, OR 0.82, 95% CI 0.64–1.04; Table 1).
BANK1 gene polymorphisms in patients with giant cell arteritis (GCA) and healthy controls.
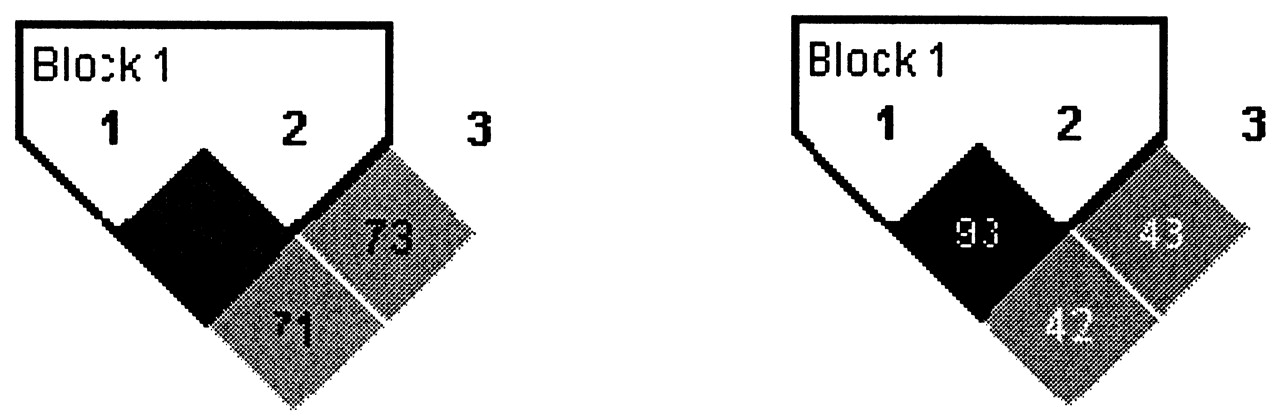
Allelic frequencies for the 3 SNP were similar to those found in other populations7,13. SNP rs10516487 and rs17266594 were in strong linkage disequilibrium (D’ 0.97; r2 = 0.94), since they are separated by 153 base pairs. These 2 markers lie on a linkage disequilibrium block spanning 21 kilobase pairs (kbp) within the BANK1 gene. Linkage disequilibrium between rs3733197, which is located in a different linkage disequilibrium block that encompasses 57 kbp of the BANK1 gene, and r10516487s (D’ 0.73; r2 = 0.42) and rs17266594 (D’ 0.71; r2 = 0.44), respectively, was less strong, since they are 88 kbp apart (Figure 1). In addition, we performed a haplotype analysis of 3 SNP according to the method of Gabriel, et al14. However, we found no statistically significant differences between the patients and controls (Table 2).

Linkage disequilibrium between the 3 BANK1 single-nucleotide polymorphisms (SNP) in the study population. SNP 1 is rs17266594, SNP 2 is rs10516487, SNP 3 is rs3733197.
Frequencies of the most common (> 5 %) haplotypes formed by BANK1 single-nucleotide polymorphism (SNP) in patients with GCA and healthy controls. SNP of the 2-SNP haplotype are rs17266594 and rs10516487, and those of the 3-SNP haplotype are rs17266594, rs10516487, and rs3733197.
No significant differences for the BANK1 gene polymorphisms between patients with GCA with or without PMR, visual ischemic manifestations, or severe ischemic complications were found (data not shown).
DISCUSSION
Our study constitutes the first attempt to determine the potential influence of 3 BANK1 gene polymorphisms (rs17266594 T/C, rs10516487 G/A, rs3733197 G/A) in the susceptibility to GCA using the largest series of patients with biopsy-proven GCA ever assessed for genetic analysis. Our results do not support a major implication of these gene polymorphisms in susceptibility to GCA or in the phenotypic expression of this vasculitis. However, GCA is a relatively uncommon disease and our cohort is probably underpowered for the detection of an association.
In a recent study, Orozco, et al analyzed the potential role of BANK1 gene polymorphisms in the genetic susceptibility to rheumatoid arthritis (RA), using 4 different populations15. The study confirmed that rs17266594 and rs10516487 are in strong linkage disequilibrium. The BANK1 gene variants rs10516487 and rs3733197 were associated with RA with a low effect15. In keeping with our results in GCA, Orozco, et al did not find statistically significant differences in allele and genotype frequencies for the rs10516487 and rs17266594 BANK1 polymorphisms in the Spanish population, when patients with RA were compared with controls. In addition, in the pooled analysis the effect sizes at the BANK1 locus found for RA were very modest for rs10516487 and rs3733197. These results suggest that the effect of these BANK1 polymorphisms in RA susceptibility may be less important than that seen in SLE7.
In keeping with results reported in RA, the pathogenic effect of autoantibodies in the development of GCA seems to be less important than it is in SLE. That may explain our negative results in terms of the minimal effect of mechanisms leading to an impaired B cell activity in the pathogenesis of GCA.
Footnotes
- Accepted for publication February 3, 2010.








{kind=link}