

Abstract
Objective. Calprotectin is a calcium-binding cytosolic protein of the neutrophil, monocyte, and macrophage, and its secretion increases during activation of these cells. Our objective was to measure serum calprotectin concentrations in patients with adult-onset Still’s disease (AOSD) and to correlate serum calprotectin with the activity and severity of AOSD.
Methods. We enrolled 25 patients with AOSD and 30 age- and sex-matched healthy controls. Thirty-one serum samples were obtained from patients with AOSD during active or inactive disease and were assayed for calprotectin by ELISA. Clinical and laboratory data related to disease activity and severity were collected at the same time, and systemic scores for disease severity were calculated.
Results. Mean calprotectin levels in patients with AOSD were significantly higher than in controls (57.11 ± 25.38 ng/ml vs 34.90 ± 4.85 ng/ml, respectively; p < 0.05). Patients with active AOSD had a significantly higher mean calprotectin level than those with inactive disease (61.26 ± 25.59 ng/ml vs 35.32 ± 5.90 ng/ml; p < 0.05). Calprotectin levels decreased significantly after treatment in all 6 patients with AOSD from whom followup samples were obtained (p = 0.028). Serum calprotectin showed strong correlations with serum ferritin (r = 0.686, p < 0.001), lactate dehydrogenase (r = 0.647, p < 0.001), leukocyte count (r = 0.774, p < 0.001), aspartate aminotransferase (r = 0.387, p = 0.042), and C-reactive protein (r = 0.588, p = 0.001), but not with erythrocyte sedimentation rate, arginine aminotransferase, hemoglobin, or platelet count. Serum calprotectin showed a significant correlation with AOSD systemic scores, reflecting disease severity (r = 0.803, p < 0.001).
Conclusion. Serum calprotectin increased in patients with AOSD, in close correlation with disease activity and severity. These findings suggest that serum calprotectin can provide a reliable clinical marker for monitoring the disease activity and severity of AOSD.
Calprotectin belongs to the S100 family of calcium-binding cytosolic proteins normally present in regenerative cell types such as neutrophils, monocytes, macrophages, and endothelial and epithelial cells1. In neutrophils, monocytes, and activated macrophages, calprotectin constitutes 40% to 60% of the soluble cytosolic proteins, which suggests a specific function1,2. Although this function is not clearly defined, it may involve modulation of inflammatory and antimicrobial activities and calcium-dependent regulation of protein phosphorylation, transcription, and enzyme activities3,4. Calprotectin concentrations rise at the site of local inflammation following its release from activated and dying cells2. Calprotectin released from activated monocytes binds to endothelial cells and modulates transendothelial leukocyte migration5. Evidence for these mechanisms has prompted several studies dealing with calprotectin in inflammatory disease. Patients with ulcerative colitis and Crohn’s disease have increased calprotectin concentrations in serum, feces, and intestinal mucosa6–8. In patients with rheumatoid arthritis (RA), this protein is detected in the inflamed synovium and is elevated in plasma and synovial fluid from affected joints2,9. As a relatively low molecular-weight protein (36.5 kDa), calprotectin diffuses freely from inflamed tissues into circulation2 and can be accurately measured in plasma.
Adult-onset Still’s disease (AOSD) is a systemic inflammatory disorder characterized by high spiking fever, evanescent rash, arthralgia or arthritis, hepatosplenomegaly, and laboratory abnormalities including neutrophilic leukocytosis, abnormal liver function tests and increased ferritinemia10. Although AOSD is rare and usually self-limiting, more than one-third of patients develop chronic disease with a poor prognosis10,11, with complications such as pericarditis, cardiac tamponade, disseminated intravascular coagulation, and hepatic and respiratory failure leading ultimately to death10,12,13. Effective treatment of AOSD therefore requires accurate determination of disease activity and severity. Markers in current use include acute-phase indicators such as erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and serum ferritin. But these markers lack the sensitivity, specificity and precision required to monitor the disease. Although the pathogenesis of AOSD is not clearly understood, evidence indicates important roles for monocytes and macrophages through secretion of proinflammatory cytokines such as interleukin 1ß (IL-1ß), IL-6, IL-18, and tumor necrosis factor-α (TNF-α)10,14,15. The pathologies of Still’s rash and synovial tissue also support the role of inflammatory signaling in AOSD. We hypothesized that serum levels of calprotectin would be increased, in conjunction with disease activity and severity, in patients with AOSD. The aims of our study were to determine the serum concentrations of calprotectin in patients with AOSD and to investigate their correlations with disease activity and severity of AOSD.
