

Abstract
Objective. To assess possible correlations between endothelial-dependent flow-mediated dilation (FMD) of the brachial artery and nailfold videocapillaroscopy (NVC) in patients with systemic sclerosis (SSc). Evidence has shown that vascular impairment in SSc may be a sign of endothelial dysfunction involving both microvascular and macrovascular systems, although the pathological mechanisms of the dysfunction are poorly understood.
Methods. Forty-three consecutive patients (mean age 51 ± 11 yrs) with SSc were studied. Thirty patients had limited cutaneous SSc, 13 had diffuse cutaneous SSc. Twenty-seven healthy subjects (mean age 48 ± 8 yrs) were recruited as controls. Ultrasound assessment of FMD was performed on all subjects in order to evaluate macrovascular function. Patients were divided into 3 patterns of microvascular damage on the basis of NVC (early, active, and late), and the microangiopathy evolution score was calculated, as reported elsewhere.
Results. FMD was significantly reduced in patients with SSc compared to healthy subjects [median 8.0% (3.0%–9.0%) vs 15.0% (12.0%–16.0%), respectively; p < 0.0001]. Patients with an early pattern of microangiopathy showed reduced FMD values compared to controls (p = 0.0001). FMD was significantly reduced in patients with SSc who had the late NVC pattern of microangiopathy compared to active and early patterns (p = 0.003 and p = 0.001, respectively). FMD was inversely correlated with the microvascular damage rate in patients with SSc (p < 0.0001).
Conclusion. We demonstrated the simultaneous presence of macrovascular and microvascular impairment in patients with SSc, which was already present in the early phase of the vascular disease.
Systemic sclerosis (SSc) is a clinically heterogeneous disease characterized by disturbances of the immune system and massive deposition of collagen and other extracellular matrix proteins in the connective tissue of the skin and internal organs1. Vascular impairment is one of the main features in the pathogenesis of SSc and it is detectable in the early phase of the disease. It has recently been hypothesized that the endothelial injury can explain the pathogenesis of the vascular lesions, even if the pathological mechanisms of the dysfunction are poorly understood2. Raynaud’s phenomenon (RP), together with capillary morphological abnormalities, is the most common and earliest finding of SSc and can be considered the main expression of microvascular dysfunction3. Nailfold videocapillaroscopy (NVC) is a simple technique that is useful in the early identification of microvascular involvement in patients with SSc. Recently, attempts have been made to identify disease-specific capillary abnormalities, as well as to define specific capillaroscopy patterns of microangiopathy in order to assess the progression of the microvascular damage in patients with SSc4,5.
Structural histopathological changes in the wall of arterioles, such as intimal proliferation, intimal and medial hypertrophy, and disruption of the internal elastic lamina, are well recognized in SSc6. But few data are available regarding the functional changes of small elastic conduit arteries, such as brachial and radial arteries. Recent evidence has shown that SSc vascular impairment may be a sign of endothelial dysfunction involving both microvascular and macrovascular systems7,8.
Ultrasound assessment of brachial artery endothelial-dependent flow-mediated dilation (FMD) is a noninvasive instrumental evaluation that is routinely performed as an index of macrovascular function. This technique, described by Celermajer, et al in 19929, measures brachial artery diameter before and after an ischemic stimulus, and shows the vasodilatory response to blood flow-associated shear stress increase. Forearm ischemia causes a marked drop in peripheral resistance, followed by an increase in wall shear stress in the conduit artery after the release of ischemia. Shear stress increase stimulates both endothelial production and the release of several vasodilators, primarily endothelial nitric oxide (NO). The resulting augmentation of arterial diameter, expressed as percentage of increase, estimates the NO release and, vicariously, the endothelium-dependent vasodilatation. Thus, a small percentage of FMD response is interpreted as low NO bioavailability and is associated with an increased risk of vascular disease10.
Our study was designed to assess the possible involvement of macrovasculature dysfunction in SSc, as well as the correlations between macrovascular and microvascular impairment.
