

Abstract
Objective. Children often develop arthritis secondary to Lyme disease; however, optimal treatment of Lyme arthritis in pediatric patients remains ill-defined. We sought to characterize the outcomes of a large cohort of children with Lyme arthritis treated using the approach recommended by the American Academy of Pediatrics and the Infectious Diseases Society of America.
Methods. Medical records of patients with Lyme arthritis seen by rheumatologists at a tertiary care children’s hospital from 1997 to 2007 were reviewed. Patients were classified with antibiotic responsive or refractory arthritis based on absence or presence of persisting joint involvement 3 months after antibiotic initiation. Treatment regimens and outcomes in patients with refractory arthritis were analyzed.
Results. Of 99 children with Lyme arthritis, 76 had arthritis that responded fully to antibiotics, while 23 developed refractory arthritis. Most patients with refractory arthritis were successfully treated with nonsteroidal antiinflammatory drugs (6 patients), intraarticular steroid injections (4), or disease-modifying antirheumatic drugs (DMARD) (2). Five were lost to followup. Six patients with refractory arthritis were initially treated elsewhere and received additional antibiotic therapy, with no apparent benefit. Three subsequently required DMARD, while 3 had gradual resolution of arthritis without further therapy. Antibiotic responsiveness could not be predicted from our clinical or laboratory data.
Conclusion. Lyme arthritis in children has an excellent prognosis. More than 75% of referred cases resolved with antibiotic therapy. Of patients with antibiotic refractory arthritis, none in whom followup data were available developed chronic arthritis, joint deformities, or recurrence of infection, supporting current treatment guidelines.
Lyme disease is the most common arthropod-borne infection in the United States. It is particularly common in the endemic regions of the Northeast, Midwest, and Pacific1. Its clinical significance appears to be increasing: between 1992 and 2006, the number of reported cases doubled in the United States2. Lyme arthritis is a well described late manifestation of Lyme disease, characterized by intermittent, recurring, asymmetrical, pauciarticular attacks of joint swelling and pain, persisting for days to months. Lyme arthritis occurs in 50%–60% of untreated patients3,4, with the knee the most commonly affected joint5. Children are more likely to develop arthritis secondary to Lyme disease than adults, and they are more likely to have arthritis as the sole presenting symptom of the disease1.
The outcomes of adult patients treated for Lyme disease with antibiotics are fairly well established. Most cases of Lyme arthritis resolve without sequelae following a single course of doxycycline, amoxicillin, or cefuroxime for 28 days. In approximately 10% of cases, however, arthritis persists despite this treatment, requiring either an additional 28 days of oral antibiotics or intravenous ceftriaxone for 14–28 days, or both6. Of the patients in whom arthritis is persistent, 1%–3% will develop refractory arthritis and continue to have active synovitis despite the additional antibiotic therapy. These patients are often treated with intraarticular steroid injections, surgical synovectomy, or immunomodulating agents, but there remains no well developed treatment protocol to guide the management of this antibiotic-refractory, postinfectious arthritis4.
Management and longterm outcomes of pediatric patients treated for Lyme arthritis similarly are not well defined. Overall, the prognosis of children with Lyme arthritis appears to be good, with most series reporting that 10%–20% of patients recover each year even without specific therapy3. Most do not develop chronic or disabling arthritis, regardless of treatment status3,7,8, although at least one group argued that almost 25% of patients continued to have joint symptoms more than 1 year after treatment9. Complicating interpretation of these studies is that patients in these case series were treated with a variety of interventions, including prolonged courses of antibiotics, disease-modifying antirheumatic agents (DMARD), and surgical synovectomy. Initial antibiotic treatment in pediatric patients with Lyme arthritis is standardized10, but published treatment guidelines for the management of children with persistent Lyme arthritis reflect a broad array of approaches11, based on minimal clinical data. Indeed, the optimal treatment strategy and followup of children with Lyme arthritis remain unclear. Accordingly, we sought to characterize the outcomes of a large cohort of children who were treated for Lyme arthritis using a hierarchical treatment approach.