MATERIALS AND METHODS
Study subjects and samples
This study included 25 Korean patients with AOSD (21 women, 4 men; mean age 37.1 ± 15.3 yrs) and 30 age- and sex-matched healthy controls (24 women, 6 men; mean age 36.1 ± 10.2 yrs). AOSD patients were diagnosed according to the criteria of Yamaguchi, et al16. All study subjects were seen at Severance Hospital, Yonsei University College of Medicine, Seoul, from December 1998 to January 2006. We excluded patients who had an infection, trauma, neoplasm, or any other condition potentially requiring surgery in order to minimize confounding effects on serum calprotectin. Blood samples were obtained from patients and controls. Of the 25 AOSD patients, 21 were in an untreated active disease state at the time of sampling, and followup samples were obtained from 6 patients after treatment. The other 4 patients were in a treated inactive state at the time of sampling. Samples were immediately centrifuged and the upper third of serum was stored at −70°C until analysis. The Institutional Review Board of Severance Hospital approved this study.
Clinical and laboratory assessment
Detailed clinical and laboratory data were collected at the time of serum sampling. To evaluate systemic AOSD severity, we used the method described by Pouchot, et al17, which assigns a score from 0 to 12 and adds 1 point for each of the following manifestations: fever, typical rash, pleuritis, pneumonia, pericarditis, hepatomegaly or abnormal liver function tests, splenomegaly, lymphadenopathy, leukocytosis ≥ 15,000/mm3, sore throat, myalgia, and abdominal pain. We also obtained conventional markers for disease activity, including white blood cell (WBC) count, ESR, CRP, lactate dehydrogenase (LDH), and serum ferritin levels to test their correlations with calprotectin.
Measurement of calprotectin concentrations
Serum concentrations of calprotectin were quantified using a commercial enzyme-linked immunosorbent assay (ELISA) kit (Hycult biotechnology, Uden, The Netherlands) according to the manufacturer’s protocol. Each 100-μl sample of serum or standard was placed in a microtiter plate well coated with a monoclonal antibody to human calprotectin heterodimer. After incubation for 1 h at room temperature, the wells were washed 4 times with buffer, and samples were labeled with 100 μl of dilute tracer (biotinylated secondary antibody to human calprotectin). After washing again, each well received 100 μl of diluted streptavidin-peroxidase conjugate, which reacts specifically with the calprotectin-bound tracer. After incubation at room temperature for 1 h, excess conjugate was removed by washing, and tetramethylbenzidine substrate solution (100 μl) was applied to each well for 30 min in the dark at room temperature. To terminate the reaction, stop solution containing citric acid (100 μl) was added to each well, and absorbances were measured at 450 nm using an ELISA plate reader (Tecan, Saint-Julie, PQ, Canada). The coefficient of variation for duplicate measurements using ELISA was < 6%.
Statistical analysis
All statistical analyses were performed using SPSS for Windows, version 11.5 (SPSS Inc., Chicago, IL, USA). Results are presented as the mean ± standard deviation, and all biochemical data represent duplicate measurements. The results were analyzed by independent t tests, Mann-Whitney U test, and chi-square tests as appropriate. The correlations between serum calprotectin level and disease-related variables were evaluated using Spearman’s correlation test. The Wilcoxon signed-rank test was also used to compare calprotectin levels before and after treatment. A p value < 0.05 was considered statistically significant.
RESULTS
Characteristics of subjects
Subjects’ baseline characteristics are summarized in Table 1. Mean ages and male-female ratio did not differ between patients and controls. Fever, salmon-colored rash, arthritis, sore throat, myalgia, hepatosplenomegaly, lymphadenopathy, pleuritis, pericarditis, pneumonitis, and abdominal pain were found in 21 (84%), 17 (68%), 16 (64%), 3 (12%), 15 (60%), 6 (24%), 3 (12%), 3 (12%), 1 (4%), 2 (8%) and 4 (16%) patients with AOSD, respectively. Twenty-one patients with active AOSD (84%) did not receive any treatment initially, and of these, 6 patients (24%) were treated with methylprednisolone pulse therapy or moderate- to high-dose corticosteroids and immunosuppressive agents such as azathioprine, methotrexate, or cyclosporine at the time of followup sampling. Four inactive patients (16%) were maintained with low-dose corticosteroid (prednisolone ≤ 15 mg/day).
Baseline characteristics of patients with adult-onset Still’s disease and controls.