MATERIALS AND METHODS
Patient population
Forty-three consecutive patients were studied (37 women and 6 men, mean age 51 ± 11 yrs). They were diagnosed as having SSc as defined by the American College of Rheumatology criteria11 and were referred to the Academic Units of Clinical Rheumatology and Immunology of the University of Genoa. Thirty patients (mean age 51.0 ± 11.7 yrs) had limited cutaneous SSc (lcSSc) and 13 (mean age 50 ± 9.5 yrs) had diffuse cutaneous SSc (dcSSc)12. All enrolled patients reported the presence of RP. Age at onset of both SSc and RP was investigated in all patients. The duration of SSc at the time of study entry was evaluated by clinical interview and/or from clinical file data. In particular, the duration of SSc was calculated from the time of the first complaints of clinical signs or symptoms clearly related to SSc, or from the time of instrumental and/or serological examinations specific for SSc.
All of the 43 enrolled patients were treated with vasodilators and/or calcium channel blockers. One month of washout from these drugs was done prior to carrying out cardiovascular examinations. A few patients taking nonsteroidal antiinflammatory drugs were banned from taking them in the 30 days before the study. Exclusion criteria included history of cigarette smoking, diabetes mellitus, hypercholesterolemia, cancer, heart and pulmonary failure, myocardial infarction, and angina pectoris. Twenty-seven healthy subjects (20 women, 7 men, mean age 49 ± 8 yrs) were recruited as controls. Informed consent was obtained from all patients and controls before entry into the study. The local ethics committee approved the study. FMD and NVC assessment were performed on all subjects.
Electrocardiography and echocardiography
Surface electrocardiography (ECG) and transthoracic echocardiography were performed on all subjects. All echocardiographic studies were performed using a high-resolution ultrasonographic scanner, C512 Acuson Sequoia (Siemens Medical Solutions Inc., Mountain View, CA, USA) equipped with a 1.0–4.0 MHz wideband multihertz imaging probe (4V1c). The overall monodimensional left ventricular measurements and the bidimensional (apical, 4-chamber, and 2-chamber) views were obtained according to the recommendations of the American Society of Echocardiography13.
FMD in the brachial artery
All assessments were performed by the same operator in an air-conditioned room at 21–24°C, after overnight fasting and following a 30-min rest. Heavy foods, including high-fat foods and caffeine-containing beverages, were prohibited the night before the study.
Ultrasound scans were performed using the C512 Acuson Sequoia, equipped with a 5.0–8.0 MHz linear wideband multihertz imaging probe (8L5).
The brachial artery was scanned over a longitudinal section 2–3 cm above the antecubital fossa, based on individual anatomical variability. When an adequate image was obtained, the ultrasound probe was positioned using a mechanical probe stabilizer. After baseline measurements of brachial artery diameter, the pressure cuff was kept inflated for 5 min at 50 mm Hg over systolic blood pressure on the proximal portion of the forearm, as reported14. No patients experienced significant discomfort during or after cuff occlusion.
Postischemic artery diameter recording was started 30 s before rapid deflation of the blood pressure cuff and the longitudinal image of the artery was recorded continuously for up to 4 min. FMD was expressed as percentage of increase in arterial diameter from baseline to the postocclusive period. Ultrasound images were analyzed offline by averaging the arterial diameter along 10 mm segments. Diameters from 3 consecutive end-diastolic frames (identified by the electrocardiographic R wave) were averaged to yield the brachial artery diameter during the respective experimental stages. The intraoperator variability was 3.8%. FMD measurements were blindly performed with respect to the NVC evaluation.
Nailfold videocapillaroscopy
Morphological evaluation of skin capillaries is generally performed at the nailfold because this area is easily accessible for examination, and because the major axis of the capillaries is parallel to the skin surface (in other areas, it has a perpendicular status).
The same operator performed all the NVC using a videocapillaroscopy optical probe equipped with a magnification ×200 contact lens and connected to image analysis software (Videocap, DS MediGroup, Milan, Italy). Each subject was in the test room for a minimum of 15 min before the nailfold examination, and the room temperature was 20–22°C. The nailfold (distal row) of the 2nd, 3rd, 4th, and 5th fingers was examined in each patient.
Based on the NVC abnormalities, the patients with SSc were classified by the most appropriate NVC pattern15. The patterns included (1) “early” pattern: few giant capillaries (< 4 altered capillaries per mm), few capillary hemorrhages, relatively well preserved capillary distribution, no evident loss of capillaries; (2) “active” pattern: frequent giant capillaries (> 6 altered capillaries per mm), frequent capillary hemorrhages, moderate loss of capillaries (20%–30%), mild disorganization of the capillary architecture (4–6 altered capillaries per mm), absent or mild ramified capillaries; and (3) “late” pattern: irregular enlargement of the capillaries, few or absent giant capillaries and hemorrhages, severe loss of capillaries (50%–70%) with large avascular areas, disorganization of the normal capillary array, and evident ramified capillaries15.