MATERIALS AND METHODS
Study population
The medical records of all patients seen by the Rheumatology Service at Children’s Hospital Boston for Lyme arthritis between 1997 and 2007 were reviewed. Patients were included in the study if they fulfilled the diagnostic criteria for Lyme arthritis and were given the International Classification of Diseases, 9th Revision, code 711.8. Specifically, arthritis was diagnosed by physician documented presence of one or more joints with effusion, swelling, or at least 2 of 3 other signs of inflammation (warmth, tenderness, or limited range of motion). Lyme arthritis was confirmed when children with arthritis had positive serologic testing for Lyme disease [positive enzyme-linked immunosorbent assay and positive Western blot (at least 5 of 10 IgG bands)]. Other potential causes of arthritis were excluded. Institutional review board approval was obtained for this study.
Treatment regimen
This was a retrospective analysis of all patients treated for Lyme arthritis at Children’s Hospital Boston during the study period. Intervals between various stages of treatment and decisions to use oral or intravenous antibiotics varied depending on individual caregivers’ preferences, and on whether patients were initially treated for Lyme arthritis at the study institution or elsewhere. Those in whom antibiotic treatment was not initiated until after referral were treated and classified according to the antibiotic guidelines recommended by the American Academy of Pediatrics (AAP; Red Book Editions 24–27)10. Some patients were referred to the study center after previous antibiotic therapy. These patients were classified based on the total duration of arthritis and total length of antibiotic therapy. For the purposes of this study, all patients experiencing complete resolution of arthritis within 3 months of initiation of the first antibiotic course, and treated with no more than 4 weeks of intravenous antibiotic therapy or 8 weeks of oral treatment, were classified as having Lyme arthritis responsive to antibiotics7. Patients with physician documented evidence of arthritis (warmth, limited range of motion, tenderness, or elevated laboratory markers of inflammation with effusion) persisting for more than 3 months after initiation of antibiotic therapy were classified as having antibiotic-refractory Lyme arthritis, as described12. The treatment regimens received by these patients after the completion of antibiotics, including nonsteroidal antiinflammatory drugs (NSAID), intraarticular steroids, and DMARD, were then reviewed in detail.
Medical chart review
Records were reviewed for treatment regimen and response to therapy. Information was collected using standardized data collection forms and included the patients’ demographic data, Lyme serologies, arthritis characteristics, laboratory data, treatments, and disease course. When available, studies obtained elsewhere were included in the analysis.
Statistical analysis
We compared categorical data using Fisher’s exact tests and the means of continuous data using Student t tests. Joint count and duration did not follow a normal bell-shaped distribution, as tested by the Kolmogorov-Smirnov statistic. Therefore, responsive and refractory groups for these data were compared by the Mann-Whitney U test and results were described using medians, interquartile ranges, and full ranges. Due to the investigatory design of this study, we used 2-tailed p values < 0.05 to determine significance with no Bonferroni correction.
RESULTS
The medical records of all children seen in the Rheumatology Program between January 1997 and September 2007, both in-clinic and as in- or outpatient consultations, were screened for a diagnosis of Lyme arthritis. A total of 142 patients were considered for this diagnosis and were evaluated for inclusion in the study. Thirty-six received alternative diagnoses and were excluded, including one patient treated for Lyme disease but subsequently diagnosed with spondyloarthritis. Seven more were excluded from statistical analysis because they were lost to followup before their response to antibiotics could be determined.
The remaining 99 patients met criteria for inclusion in this study. Patients ranged in age from 2 to 18 years at the time of diagnosis, and 69% were male (Table 1). Only 6% of subjects reported the presence of erythema migrans, while in 91% arthritis was the presenting symptom leading to the diagnosis of Lyme disease. The median joint count at presentation was 1, most commonly a knee but including the ankles, hips, shoulders, elbows, wrists, and smaller joints of the hand as well. Neurologic involvement was clinically suspected in 3 patients, one of whom had documented facial nerve palsy, but cerebrospinal fluid that was negative for Borrelia burgdorferi by polymerase chain reaction (PCR).