Serum calprotectin levels in patients and controls
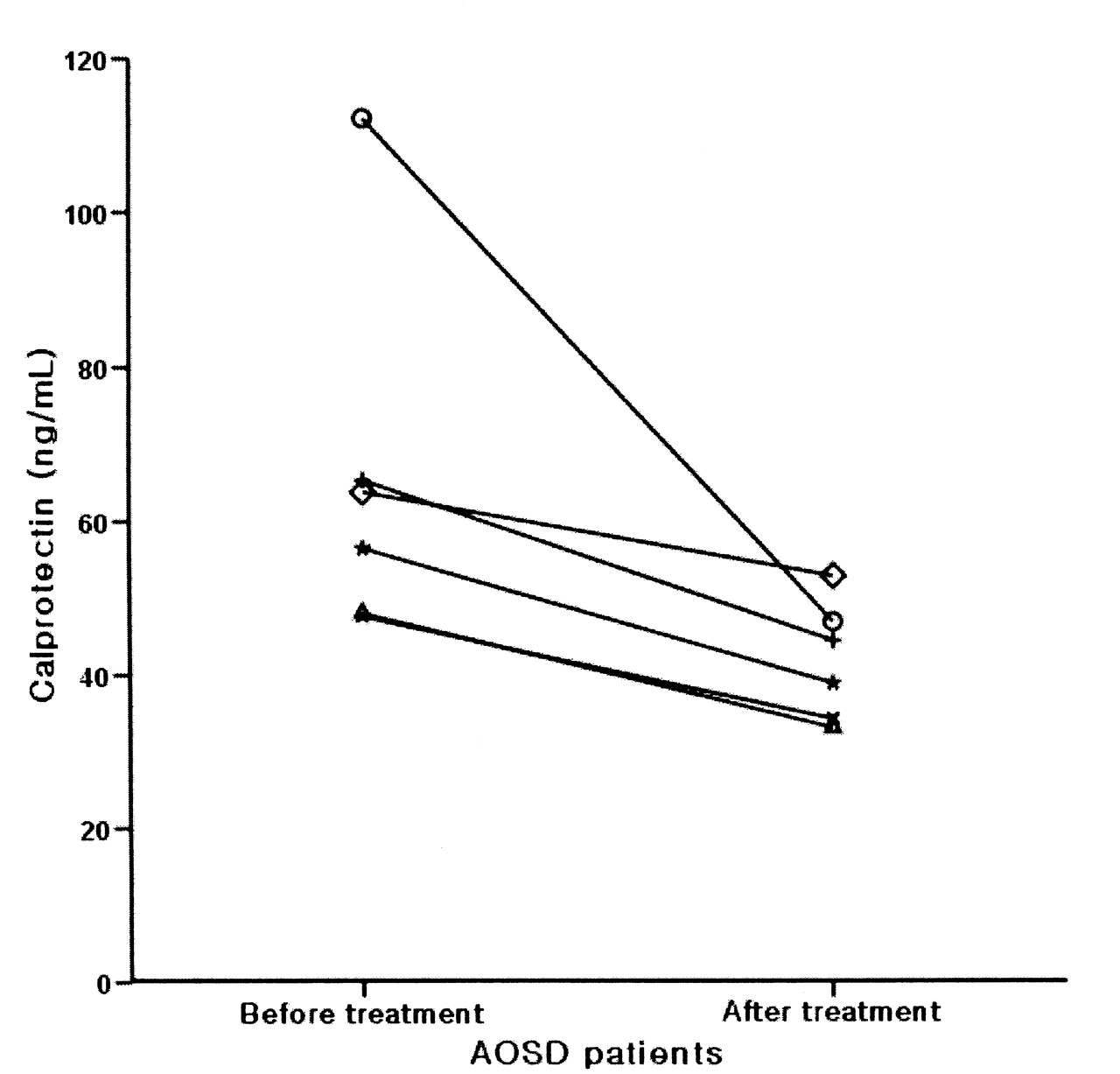
Patients with AOSD had a significantly higher mean calprotectin level than the controls (57.11 ± 25.38 ng/ml vs 34.90 ± 4.85 ng/ml, respectively; p < 0.05; Figure 1A). Patients with active AOSD had a significantly higher mean calprotectin level than did those with inactive disease (61.26 ± 25.59 ng/ml vs 35.32 ± 5.90 ng/ml; p < 0.05), but patients with inactive AOSD and the controls had no significant difference in mean calprotectin level (Figure 1B). Serum calprotectin levels decreased significantly after treatment in all 6 patients with AOSD who had followup evaluations (p = 0.028; Figure 2).