The following capillaroscopic measurements were taken into consideration, as they were found to correlate with progression of the nailfold microangiopathy, as described: loss of capillaries, disorganization of the microvascular array, and capillary ramifications4,5. A semiquantitative rating scale to score each capillary abnormality was adopted according to previous studies (0 = no changes; 1 = less than 33% of capillary alterations/reduction; 2 = 33%–66% of capillary alterations/reduction; and 3 = more than 66% of capillary alterations/reduction, per mm)5. The mean score value for each capillaroscopic measurement was calculated from the analysis of 4 consecutive fields (1 mm for each) in the middle of the nailfold of each digit; the average score values of the 8 digits were added together, and the final value was divided by 8. The resulting value represented the score for each capillaroscopic measurement that was analyzed. The scores of these measurements were added together to globally assess the variation of the SSc microangiopathy over time [microangiopathy evolution score (MES): 0–9]. The intraoperator variability was 3%. NVC measurements were blindly performed with respect to the FMD evaluation.
Autoantibody detection
Serum antinuclear (ANA), antitopoisomerase I (Scl-70), and anticentromere (ACA) antibodies were investigated in all patients. ANA were detected by indirect immunofluorescence using HEp-2 cells as substrate (Euroimmun, Luebeck, Germany). ACA and Scl-70 were measured using an enzyme-linked immunosorbent assay (ELISA; Euroimmun).
Statistical analysis
Results are expressed as median and 25th–75th percentiles. The Kruskal-Wallis test was used to assess differences among the distributions of variables, as appropriate. The Mann-Whitney U test was used to compare continuous variables with nominal variables. Regression tests were used to evaluate any possible relationship between continuous variables as well as the Spearman’s rank correlation test. A p value ≤ 0.05 was considered statistically significant.
RESULTS
Clinical characteristics
Characteristics of patients and controls are summarized in Table 1. None of the patients had signs or symptoms of cardiovascular disease. Sinus rhythm but no other major abnormalities were found at ECG in all subjects. All echocardiographic measurements were within the normal range13. Left and right ventricular function was normal and no pericardial effusion was detected in any of the subjects. Systolic pulmonary pressure, determined by the peak flow velocity of the tricuspid regurgitation, was normal in all patients (< 40 mm Hg)16.
Clinical characteristics of the patients with SSc and controls. Data are expressed as mean ± SD or percentage.