Pretreatment clinical characteristics of patients with Lyme arthritis.
All patients included in the analysis, whether diagnosed with Lyme arthritis at the study center or at the referring institution, were treated initially with antibiotics. The median duration of arthritis prior to initiation of antibiotic therapy was 2 weeks. Initial treatment in 92% of patients was a 28-day course of doxycycline (100 mg orally, twice daily) for those over 8 years of age (43 patients), or amoxicillin (50 mg/kg/day orally, divided into 3 doses) for those less than 8 years old (48 patients). Of the remaining 8 patients, 3 were initially treated with ceftriaxone (75–100 mg/kg/day intravenously once daily) due to an initial diagnosis of septic arthritis (2 cases) or prolongation of symptoms for nearly 1 year (1 case). Three patients were treated with other cephalosporins and 2 were treated with 28 days of an unspecified antibiotic. Twenty-nine patients had persisting arthritis 1–2 months after initiating antibiotic treatment. These patients were given a second 28-day course of oral antibiotics (10 patients), a course of intravenous ceftriaxone (6 patients), or both (13 patients). Six patients were cured following this additional antibiotic therapy and these 76 patients (76.8%) were classified as having antibiotic-responsive arthritis.
Of the overall cohort of 99 patients, 23 (23.2%) had ongoing evidence of synovitis 3 months after starting antibiotics and after completion of 8 weeks of oral antibiotic therapy (8 patients) or 4 weeks of intravenous therapy (4 patients) or both (11 patients). These patients were classified as having antibiotic-refractory arthritis7 (Figure 1). The pretreatment characteristics of antibiotic-responsive and antibiotic-refractory patients were similar (Table 2). Antibiotic-responsive patients tended to be younger (p = 0.09), but no other clinical markers were statistically different. Similarly, the ESR, CRP, serum white blood cell (WBC) and synovial WBC counts were not statistically different, although patients with antibiotic-refractory arthritis did have a higher mean platelet count than antibiotic-responsive patients [405,000 vs 340,000, respectively (p = 0.02)].

Treatment regimen and outcomes for 99 patients with Lyme arthritis. Values in parentheses are number of patients for each group. PO: oral; IV: intravenous.
Pretreatment clinical findings, according to treatment response.
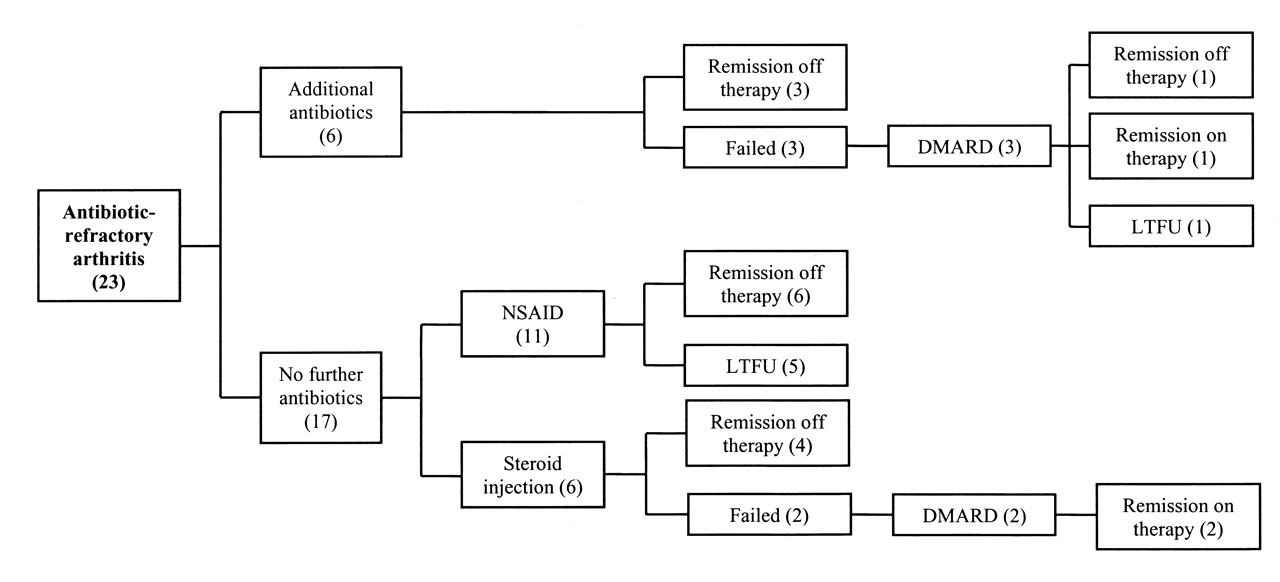