Calprotectin levels in AOSD patients and controls. A. Mean calprotectin level of patients was significantly higher than controls (57.11 ± 25.38 ng/ml vs 34.90 ± 4.85 ng/ml; p < 0.05). B. Patients with active AOSD had a significantly higher mean calprotectin level than patients with inactive disease (61.26 ± 25.59 ng/ml vs 35.32 ± 5.90 ng/ml; p < 0.05), but patients with inactive AOSD and controls had no significant difference in the mean calprotectin level. Horizontal bars represent mean values.

Calprotectin levels before and after treatment in 6 patients with AOSD. Levels decreased significantly after treatment (p = 0.028).
Correlation between serum calprotectin and disease activity
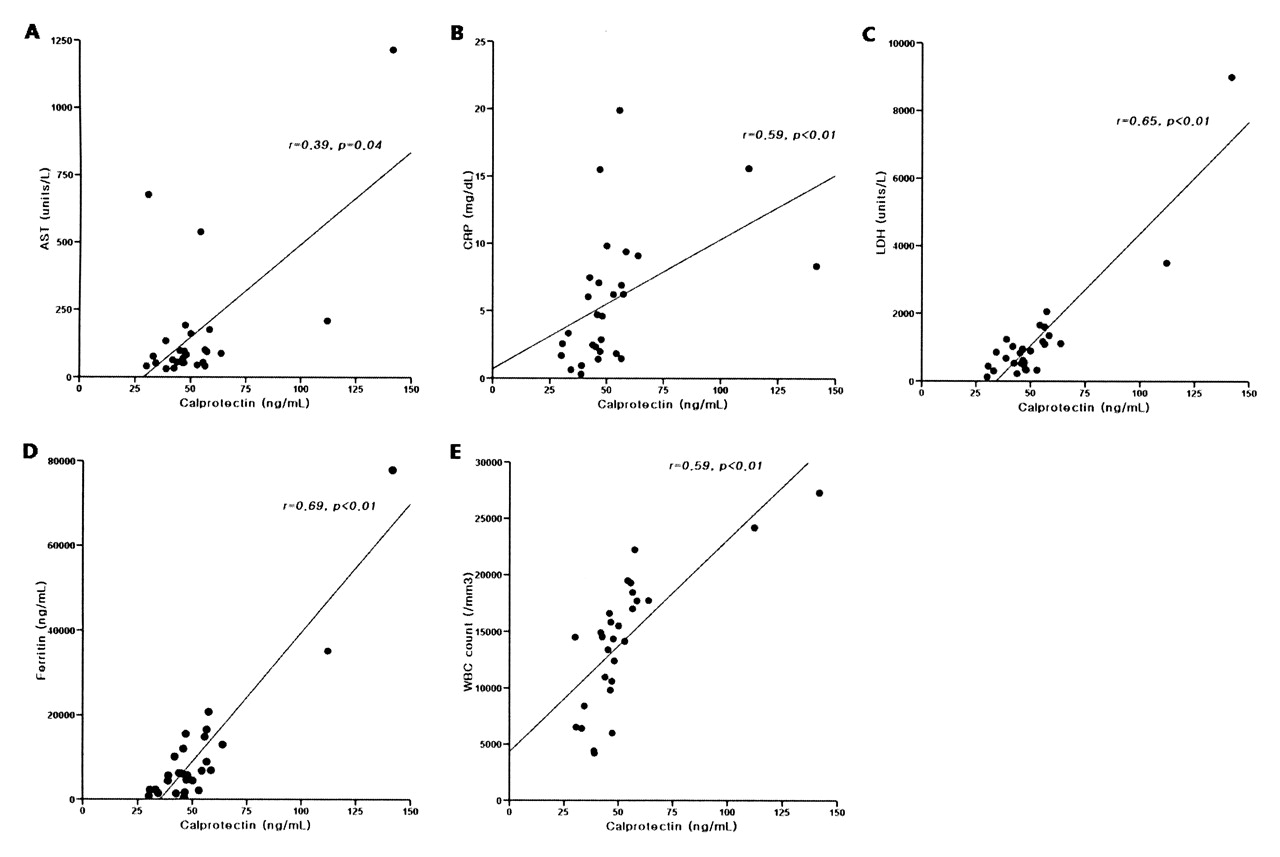
Serum calprotectin levels showed strong correlations with aspartate aminotransferase (AST; r = 0.387, p = 0.042; Figure 3A), CRP (r = 0.588, p = 0.001; Figure 3B), LDH (r = 0.647, p < 0.001; Figure 3C), serum ferritin (r = 0.686, p < 0.001; Figure 3D), and WBC count (r = 0.774, p < 0.001; Figure 3E). Calprotectin did not correlate significantly with ESR, arginine aminotransferase, hemoglobin, or platelet count.