No major differences were observed between patients with SSc and healthy controls in means of height, weight, systolic and diastolic blood pressure, resting heart rate, brachial artery diameter, or levels of low-density or high-density lipoprotein cholesterol. Serum ACA and Scl-70 were positive in 18 (48.6%) and 8 patients with SSc (21.6%), respectively (Table 1).
Vascular evaluation
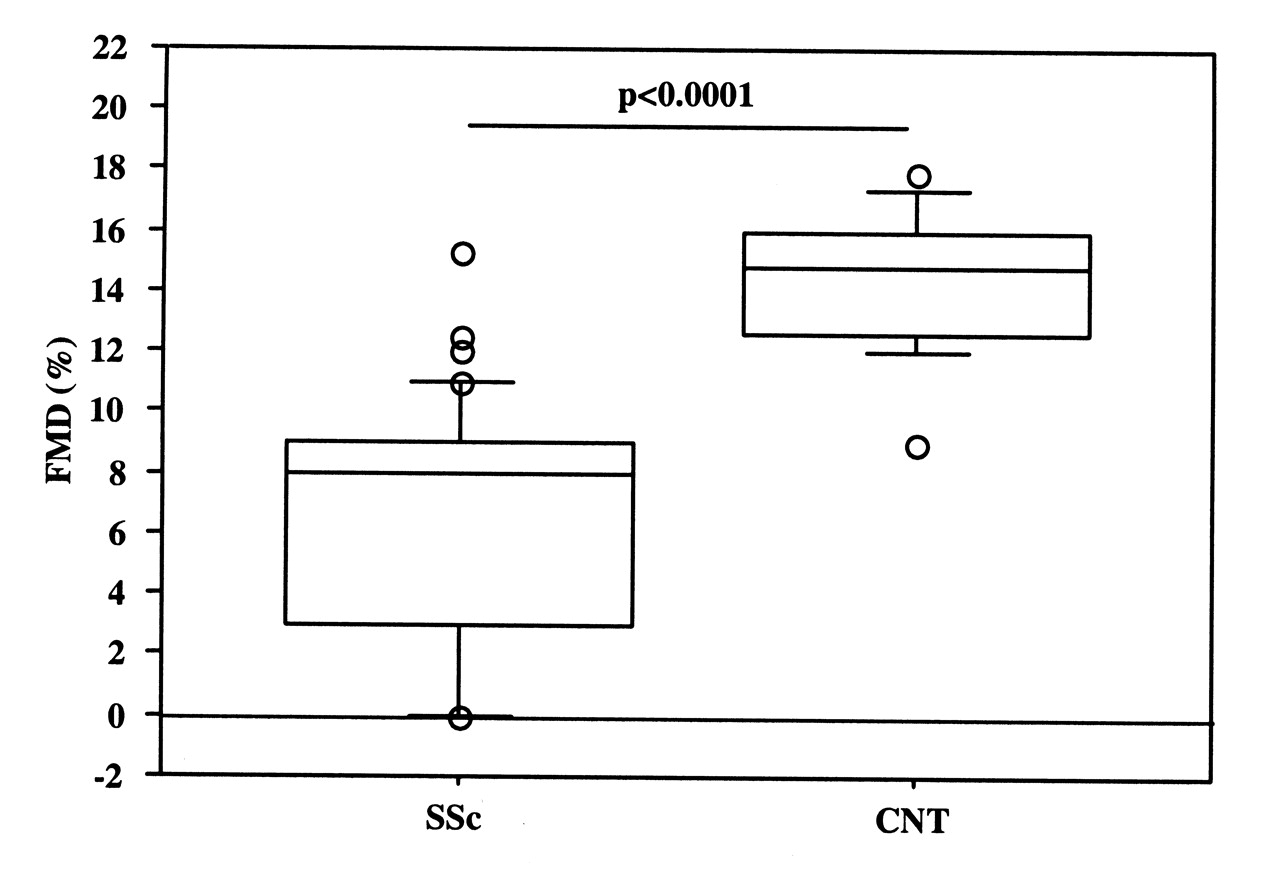
All enrolled patients showed a scleroderma pattern of microangiopathy at NVC examination: early NVC pattern was found in 13 patients, active pattern in 15 patients, and late pattern in 15 patients. FMD was significantly reduced in patients with SSc compared to healthy subjects [median 8.0% (25th and 75th percentiles 3.0–9.0) vs 15.0% (12.0–16.0), respectively; p < 0.0001; Figure 1]. Notably, patients with SSc who had the early pattern of microangiopathy showed lower FMD values than the healthy controls (p = 0.001). Further, FMD was significantly reduced in patients with SSc who had the late NVC pattern compared to the active and early patterns [median 3.0% (0.5–5.8) vs 8.6% (3.2–10.0) and 9.0% (6.1–10.1); p = 0.003 and p = 0.001, respectively; Figure 2]. Microangiopathy evolution score was significantly different in patients with SSc in all 3 NVC patterns of microangiopathy [median 0.0 (0.0–2.0), 3.0 (2.7–4.2), and 6.0 (6.0–8.0), respectively (p < 0.0001)]. A negative correlation between FMD and MES was found in patients with SSc (p < 0.0001; Figure 3). No statistically significant difference concerning FMD values, MES, and NVC patterns was found between patients with lcSSc and those with dcSSc.

Flow-mediated dilation (FMD) in patients with SSc and in healthy controls (CNT). Data are given as 5th, 10th, 50th (median), 90th, and 95th percentiles.

Flow-mediated dilation (FMD) in patients with SSc with different nailfold videocapillaroscopy patterns of microangiopathy (early, active, and late). Data are given as 5th, 10th, 50th (median), 90th, and 95th percentiles.

Inverse correlation between flow-mediated dilation (FMD) and microangiopathy evolution score (MES), as evaluated by nailfold videocapillaroscopy.
DISCUSSION
In our study we showed a significant, blunted macrovascular response at FMD evaluation in patients with SSc who were asymptomatic for cardiovascular diseases as compared to healthy subjects. This is the first study to report that FMD is already reduced in patients with SSc with the early pattern of microangiopathy, and that lower FMD values are found in patients with the late NVC pattern of microangiopathy compared to those with the active and early patterns. Moreover, a significant, inverse correlation between FMD values and the rate of microvascular damage was found in patients with SSc.