Of the 23 patients with antibiotic-refractory arthritis, 14 were referred to this center after failing at least 1 course of antibiotic therapy. Prior to referral, no patient had been treated for Lyme arthritis with any medications other than antimicrobial agents, apart from occasional doses of analgesics. Six of the patients in the antibiotic-refractory group had received antibiotic medication for a prolonged period of time before they were referred to the study institution. These patients received a total of 5 to 8 months of antibiotic treatment, over the course of 5 to 13 months. In 3 patients, remission off-therapy had ultimately been achieved prior to referral, at 15–56 weeks following initiation of the first course of antibiotics, and these patients required no additional therapy. Three patients continued to have synovitis despite prolonged antibiotic therapy. One was started on methotrexate (MTX) and was in remission on therapy at final followup 9 months later. Another patient received hydroxychloroquine for 8 weeks without benefit, followed by sulfasalazine for 9 months. He was in remission at final followup 1 year later. The remaining patient was treated with sulfasalazine and was lost to followup during therapy (Figure 2).

Treatment regimen and outcomes for 23 patients with antibiotic-refractory Lyme arthritis. Values in parentheses are number of patients for each group. NSAID: nonsteroidal antiinflammatory drugs; LTFU: lost to longterm followup; DMARD: disease-modifying antirheumatic drugs.
The remaining 17 patients were treated without additional antimicrobials, using NSAID, intraarticular steroid injections, or DMARD (Figure 2) as recommended by the Infectious Diseases Society of America (IDSA) guidelines11. Eleven patients were treated with only NSAID and 6 achieved a complete medication-free remission within 6 months. The remaining 5 patients were lost to followup before their effusions resolved. Four of the 6 patients treated with intraarticular steroid injections achieved remission of arthritis without further therapy and the remaining 2 were subsequently treated with DMARD for persistent synovitis. One patient was treated with MTX and was in remission on therapy at final followup 1 year later. Another was treated with 4 months of hydroxychloroquine without benefit, followed by a combination of MTX and leflunomide. At final followup 14 months after the initiation of treatment, his arthritis was quiescent on medications.
Overall, 94% of patients in this study were treated according to the recommendations of the AAP and IDSA guidelines, with no more than two 28-day courses of oral and one 28-day course of intravenous antibiotics10, followed by non-antimicrobial therapy11. Of these patients, 92.5% were cured or in remission off therapy, 2.1% were in remission on therapy, and 5.4% were lost to followup. In the group of patients with antibiotic-refractory arthritis who were treated with only recommended antibiotic therapy, followed by NSAID, intraarticular steroid injections, or DMARD, no patient had continuing symptoms of B. burgdorferi infection, chronic debilitating arthritis, or permanent joint deformities at final followup.