Correlations of calprotectin levels with AST, LDH, WBC count, CRP, and ferritin levels. Serum calprotectin levels showed strong correlations with AST (A: r = 0.387, p = 0.042), CRP (B: r = 0.588, p = 0.001), LDH (C: r = 0.647, p < 0.001), serum ferritin level (D: r = 0.686, p < 0.001), and WBC count (E: r = 0.774, p < 0.001).
Correlation between serum calprotectin and disease severity
The mean systemic score in patients with AOSD was 4.79 ± 1.67 points (range 2–8). Serum calprotectin showed a significant correlation with the AOSD systemic score, which reflects disease severity (r = 0.803, p < 0.001; Figure 4). Individual variables of the AOSD systemic score did not correlate significantly with serum calprotectin.

Association between calprotectin levels and systemic scores in patients with AOSD. Calprotectin levels showed significant correlations with AOSD systemic score, reflecting disease severity (r = 0.803, p < 0.001).
DISCUSSION
Specific serologic markers are urgently needed to diagnose and assess disease activity in AOSD. A subgroup of patients will develop a progressive disease with high risk for disability or death, and close monitoring will help to facilitate prompt and effective treatment. Markers proposed for AOSD activity and/or severity include serum soluble intracellular adhesion molecule-1 (sICAM-1)11, macrophage migration inhibitory factor (MIF)18, and IL-6 and IL-1814,19,20. These markers, however, have limited clinical utility. Serum ferritin has to date provided the most useful indication of AOSD activity10, but this acute-phase reactant may also increase during an infection or nonspecific inflammation and can be affected by iron concentration in the body. The search for disease-specific markers for AOSD therefore continues.
Various types of cells produce the calcium-binding cytosolic protein calprotectin, which participates in intracytoplasmic secondary signal transduction1,3. In an inflammatory response, activated macrophages and neutrophils secrete significant quantities of calprotectin, which in diseases such as Crohn’s disease, ulcerative colitis, acute pancreatitis, cystic fibrosis, and bacterial pneumonia can be detected in the serum, urine, or feces6–8,21–23. Calprotectin secretion is also associated with RA, systemic lupus erythematosus, juvenile idiopathic arthritis, and gout2,9,24–28. Particularly in patients with RA, calprotectin levels increase in the serum and synovial fluid and show a close correlation with the severity of joint damage2. Calprotectin may therefore provide a reliable measure of inflammatory activity.
We have searched for AOSD-specific serologic markers. We know that this disease involves the activation of macrophages, lymphocytes, and neutrophils, triggered perhaps by exogenous factors, and that proinflammatory cytokines such as IL-1, IL-6, IL-18 and TNF-α also contribute. This led us to consider that calprotectin secretion may increase with disease activity.
In our study, serum calprotectin levels were higher in AOSD patients than in controls and were significantly higher during active disease than in the inactive stage. The levels decreased significantly after treatment in all 6 patients with AOSD from whom followup samples were available. Hence serum calprotectin may potentially be used to monitor treatment responses.
We tested associations between serum calprotectin and conventional markers of AOSD activity, including serum ferritin, LDH, AST, arginine aminotransferase, ESR, and CRP. Although these lack precision, they represent the markers clinically available. In our study, serum calprotectin levels showed significant correlations with serum ferritin, LDH, AST, WBC count, and CRP. The very close association with serum ferritin suggests that these 2 indicators together may provide an especially robust marker for disease activity. Interestingly, serum calprotectin showed a higher correlation with WBC count than with other markers, probably because calprotectins are secreted from leukocytes.
Using the systemic score for AOSD activity proposed by Pouchot, et al17, we found a significant positive correlation of calprotectin with clinical symptoms. Evidence supports a role for calprotectin in the transendothelial migration of inflammatory cells5, which implies its involvement in synovium, pleura, lymph node, or liver. Thus, we may interpret newly rising levels of serum calprotectin to indicate the onset or perpetuation of a clinical manifestation.
Our study was limited by the small number of patients, which reflects the low incidence of AOSD. A larger future study will more accurately reveal the changes in calprotectin that accompany disease activation, remission, and treatment.
Serum calprotectin levels increased in patients with AOSD, in correlation with disease activity and severity. Serum calprotectin may therefore provide a reliable clinical monitoring tool for AOSD.
Footnotes
- Accepted for publication December 19, 2009.








{kind=link}
{kind=link}
{kind=link}
{kind=link}