Vascular dysfunction is a key element of SSc pathogenesis, and it occurs in almost all patients with SSc. Functional and structural changes may occur in microvessels, digital arteries, and sometimes even in the more proximal vessels of these patients17. Peripheral impairment in SSc can be caused by several things, e.g., abnormalities of neuroendothelial control mechanisms; structural abnormalities of the vasculature involving both microvessels and the digital arteries; and intravascular factors, including a procoagulant tendency and increased oxidative stress17. Structural changes affect both peripheral capillaries, which can be carefully studied by NVC, and digital arteries, in which the most characteristic histologic lesions are marked intimal hyperplasia and fibrosis4,18,19.
NVC microvascular impairment in SSc is characterized by the early detection of giant capillaries, followed in the advanced stages by capillary reduction, neoangiogenesis, and disorganization5,14,20. Three distinct NVC patterns of microangiopathy (early, active, and late) have recently been identified and are useful for evaluating the stage and severity of microvascular damage in SSc5. On the other hand, 3 capillaroscopic measurements (loss of capillaries, disorganization of the microvascular array, and capillary ramifications) were found to correlate with progression of the microvascular damage in SSc, and a composite score has been proposed to monitor microvascular evolution5. Our study proves that macrovascular impairment is already present in the early phase of SSc microangiopathy as demonstrated by the reduction of FMD in patients with the early NVC pattern, which becomes more evident in the advanced stage of microangiopathy, as confirmed by the inverse correlation between FMD values and MES. The lack of statistical difference between early and active NVC patterns might be related to the small sample data (p = 0.10), suggesting that a larger population of patients with SSc should be studied. But if the involvement of conduit arteries was believed to be unusual, in the last 15 years considerable interest has been shown in the hypothesis that patients who have SSc have an increased prevalence of large-vessel disease16,21,22.
Vasodilation and vasoconstriction are dependent upon both intact endothelium and neural control mechanisms23. It is likely that both of these elements are dysfunctional and/or damaged in SSc and that vascular dysregulation is associated with increased risk of vascular disease9. In SSc, the balance between vasodilation and vasoconstriction is disturbed in favor of reduced vasodilation or increased vasoconstriction24. Ultrasound assessment of FMD is an index of macrovascular function and, vicariously, of NO release25. Conflicting data have been reported in SSc regarding abnormal vasodilation (endothelial-dependent and endothelial-independent), but reduced availability of NO is a common feature found in SSc. The significance of this reduced availability was outlined in a review by Herrick2, who reported on endothelial-dependent and endothelial-independent vasodilation in both the dermal microvasculature and large peripheral vessels of patients with SSc. The NO produced by the endothelium acts directly on the vascular smooth muscle, and results in vasodilation26. The endothelial-dependent vasodilation, which is related to an intact endothelium, was found to be compromised in SSc, while the endothelial-independent vasodilation, which does not require a functioning endothelium and evaluates smooth muscle function, is still uncertain17,27. Our data suggest that the vascular dysregulation shown by FMD examination is associated with morphological alterations observed in the different phases of SSc microangiopathy. Although the pathogenesis of microvascular damage progression is not well known, based on our finding of an inverse correlation between FMD and MES, we suggest that the progression into different microangiopathic patterns might be related to the endothelial dysfunction, which is already detected by FMD evaluation in the early phase of microvascular impairment of SSc. The capillary abnormalities that characterize the progression of the SSc microvascular damage (early, active, and late patterns of microangiopathy) do not relate only to endothelial-dependent impairment. Other factors might also be involved.
Our study shows the simultaneous presence of macrovascular and microvascular impairment in patients with SSc that is already detectable in the early phase of the vascular disease and is probably related to a multifaceted derivation that requires further investigation. FMD evaluation might lead to early detection of macrovascular impairment in SSc when the vascular capillary anatomy is still preserved, because NVC detects the microvascular changes that characterize the disease at an early stage28. Further studies are needed to better understand the pathogenetic pathways that are responsible for the composite vascular abnormalities that characterize the multiple aspects of endothelial biology and vascular dysfunction in patients with SSc.
Footnotes
- Accepted for publication February 3, 2010.








{kind=link}
{kind=link}
{kind=link}