DISCUSSION
We characterized treatment regimens and outcomes achieved in our cohort of pediatric patients with Lyme arthritis. The efficacy of antibiotic therapy for treatment of Lyme disease, specifically tetracyclines and ceftriaxone, has been well established13,14. In a comparison study of adults with Lyme arthritis, 90% of patients treated with doxycycline and 89% treated with amoxicillin plus probenecid had complete resolution of arthritis within 3 months6. Of the remaining 4 patients, 2 were treated with an additional month of oral antibiotic therapy and had resolution of arthritis within 1 year. Two others received intraarticular steroids followed by a course of intravenous ceftriaxone. One of these patients also underwent arthroscopic synovectomy, but full resolution did not occur for up to 4 years after treatment6. In contrast, a more recent series reported that 9 of 24 (38%) patients with Lyme arthritis required intraarticular steroid injections or synoviorthesis to control the arthritis, following at least 14 days of intravenous antibiotics preceded in some cases by 30 days of oral therapy. All ultimately achieved resolution of disease15. This study included only patients that were seen and treated by rheumatologists, and the percentage of refractory cases was therefore likely skewed by referral bias. Our patients were similarly less likely to respond fully to antibiotics. Only 71% of children in our series had resolution of arthritis following the initial course of antibiotics, and further antibiotic therapy achieved full resolution in another 6%. A total of 23% of our patients qualified as having antibiotic-refractory Lyme arthritis. This relatively high antibiotic failure rate likely reflects a bias for referral of refractory cases, since nearly two-thirds of the patients with refractory arthritis had already failed one course of antibiotic therapy prior to presentation at our clinic. While some of the study subjects were children who had readily responded to antibiotics and were referred simply for confirmation of the diagnosis, many such cases likely were not referred to our tertiary care subspecialty clinic. Therefore, we cannot make any conclusions about the overall prevalence of antibiotic-refractory arthritis in this population.
As with other investigators, we did not find any specific predictors of resistance to antibiotics among clinical or laboratory measures12,16, although there was a significantly higher platelet count among patients with refractory arthritis. This finding, however, is not sufficiently specific to be relied upon in clinical practice. The age of the patient also tended to correlate with antibiotic responsiveness, with a trend towards a younger mean age in the antibiotic-responsive group. This is not surprising in view of previously noted correlations between younger age at onset and shorter total duration of arthritis17, and older age and increased likelihood of prolonged or chronic arthritis18. Antibiotics generally were started within 2–3 weeks of the onset of symptoms, and there was no difference between antibiotic-refractory and responsive groups in this regard. There was also no difference between groups in antibiotic use, with amoxicillin being equally as effective as doxycycline for initial therapy, supporting the results of other studies6. Similarly, we found no difference between groups in the use of only oral, versus oral and intravenous antibiotics, for subsequent therapy. The ratio of amoxicillin to doxycycline for initial therapy was slightly higher in the responsive group, but this was likely due to the younger mean age of the patients in this group and the avoidance of tetracycline derivatives in children under 8 years of age.
Other investigators have identified predictors of antibiotic refractoriness, including an increased frequency of certain HLA-DR alleles and antibody reactivity to the B. burgdorferi outer-surface proteins Osp A and Osp B in patients with antibiotic-refractory arthritis or arthritis of prolonged duration19,20. A recent study found that 7 of 14 HLA-DR molecules tested for reactivity bound to Osp A (particularly those alleles associated with rheumatoid arthritis), and patients with antibiotic-refractory arthritis were significantly more likely to have at least 1 of these alleles than patients with responsive arthritis (79% vs 46%, respectively)21. Our patients were not tested for HLA alleles. Most recently, infection with a specific strain of B. burgdorferi (RST 1) has been reported to more commonly lead to refractory arthritis, possibly due to an increased inflammatory response to this strain22. All of these are potential areas for further study.
Our study supports adherence to AAP and IDSA guidelines in the treatment of pediatric patients with Lyme arthritis. Of our 23 patients with ongoing synovitis after antibiotic therapy, 11 were treated only with NSAID. Those patients not lost to followup experienced full relief of symptoms, as reported in other reviews23. Six patients received intraarticular steroid injections following antibiotic therapy, which appeared to be well tolerated and generally effective. While concern has been raised over administering steroid injections to patients prior to antibiotic therapy12, the effectiveness of such treatment in cases of persistent effusions has also been demonstrated6. In our study, two-thirds of the patients who received steroid injections experienced rapid and persisting improvement with no additional therapy. It may be reasonable to consider this treatment more consistently in patients with antibiotic-refractory arthritis.
Two of our patients were treated with DMARD after the recommended courses of antibiotics and steroid injections failed to resolve their arthritis. Previous studies demonstrated the safety and effectiveness of hydroxychloroquine in managing antibiotic-refractory arthritis6,24 and experience has shown that patients given this immune-modifying medication do not develop worsening or recurrent Lyme infections25. Recommendations regarding the use of other, more potent DMARD, however, have been conservative. In our study, hydroxychloroquine was not effective in controlling synovitis in either of the patients who received it, but subsequent treatment with sulfasalazine or MTX plus leflunomide did result in remission. Following treatment with disease modifying agents, none of these patients experienced worsening arthritis or developed any other manifestations of late-stage Lyme disease that would have suggested aggravation of a persistent spirochetal infection.
Most importantly, our findings support previous data that prolonged antibiotic courses do not have a role in the treatment of persistent synovitis following infection with B. burgdorferi, as antibiotic-refractory arthritis is not thought to be due to continuing or persistent infection10,11,26. B. burgdorferi DNA is demonstrable in synovial aspirates prior to antibiotic therapy, but is absent upon repeat testing of patients with persistent arthritis after therapy, indicating eradication of infection27. Rather, the etiology of antibiotic-refractory arthritis likely involves infection-induced autoimmunity inciting persistent synovial inflammation25. Supporting this theory are molecular studies pointing to the presence of different proteins in synovial fluid pre- and post-antibiotic therapy in patients with refractory arthritis28 and describing increased proinflammatory chemokines and cytokines in synovial fluid from these patients29. Recent reports from murine models also support a role for inflammatory cytokines and B cells in persistent disease30. Additionally, cross-reactivity between the Osp A spirochetal epitope and synovial membrane cytokeratin structures has been shown to initiate a T cell inflammatory response31.
We did not routinely perform PCR testing in our patients, but our results nonetheless support the hypothesis that refractory arthritis is not due to persisting infection: our patients treated with immunosuppressive medications, including intraarticular steroids and DMARD, but without additional antibiotics, had full recovery and no findings suggestive of recurrent or persistent B. burgdorferi infection. On the other hand, of the 6 patients treated with prolonged courses of antibiotics, 3 still required treatment with DMARD for resolution of their arthritis. The 3 patients who did achieve remission required 15–56 weeks of additional therapy, longer than the time to remission in the DMARD-treated patients. These 3 cases likely reflect the natural course of the disease, as many cases of persistent arthritis have been shown to gradually resolve without any therapy3,7,8,32. These data suggesting that the immunopathogenesis of acute and persistent Lyme arthritis differ are especially important in view of the risks associated with longterm antibiotic use and, in cases of intravenous treatment, line complications and sepsis12,28,33.
Our results lend support to the management of Lyme arthritis in children in accord with AAP (Red Book) and IDSA guidelines. Our patients were treated with 1 to 2 months of oral antibiotics, with or without an additional month of intravenous therapy. In those patients with persisting arthritis, prolonged antibiotic therapy was not of clear benefit. Instead, our findings support results from others recommending treatment of patients with antibiotic-refractory Lyme arthritis with NSAID, intraarticular steroid injections, or DMARD. These treatments were safe and effective in managing persistent arthritis in our patients. All the children in this study who were treated following this regimen and for whom we have followup data had excellent outcomes, with no evidence of chronic arthritis, permanent joint changes, or breakthrough cases of persistent infection. Thus, while further attempts to optimize the treatment of children with Lyme arthritis are indicated, significant deviations from current treatment recommendations do not appear warranted.
Footnotes
-
Supported in part by the Samara Jan Turkel Center for Pediatric Autoimmune Disease, Boston, Massachusetts.
- Accepted for publication January 2, 2010.








{kind=link}
{kind=link}